My definition of comprehensive is 100% recovery protocols. Anything less and you don't even have a stroke hospital.
A comprehensive neurorehabilitation program should be an integral part of a comprehensive stroke center
 Reza Bagherpour1,2,
Reza Bagherpour1,2,
 Dennis D. Dykstra
Dennis D. Dykstra A. M. Barrett
A. M. Barrett Andreas R. Luft
Andreas R. Luft Afshin A. Divani
Afshin A. Divani- 1Department of Physical Medicine and Rehabilitation, University of Minnesota, Minneapolis, MN, USA
- 2Department of Neurology, University of Minnesota, Minneapolis, MN, USA
- 3Stroke Rehabilitation Research, Kessler Foundation, West Orange, NJ, USA
- 4Clinical Neurorehabilitation, Department of Neurology, University of Zurich, Zurich, Switzerland
- 5Department of Neurosurgery, University of Minnesota, Minneapolis, MN, USA
Introduction
With the aging population, strokes have become a leading cause of disability and cognitive impairment. On average, someone has a stroke every 40 s in the United States, resulting in approximately 800,000 strokes annually (1, 2). As a result, acute management of stroke volume has increased in order to meet the demand. This includes initial assessment, diagnostic imaging, laboratory studies, and appropriate acute treatments (3).
Forty percent of stroke survivors experience moderate to severe impairments requiring specialized care (4), while about 10% will require long-term care or placement in a skilled nursing facility (5). Furthermore, even minor strokes are associated with memory, spatial, and mood disorders as well as other hidden disabilities (6). Morbidity from stroke remains high despite new advances in treatment of acute stroke with thrombolytic agents and endovascular approaches (1). Therefore, protocols for appropriate triage and referral at all care stages may need to be centralized. An ideal setting for implementing systematic care protocols is a comprehensive stroke center (CSC).
Integrating Neurorehabilitation Service in CSCs
Although CSCs treat acute stroke patients more effectively (7), we feel that a critical part of the management process is often overlooked by the lack of emphasis on neurorehabilitation.(You're absolutely right, you have not done one damn thing on 100% recovery protocols. When are you going to do that?) As a result, delay in initiation of pathways for evidence-based and targeted rehabilitation care can occur, even in these specialized settings.
The ideal way to integrate neurorehabilitation services in CSCs is to base recommendations on quality improvement studies that have demonstrated how to manage referral protocols to optimize rehabilitation outcomes. For example, studies examining the impact of referring patients for rehabilitation during the first days of admission vs. those referred at discharge can be used to create quality standards for internal and external monitoring. Unfortunately, studies comparing rehabilitation outcomes with different rehabilitation care referral procedures are not yet available. CSCs are ideal settings for examining differences in outcome based on systems of care, and thus we urge stroke researchers to begin evaluating and comparing rehabilitation referral pathways. However, until evidence-based protocols for rehabilitation are available, true quality monitoring in the CSC setting needs to be based on the best-practice standards.
Psychological care is an integral part of all neurorehabilitation programs, due to the fact that stroke patients are at high risk of depression (8, 9). Integrating rehabilitation into a CSC will facilitate psychological and psychiatric evaluation of all stroke patients (10).
Benefits of Availability of Neurorehabilitation Service in CSCs
The presence of neurorehabilitation services in designated CSCs can allow for the continuity of care from physiatrists, neurologists, rehabilitation nurses, physical and occupational therapists, speech-language pathologists, dieticians, social workers, neuropsychologists, case managers, and recreational therapists as part of the experienced and specialized interdisciplinary team paying careful attention to neurorehabilitation. With a more systematically integrated assessment of progress, including attention to psychosocial issues and early comprehensive discharge planning, this model for stroke-care not only potentially improves patient outcomes, but also decreases the financial burden on the medical care system and improves hospital–home transitions.
Rehabilitation should begin in the hospital, as soon as possible, following the stroke. Any rehabilitation program should aim to improve function by allowing stroke survivors to operate as independently as possible (11). Stroke sequelae invariably include both neurological impairments and related functional disabilities (12–14). Early spontaneous neurological recovery is dependent on local processes leading to initial clinical improvement independent of behavior or stimuli. Functional recovery is influenced by both rehabilitation interventions and spontaneous neurological recovery. Therefore, an effective neurorehabilitation regimen can be extremely beneficial to both types of recovery.
Since peak neurological recovery occurs within the first 3 months of the initial insult (15) and large numbers of stroke survivors may not be able to access outpatient treatment (16), it is essential to expeditiously incorporate a comprehensive neurorehabilitation regimen as part of any universal stroke treatment curriculum. Neurological reorganization plays an important role in this restoration of function. It can extend for a much longer period than local processes, such as the resolution of edema or reperfusion of the penumbra. Of particular interest is the influence of rehabilitation training on neurological reorganization. For example, motor imagery neurorehabilitation techniques that have long been used for athletic improvement (17) are a feasible treatment for patients with sensory-motor impairments following a stroke, and may also support sensory-motor reorganization to prepare for the return of function (18). Techniques such as these might be used early in the recovery period while reorganization is concurrently taking place (19).
Another major advantage of involving rehabilitation in CSCs is to initiate a robust rehabilitation care pathway that includes post-acute, home-based and chronic components, patient and family education, and lifestyle adjustments (see Table 1). A large number of stroke survivors can benefit from inpatient acute rehabilitation in hospitals that provide a full range of rehabilitation services combined with skilled nursing staff. These are generally the only settings where subspecialty rehabilitation providers and intensive treatments are available.
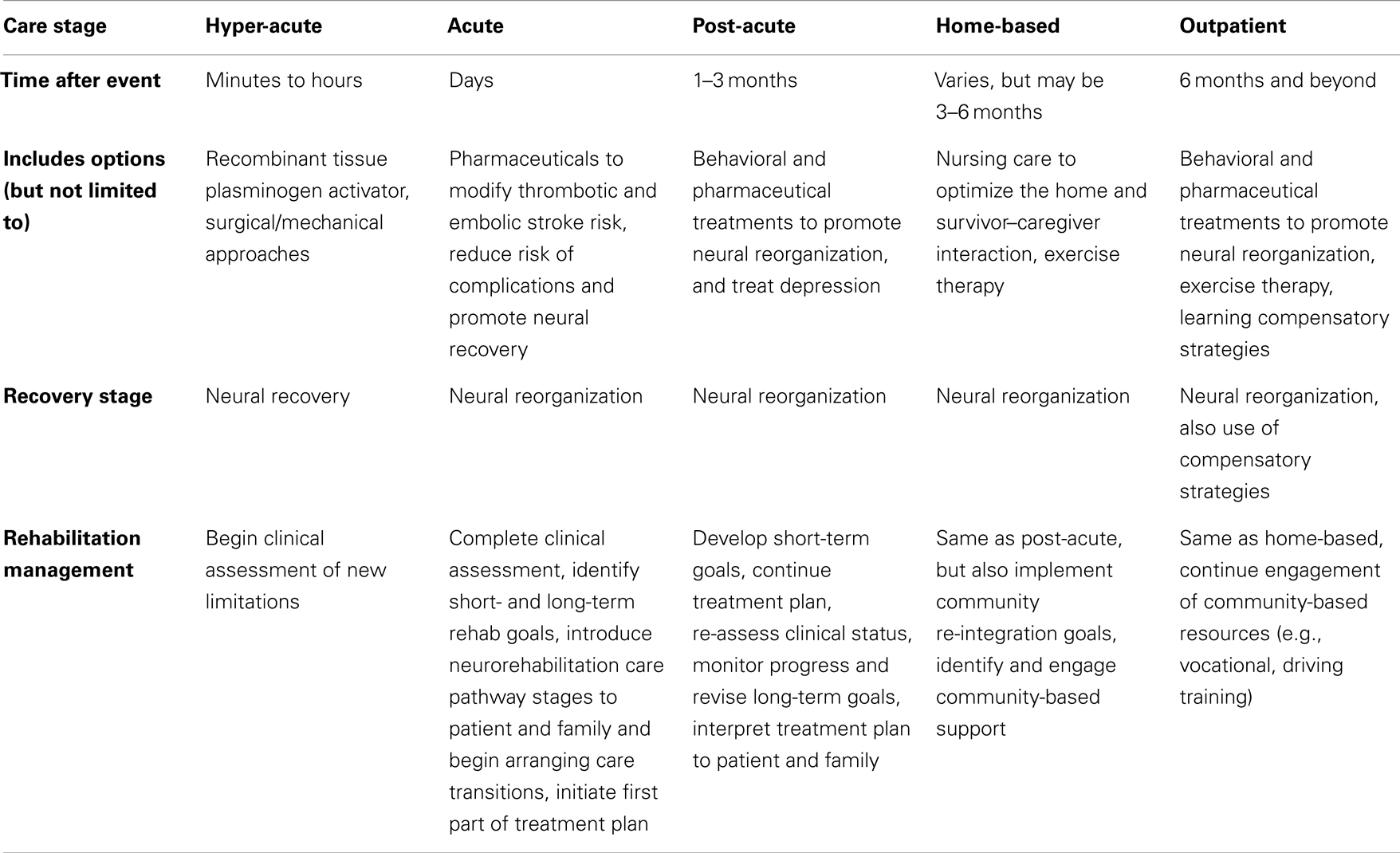
Table 1. Brief outline of care pathway for neurorehabilitation after stroke, Adapted from Ref. (20, 21).
Long-term care facilities, home therapy through visiting nursing staff, day programs, and outpatient therapy are all viable options for the next stage of recovery, which may continue for years, albeit at a less rapid rate. As opposed to daily rehabilitation offered in acute inpatient facilities, other facilities offer rehabilitation services two to three times per week to optimize activity of daily living to prevent decline in functional ability and performance. As part of the transition to the community, access to appropriate support services (vocational counseling, peer advocacy, and social support organizations) is extremely important.
Because current stroke-care frequently involves a delay in initiating intensive acute inpatient rehabilitation, starting these services within a CSC, to continue in another sub-acute setting, may be optimal for qualifying patients (22). As these acute services may favorably modify motor, communication, or other recovery trajectory, we can expect that (faster) patient recovery to baseline functional status will result in significant reduction in healthcare costs.
More at link.
No comments:
Post a Comment