Our stroke leaders have no clue as to why stroke has fallen in the US from 3rd to 4th to 5th most deadly disease. This would be an excellent way to find out if we had anybody in our stroke associations that have two neurons to rub together. But I can guarantee that our stroke associations will fail miserably once again. And their boards of directors must be ok with such f*cking failure because they allow it to continue.
Possible Explanations
While it’s too early to know exactly why the stroke numbers went down,
interventions like the clot-buster tPA likely are a factor, Lackland
said.
“We know that management of blood pressure has a major impact here yet
only 50 percent of people with high blood pressure have it under
control,” he said.
According to Lackland, stroke deaths, stroke incidence, and recurrent strokes are all on the decline.
So they really know nothing.
Seeing a pattern
Joseph Budner Elad has sought patterns in roadside bombings in war, and the path of deadly pathogens.
Now, Elad, president and CEO of Quantum Leap Innovations of Newark,
has begun putting his company’s pattern-seeking technology to more
everyday use for business.
For instance, the software can examine whether patients who get
readmitted to a hospital share certain traits, or which other products a
bank customer might be likely to buy.
Elad, originally of Israel, uses technology he calls “pattern-based analytics.”
“We’re just scratching the surface of what can be done,” he said.
Predictive analytics, also known as data mining, is widespread in
the field of business intelligence. But Elad has managed to find a new
twist, said Tom Davenport, professor of information technology and
management at Babson College in Massachusetts.
Most analytics use regression, a statistical technique that’s been
around for a century, which helps explain the relationship between
variables, he said.
What Elad is doing is pattern matching, which is more complicated
and relies on artificial intelligence, Davenport said. By establishing
that something has taken place in the past, it predicts what will
happen in the future, he said.
- See more at: http://deltechpark.org/2011/12/seeing-a-pattern/#sthash.ufX9Zjfg.dpuf
Joseph Budner Elad has sought patterns in roadside bombings in war, and the path of deadly pathogens.
Now, Elad, president and CEO of Quantum Leap Innovations of Newark,
has begun putting his company’s pattern-seeking technology to more
everyday use for business.
For instance, the software can examine whether patients who get
readmitted to a hospital share certain traits, or which other products a
bank customer might be likely to buy.
Elad, originally of Israel, uses technology he calls “pattern-based analytics.”
“We’re just scratching the surface of what can be done,” he said.
Predictive analytics, also known as data mining, is widespread in
the field of business intelligence. But Elad has managed to find a new
twist, said Tom Davenport, professor of information technology and
management at Babson College in Massachusetts.
Most analytics use regression, a statistical technique that’s been
around for a century, which helps explain the relationship between
variables, he said.
What Elad is doing is pattern matching, which is more complicated
and relies on artificial intelligence, Davenport said. By establishing
that something has taken place in the past, it predicts what will
happen in the future, he said.
- See more at: http://deltechpark.org/2011/12/seeing-a-pattern/#sthash.ufX9Zjfg.dpuf
Joseph Budner Elad has sought patterns in roadside bombings in war, and the path of deadly pathogens.
Now, Elad, president and CEO of Quantum Leap Innovations of Newark, has begun putting his company’s pattern-seeking technology to more everyday use for business.
For instance, the software can examine whether patients who get readmitted to a hospital share certain traits, or which other products a bank customer might be likely to buy.
Elad, originally of Israel, uses technology he calls “pattern-based analytics.”
“We’re just scratching the surface of what can be done,” he said.
Predictive analytics, also known as data mining, is widespread in the field of business intelligence. But Elad has managed to find a new twist, said Tom Davenport, professor of information technology and management at Babson College in Massachusetts.
Most analytics use regression, a statistical technique that’s been around for a century, which helps explain the relationship between variables, he said.
What Elad is doing is pattern matching, which is more complicated and relies on artificial intelligence, Davenport said. By establishing that something has taken place in the past, it predicts what will happen in the future, he said.
 Vaibhav Rastogi
Vaibhav Rastogi Sylvain Doré
Sylvain Doré


 Alan C. Evans
Alan C. Evans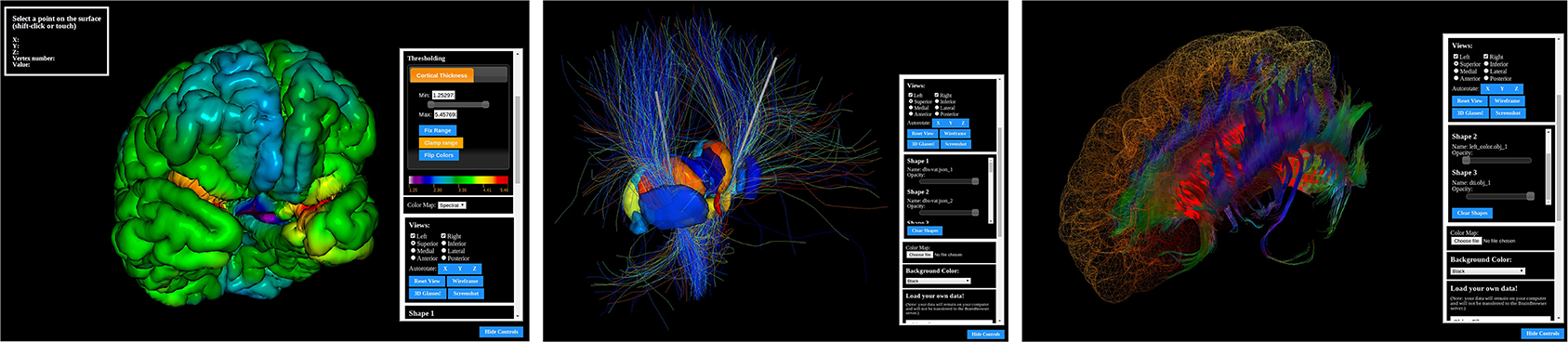 Figure 1. The BrainBrowser Surface Viewer.
Figure 1. The BrainBrowser Surface Viewer.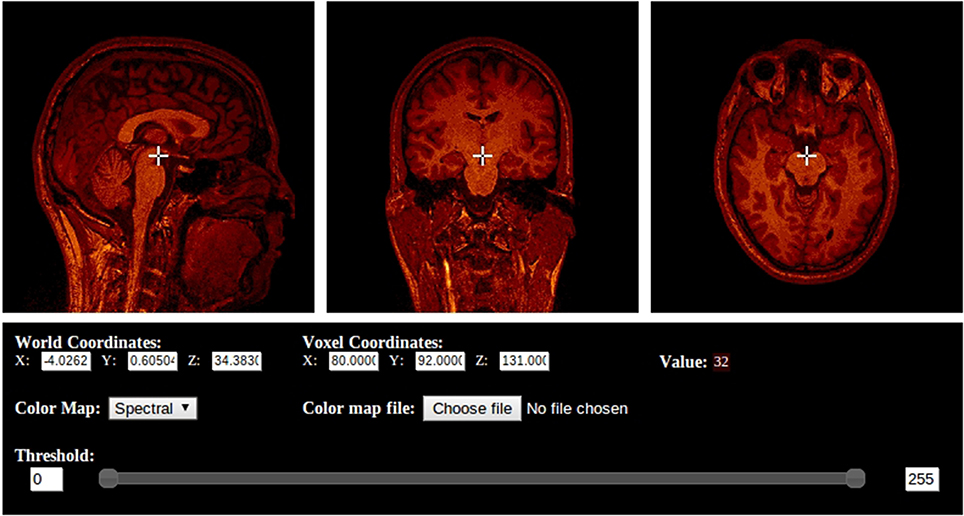 Figure 2. The BrainBrowser Volume Viewer.
Figure 2. The BrainBrowser Volume Viewer. Valentina Echeverria Moran
Valentina Echeverria Moran