What crapola. 'Monitoring'. Nothing here is going to get any survivor recovered. Useless. Oh we will monitor you, but we have NO STROKE PROTOCOLS to get you recovered. Hope you are happy with our services.
Muscle Activity After Stroke: Perspectives on Deploying Surface Electromyography in Acute Care
 Katherine M. Steele
Katherine M. Steele Christina Papazian
Christina Papazian Heather A. Feldner
Heather A. Feldner- 1Department of Mechanical Engineering, University of Washington, Seattle, WA, United States
- 2Department of Rehabilitation Medicine, University of Washington, Seattle, WA, United States
After a stroke, clinicians and patients struggle to determine if and when muscle activity and movement will return. Surface electromyography (EMG) provides a non-invasive window into the nervous system that can be used to monitor muscle activity, but is rarely used in acute care. In this perspective paper, we share our experiences deploying EMG in the clinic to monitor stroke survivors. Our experiences have demonstrated that deploying EMG in acute care is both feasible and useful. We found that current technology can be used to comfortably and non-obtrusively monitor muscle activity, even for patients with no detectable muscle activity by traditional clinical assessments. Monitoring with EMG may help clinicians quantify muscle activity, track recovery, and inform rehabilitation. With further research, we perceive opportunities in using EMG to inform prognosis, enable biofeedback training, and provide metrics necessary for supporting and justifying care. To leverage these opportunities, we have identified important technical challenges and clinical barriers that need to be addressed. Affordable wireless EMG system that can provide high-quality data with comfortable, secure interfaces that can be worn for extended periods are needed. Data from these systems need to be quickly and automatically processed to create round-ready results that can be easily interpreted and used by the clinical team. We believe these challenges can be addressed by integrating and improving current methods and technology. Deploying EMG in the clinic can open new pathways to understanding and improving muscle activity and recovery for individuals with neurologic injury in acute care and beyond.
Introduction
Every brain injury is unique—making individualized evaluations especially important for diagnosis and prognosis. For individuals who have had a stroke, impaired movement is one of the most persistent and disabling sequela, severely limiting participation, and quality of life (1–3). Many individuals initially have limited or no ability to move their limbs after stroke. However, determining when and if an individual will regain movement is challenging (4–6). Surface electromyography (EMG) provides a non-invasive window to observe neuromotor activity. By monitoring activity and observing resulting movements, we can evaluate the integrity of neuromotor pathways (7). The initial weeks after stroke are viewed as a critical period of neural plasticity and recovery (8), yet EMG is rarely deployed during this time.
In acute care, function-based clinical exams remain the standard for evaluating and monitoring muscle activity and movement. The Manual Muscle Test (MMT) and NIH Stroke Scale (NIHSS) are among the most common evaluation measures used in the United States. These measures are often performed daily in the hospital to track recovery and document outcomes for insurance purposes. Clinicians conduct these measures by asking individuals to attempt to voluntarily move specific body parts, assigning an ordinal score based upon observed movement or muscle activity felt by palpation (9–12). Members of the care team can conduct these exams quickly, but they are coarse measures that provide limited insight into the extent of injury or prognosis, especially for individuals with language barriers, receptive aphasia, neglect, or other impairments that limit ability to follow instructions. The Fugl-Meyer Assessment (FMA) expands the repertoire of movements to evaluate synergistic or other inappropriate muscle activity (13, 14). While the FMA has shown promise for predicting recovery and future function (15), it is not often used in the clinic due to the time and training required. Like the MMT and NIH Stroke Scale, it also has limited utility for individuals with impaired voluntary movement or difficulty following instructions. An ideal assessment tool to monitor muscle activity and movement after stroke would provide deeper insight into the quantity and quality of movement, while requiring minimal time to execute.
In the 1950s, clinicians like Thomas Twitchell deployed EMG to monitor muscle activity (16–19), but today EMG is mainly confined to research settings. Twitchell's detailed observations of EMG recordings from stroke survivors in acute care remain some of our most detailed descriptions of early muscle activity after stroke. Twitchell would not recognize today's sophisticated EMG systems (20). Large sensors and tangles of wires have been replaced by sleek, small packages that wirelessly transmit data from dry electrodes that make it easier to target and isolate activity from individual muscles. Material selection and electrode design continue to improve, such that EMG sensors can even be worn for multiple days with minimal impact on signal quality or skin health (21–23). One of the largest changes has come in our processing and analytic ability. We have replaced the chart recorders that Twitchell used with systems that easily capture and analyze recordings (24, 25). EMG sensors can also be integrated with other sensors, such as inertial measurement units (IMUs) that provide concurrent measurements of movement.
Despite all of the opportunities provided by this advancement, the translation of EMG to clinical care has been a slow process. In this paper, we share our team's perspective translating EMG into the clinic through a multidisciplinary collaboration between engineers and clinicians. Over the past two years, we have monitored muscle activity with adult stroke survivors within the first 5 days after stroke. This experience has shown our team that there are great opportunities in expanding the use of EMG in clinical care, but significant barriers that need to be overcome to facilitate this translation. We hope our experiences and lessons learned can support other teams attempting this translation and accelerate the use of EMG technology to advance care.
Surface EMG In Acute Care
“I think my finger moved today” is a phrase that many clinicians in acute stroke care or rehabilitation have heard from a stroke survivor. During the early weeks, movement can return rapidly and seemingly unexpectedly, which makes every twitch or sensation a potential positive sign (19). Clinicians and their patients often cannot definitively determine whether an individual voluntarily moved their arm or finger, or if there were changes compared to yesterday (26, 27). While a clinician cannot wait by the bedside, an EMG system can unobtrusively monitor muscle activity while the patient and clinical team continue with standard care. Of course, the acute setting presents unique challenges in deploying any technology (28). Large care teams work around the clock to coordinate and conduct numerous tests and procedures to address the initial injury and prevent further damage.
In our work to deploy EMG in this challenging environment, our team prioritized selecting an EMG system that provided wireless sensing in a compact form. The BioStampRC sensors (BioStampRC, MC10, Lexington, MA) included integrated EMG and accelerometer sensors that could concurrently monitor muscle activity and movement. We targeted the muscles most commonly assessed by the clinical team, placing sensors on five muscle groups: the deltoid, biceps, triceps, wrist flexors, and wrist extensors of the affected upper extremity (Figure 1). We followed SENIAM guidelines for placing the sensors, but often had to adjust to accommodate IV's, bandages, or telemetry pads. Loose skin, adipose tissue, and sweat were also common issues that impacted signal quality and sensor adherence.
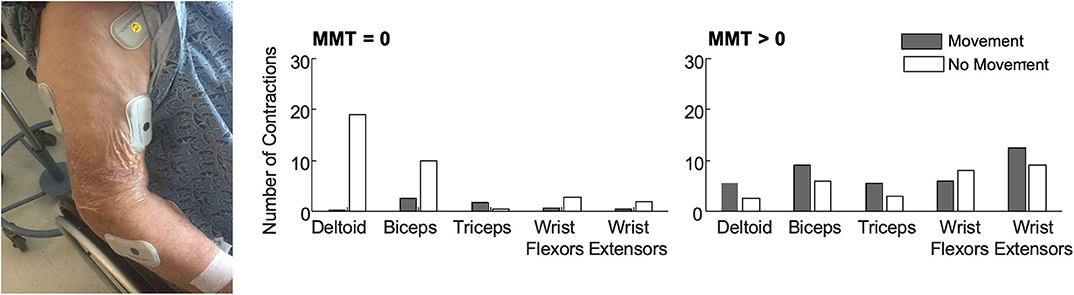
Figure 1. (Left) BioStamp sensors provided a wireless and low-profile sensor to monitor muscle activity. We monitored muscle activity from five muscle groups on the paretic arm—the deltoid, biceps, triceps, wrist extensors, and wrist flexors. Tegaderm and Coband were placed over the electrodes to ensure they did not fall off or get stuck to bed sheets during 4 h of monitoring. The EMG data were used to evaluate outcome metrics like the median number of contractions (per 30-min of analyzed data) among patients with no observable muscle activity (N = 11, MMT = 0) and patients with some residual muscle activity (N = 10, MMT > 0). Accelerometer data were used to classify each contraction as occurring during periods with or without movement. (Right) Median number of contractions identified for each muscle with and without movement. Importantly, contractions were identified for all five muscles in all patients. For participants with MMT > 0, contractions were identified in all five muscles in a single 30-min monitoring session. Up to 3 h of monitoring was required to detect contractions in all five muscles for the participants with MMT = 0. As expected, participants with MMT > 0 had more contractions with movement. For participants with MMT = 0, contractions during movement likely reflect times when their arm was being moved during care. Participants with MMT = 0 also had more contractions in proximal muscle groups.
We deployed these sensors with stroke survivors who demonstrated impaired arm movement (NIHSS > 1) at a level-one trauma hospital. Patients were excluded if they were on comfort care, but otherwise we had broad inclusion as our main goal was evaluating deployment of the technology and observing muscle activity of all stroke survivors. We recruited patients from the acute stroke unit, where some patients may have received initial care in the intensive care unit. At this hospital, most stroke survivors stay in acute care for <2 weeks, receiving daily evaluations and therapy, before being discharged to inpatient rehabilitation, a skilled nursing facility, or their home. Our primary objective was to evaluate whether muscle activity could be detected during acute stroke care. We were especially interested in determining whether EMG sensors could detect muscle activity for those patients classified as having dense hemiplegia or flaccidity, who could not participate or be evaluated with other clinical measures. For each patient, we collected up to four hours of data. We manually identified contractions for each muscle, marking the start and stop time and coding each contraction as during periods of movement or rest based upon concurrent accelerometer data. Details on the data collection, EMG processing, and analyses can be found in (29, 30) and (REF), while here we aim to share key experiences in deploying this technology.
For the patients we monitored, muscle contractions were detected from all five muscles during a single four hour collection period during standard care (Figure 1). This was true even for the patients who had an MMT score of zero (N = 11), indicating no voluntary movement or muscle activity detected via palpation. For the participants with an MMT >0 (N = 10), only a single 30-min time window was required to identify contractions in all five muscles. For the patients who were initially flaccid, we did find moderate correlations between early contraction characteristics and scores on the MMT at follow-up. These findings indicate that muscle activity is present during the first week after stroke, even among participants characterized as flaccid, and EMG can provide quantitative metrics that may have prognostic value for predicting future function.
No comments:
Post a Comment