I'm not sure what this is saying, ask your researchers if this is good or bad news. Inhibiting glutamate release sounds like hyperacute therapy to me.
http://www.biomedcentral.com/content/pdf/1476-511X-9-47.pdf
Background
During the last decade numerous studies have addressed
the role of the endocannabinoid (eCB) system in different
pathological conditions. Endocannabinoids (eCBs), e.g.
anandamide (AEA) and 2-arachidonoylglycerol (2-AG),
are lipid mediators synthesized "on demand" that inhibit
neurotransmitter (glutamate and GABA) release and
modulate neuroinflammation by activating specific CB1
(highly expressed in the CNS, where they mediate the
psychotropic effects of Δ9-tetrahydrocannabinol) and
CB2 (expressed by immune cells, including brain resident
microglial cells) receptors, respectively. Cannabinoid
receptor-inactive eCB-related molecules, e.g. palmitoylethanolamide
(PEA), also exert neuroprotective effects[1-
3], presumably by preventing mast cell degranulation [4],
and directly activating peroxisome proliferator-activated
receptor (PPAR)-α [5], or by enhancing the effects of
AEA on cannabinoid receptors, transient receptor potential
vanilloid type-1 (TRPV1) channels and PPAR-γ
receptors [6].
Previous murine and cell culture studies on stroke and
hypoxia postulated a neuroprotective role of eCBs, given
their ability to decrease NMDA-mediated toxicity in vascular
penumbra through a CB1-mediated mechanism [7].
Increases of AEA content, of the AEA biosynthetic precursors
(e.g. N-acyl phosphatidylethanolamines), and of
CB1 receptors expression in ischemic brain regions of
murine stroke models have been described [8-11]. CB1
knockout mice develop larger stroke volumes than wildtype
animals, with consequent increased post-stroke disability
and mortality [12]. In addition, CB1 agonist administration
was associated with a decrease of infarct volume
and with an improvement of clinical symptoms in stroketreated
mice [13]. Interestingly, there is evidence that also
low-doses of CB1 receptor antagonists, such as rimonabant,
reduce infarct volume in stroke models [9,10,14,15],
possibly by enhancing TRPV1-mediated actions [14]. It
has been also suggested that part of the neuroprotective
effects of CB1 receptor agonists in stroke is due to their
capability of lowering body temperature, and that CB1, as
opposed to CB2, receptors might otherwise play a counterprotective
role in cerebral ischemia [15].
Indeed, also CB2 receptors have been implicated in the
pathogenesis of stroke. Since such receptors are particularly
expressed on activated microglia and peripheral
immune cells (mastcells, macrophages and lymphocytes),
they may act by modulating the inflammatory response
to stroke [16], which is triggered 24-48 hours after symptoms
onset and is mainly responsible for the delayed neuronal
death [17]. Indeed CB2 agonists administration was
associated with a reduction of infarct volume and neurological
impairment in murine models of stroke and cerebral
ischemia [15,18]. However, such evidence is still
lacking in humans, despite the fact that a single case
report described an increase of AEA and PEA content in
the ischemic hemisphere of a stroke patient [19].
Aim of this study was to evaluate the possible involvement
of the eCB system in stroke patients, by measuring
plasma AEA, 2-AG, and PEA levels in the acute phase of
the disease and by correlating eCB and PEA plasmatic
levels with measures of neurological impairment and volume
of the ischemic brain tissue.
Sunday, September 30, 2012
Learning requires rhythmical activity of neurons
So who is going to translate this into a stroke protocol?
http://www.sciencecodex.com/learning_requires_rhythmical_activity_of_neurons-99056
pictue from the site.
http://www.sciencecodex.com/learning_requires_rhythmical_activity_of_neurons-99056
pictue from the site.
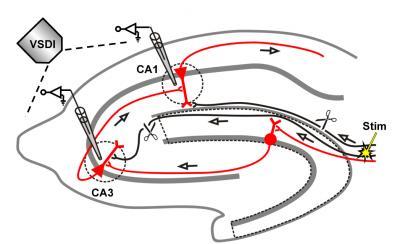
This is a schematic diagram of the trisynaptic circuit of the
hippocampus (red) and the position of the stimulation electrode.
Neuronal activity was measured using fluorescent dyes that react to
changes in voltage and a fluorescence microscope. Microelectrodes in the
CA1 and CA3 region record the electrical signals.
(Photo Credit: MPI of Psychiatry)
(Photo Credit: MPI of Psychiatry)
Baby steps in biking#3 - stroke rehab
Once again, fully successful this time, only about 10 minutes and never got out of the parking lot. It requires vast amounts of mental processing because the dividing line between success and disaster is so fine that I have to continually calculate speed, lean, obstacles, cars, feet on pedals, left arm still on handlebar?.
A new learning; when braking, the affected foot-left needs to be on the bottom of the pedal arc, this allows the weight to be distributed evenly with no quick weight shifts as the feet come off the pedals.
An additional item to work on;
1. Buckling the helmet, currently a frustrating one-handed affair. The left arm will not stay up close to my chin - the same problem as not being able to hold a phone on my left hand. My fingers have no release capability so they would pull everything apart.
I'll keep trying.
Why your stroke doctor should be paid based on your outcome
Double rant rating here:

This is one of the keys to getting better stroke rehab. Our doctors have no incentive to find better ways of doing rehab. And I know this is going to be controversial. So if you have a response that doesn't just attack me for sticking my opinion into medical matters, I will print it.
Lets put it baldly out there: Stroke rehab is a failure, look at the statistics, 10% full recovery is godawful.
http://oc1dean.blogspot.com/2011/05/stroke-recovery-statistics.html
http://oc1dean.blogspot.com/2012/05/5-things-physicians-can-learn-from.html
1. I think maybe doctors and teachers might be the only professions left that are not compensated based on results, you write up objectives and at the end of the year justify your rating based on how close you came.
2. If we have results-based therapy;
A. We'll get a specific damage diagnosis because a baseline would be needed to prove improvent.
B. We'll get doctors asking their stroke associations to provide them with concrete proven therapy protocols.
C. We'll get translation from clinical research to therapy much faster.
D. Stroke patients will actually have a say in the way stroke rehab is provided thru their doctors.
E. Stroke survivors could look up with a factual basis those that provide the best recovery possibilities. None of this crap, 'We're certified by the Joint Commission' (A great place to hide behind).
F We'll get faster and much better hyperacute therapies that stop the neuronal cascade of death because stopping neuronal death is much easier than therapy after the fact.
G. Followup will occur rather than being released to home after 2-3 months.
H. We'll actually get written stroke protocols.
Have at it, I want to see some well-reasoned arguments against this or your own proposal that would accomplish the same thing. Prevention will not be accepted as a viable answer. Copying the crap from the WSO does not count.
 Only one rant off because this rant needs to be left open.
Only one rant off because this rant needs to be left open.
A doctor blogging disagreeing about pay for performance, I disagree.
This is one of the keys to getting better stroke rehab. Our doctors have no incentive to find better ways of doing rehab. And I know this is going to be controversial. So if you have a response that doesn't just attack me for sticking my opinion into medical matters, I will print it.
Lets put it baldly out there: Stroke rehab is a failure, look at the statistics, 10% full recovery is godawful.
http://oc1dean.blogspot.com/2011/05/stroke-recovery-statistics.html
http://oc1dean.blogspot.com/2012/05/5-things-physicians-can-learn-from.html
1. I think maybe doctors and teachers might be the only professions left that are not compensated based on results, you write up objectives and at the end of the year justify your rating based on how close you came.
2. If we have results-based therapy;
A. We'll get a specific damage diagnosis because a baseline would be needed to prove improvent.
B. We'll get doctors asking their stroke associations to provide them with concrete proven therapy protocols.
C. We'll get translation from clinical research to therapy much faster.
D. Stroke patients will actually have a say in the way stroke rehab is provided thru their doctors.
E. Stroke survivors could look up with a factual basis those that provide the best recovery possibilities. None of this crap, 'We're certified by the Joint Commission' (A great place to hide behind).
F We'll get faster and much better hyperacute therapies that stop the neuronal cascade of death because stopping neuronal death is much easier than therapy after the fact.
G. Followup will occur rather than being released to home after 2-3 months.
H. We'll actually get written stroke protocols.
Have at it, I want to see some well-reasoned arguments against this or your own proposal that would accomplish the same thing. Prevention will not be accepted as a viable answer. Copying the crap from the WSO does not count.
Only one rant off because this rant needs to be left open.A doctor blogging disagreeing about pay for performance, I disagree.
Some performance measures make sense, but P4P does not
Saturday, September 29, 2012
Jankowski Method - physical therapy
I wonder how different this is from the Vasa concept. Trademarking standard PT concepts seems rather cutthroat. Ask your therapist if they are paying royalties to him for using his concepts. I suppose every survivor should be paying him, and every PT school.
videos here: No explanation of what the concept is.
http://www.youtube.com/watch?v=9f5lWiAlI7U
http://www.youtube.com/watch?v=ccktrWXepEY sic(ponds?
http://www.youtube.com/watch?v=ccktrWXepEY
http://www.youtube.com/watch?v=OuURO3AsD1w&feature=relmfu
Revolutionary Breakthrough In Neurological Rehabilitation. Where?
The business page here:
http://healthcare.zibb.com/trademark/the+jankowski+method/30008728
Look at these related products;
Medical services; Veterinary services; Hygienic and beauty care for humans or animals.
Maybe not so bad, its abandoned;
http://www.trademarkia.com/the-jankowski-method-76293482.html
This is not an endorsement
videos here: No explanation of what the concept is.
http://www.youtube.com/watch?v=9f5lWiAlI7U
http://www.youtube.com/watch?v=ccktrWXepEY sic(ponds?
http://www.youtube.com/watch?v=ccktrWXepEY
http://www.youtube.com/watch?v=OuURO3AsD1w&feature=relmfu
Revolutionary Breakthrough In Neurological Rehabilitation. Where?
The business page here:
http://healthcare.zibb.com/trademark/the+jankowski+method/30008728
Look at these related products;
Medical services; Veterinary services; Hygienic and beauty care for humans or animals.
Maybe not so bad, its abandoned;
http://www.trademarkia.com/the-jankowski-method-76293482.html
This is not an endorsement
Stroke patients on a downhill memory slope
But will neurogenesis in the hippocampus offset these declines?
http://www.news-medical.net/news/20120910/Stroke-patients-on-a-downhill-memory-slope.aspx
The large memory declines associated with acute stroke are part of a long-term downward trajectory, show findings from the Health and Retirement Study (HRS).
Even before the event, HRS participants who had stroke had significantly steeper memory declines than those who did not.
The HRS participants did an immediate- and delayed-recall memory test every 2 years, which revealed memory declines of an average 0.143 points per year among the 1574 participants who went on to have a stroke. By contrast, the decline was just 0.101 points per year among the 15,766 who remained stroke-free during up to 10 years of follow up.
Memory differences between participants who did and did not have a stroke were apparent up to 4 years before onset. The differences persisted after accounting for variables including age, gender, and age at stroke onset.
"Prestroke memory decline is most likely an early sign of cerebrovascular disease," M Maria Glymour and team, from the Harvard School of Public Health in Boston, Massachusetts, USA, write in Stroke.
"However, it is also plausible that lower memory performance increases vulnerability to clinically manifest stroke. Individuals with very high memory scores may have better cognitive reserve and may be able to sustain an acute ischemic event without severe clinical manifestations."
They note that this difference "has important clinical implications and therefore merits further exploration."
The prestroke rate of memory decline was particularly steep among the 385 people who did not survive their stroke. At 0.212 points per year, this was a significantly steeper decline than that seen among stroke survivors.
"These individuals may have particularly severe underlying cerebrovascular disease that causes very rapid cognitive declines culminating in fatal stroke, or the prestroke cognitive declines may be attributable to causes other than cerebrovascular disease but may render the patient frail or unusually vulnerable to death as a result of the stroke," Glymour et al suggest.
Stroke caused a large decrease in memory performance, of 0.369 points, equivalent to 3.7 years of age-related memory decline among stroke-free participants. But after stroke, memory in stroke survivors continued to decline at a similar rate to that before stroke, at 0.142 points per year.
"This finding may indicate that cerebrovascular risk factors are not adequately controlled after stroke diagnosis, or that acute stroke presages an ongoing, cascading process of neurological injury," say the researchers.
http://www.news-medical.net/news/20120910/Stroke-patients-on-a-downhill-memory-slope.aspx
The large memory declines associated with acute stroke are part of a long-term downward trajectory, show findings from the Health and Retirement Study (HRS).
Even before the event, HRS participants who had stroke had significantly steeper memory declines than those who did not.
The HRS participants did an immediate- and delayed-recall memory test every 2 years, which revealed memory declines of an average 0.143 points per year among the 1574 participants who went on to have a stroke. By contrast, the decline was just 0.101 points per year among the 15,766 who remained stroke-free during up to 10 years of follow up.
Memory differences between participants who did and did not have a stroke were apparent up to 4 years before onset. The differences persisted after accounting for variables including age, gender, and age at stroke onset.
"Prestroke memory decline is most likely an early sign of cerebrovascular disease," M Maria Glymour and team, from the Harvard School of Public Health in Boston, Massachusetts, USA, write in Stroke.
"However, it is also plausible that lower memory performance increases vulnerability to clinically manifest stroke. Individuals with very high memory scores may have better cognitive reserve and may be able to sustain an acute ischemic event without severe clinical manifestations."
They note that this difference "has important clinical implications and therefore merits further exploration."
The prestroke rate of memory decline was particularly steep among the 385 people who did not survive their stroke. At 0.212 points per year, this was a significantly steeper decline than that seen among stroke survivors.
"These individuals may have particularly severe underlying cerebrovascular disease that causes very rapid cognitive declines culminating in fatal stroke, or the prestroke cognitive declines may be attributable to causes other than cerebrovascular disease but may render the patient frail or unusually vulnerable to death as a result of the stroke," Glymour et al suggest.
Stroke caused a large decrease in memory performance, of 0.369 points, equivalent to 3.7 years of age-related memory decline among stroke-free participants. But after stroke, memory in stroke survivors continued to decline at a similar rate to that before stroke, at 0.142 points per year.
"This finding may indicate that cerebrovascular risk factors are not adequately controlled after stroke diagnosis, or that acute stroke presages an ongoing, cascading process of neurological injury," say the researchers.
Who will help you recover from your stroke?
You. You alone have to do it.
This is only my 6th related post on this subject;
1. http://oc1dean.blogspot.com/2012/09/my-theory-on-motor-recovery-stroke-rehab.html
2. http://oc1dean.blogspot.com/2012/09/what-is-your-stroke-protocol.html
3. http://oc1dean.blogspot.com/2012/09/are-you-on-your-own-for-stroke-recovery.html
4. http://oc1dean.blogspot.com/2012/08/when-your-recovery-fails-what-is-your.html
5. http://oc1dean.blogspot.com/2011/11/why-good-doctors-give-useless-answers.html
You will need to rely on yourself, your therapists can give you exercises to do but you will need to do them. Dr. Steven Wolfs contention, 'Stroke patients need to rely more on their own problem solving to regain mobility', You can read all the survivor books you want and the common factor is persistence, not giving up. There are NO shortcuts, NO drugs, NO stem cells in the current environment to help you. That's why I am ranting so much on the hyperacute possibilities. If we can prevent lots of neurons from dying the future survivors will not have such difficult times trying to recover. And that will only happen if we can convince the whole stroke medical world that they are failing and need to look for solutions.
Until that wonderful world comes you will have to follow this and make yourself be in the 10% as listed below.
This book, The survivors club : the secrets and science that could save your life / Ben Sherwood, was interesting in that it broke down survivors of disasters into 3 groups. 10% would actively become leaders, 80% would follow the leaders, 10% would do nothing. I try to apply this to my stroke survivorship and am working on being in the top 10%. Maybe this is why only 10% of survivors fully recover.
If you are a follower you may not recover to the best of your ability.
You have to become the 10%. Its lonely up there.
This is only my 6th related post on this subject;
1. http://oc1dean.blogspot.com/2012/09/my-theory-on-motor-recovery-stroke-rehab.html
2. http://oc1dean.blogspot.com/2012/09/what-is-your-stroke-protocol.html
3. http://oc1dean.blogspot.com/2012/09/are-you-on-your-own-for-stroke-recovery.html
4. http://oc1dean.blogspot.com/2012/08/when-your-recovery-fails-what-is-your.html
5. http://oc1dean.blogspot.com/2011/11/why-good-doctors-give-useless-answers.html
You will need to rely on yourself, your therapists can give you exercises to do but you will need to do them. Dr. Steven Wolfs contention, 'Stroke patients need to rely more on their own problem solving to regain mobility', You can read all the survivor books you want and the common factor is persistence, not giving up. There are NO shortcuts, NO drugs, NO stem cells in the current environment to help you. That's why I am ranting so much on the hyperacute possibilities. If we can prevent lots of neurons from dying the future survivors will not have such difficult times trying to recover. And that will only happen if we can convince the whole stroke medical world that they are failing and need to look for solutions.
Until that wonderful world comes you will have to follow this and make yourself be in the 10% as listed below.
This book, The survivors club : the secrets and science that could save your life / Ben Sherwood, was interesting in that it broke down survivors of disasters into 3 groups. 10% would actively become leaders, 80% would follow the leaders, 10% would do nothing. I try to apply this to my stroke survivorship and am working on being in the top 10%. Maybe this is why only 10% of survivors fully recover.
If you are a follower you may not recover to the best of your ability.
You have to become the 10%. Its lonely up there.
World Heart Day: New European statistics released on heart disease and stroke
So much to fix and nobody is taking responsibility for it.
http://www.eurekalert.org/pub_releases/2012-09/esoc-whd092612.php
The figures show some progress. Since the 2008 report there has been a substantial drop in the number of deaths attributed to heart disease. CVD is now responsible for four million European deaths annually, down from 4.3 million in 2008 (which represents a drop from 48% to 47% of total European deaths). Within the EU, it is responsible for 1.8 million deaths per year, down from two million in 2008 (40% of all EU deaths, down from 42%)2.
Commenting, ESC President, Professor Panos Vardas said:
"There is good news here, but it needs to be approached with some caution. Fewer lives are being lost to cardiovascular disease than in 2008. At the same time, the scale of the problem is enormous. CVD is still responsible for four million European deaths per year. This is a real human tragedy and a significant economic burden. We anticipate this burden will continue to increase in the coming years due to ageing populations and unhealthy lifestyles".
Dr. Hans Stam, President of the European Heart Network, said:
"This reduction in CVD mortality is a real success story. A few years ago it seemed that the rise in cardiovascular disease was unstoppable; this report shows that we have reversed that trend, and that lives are being saved. At the same time, we know that there are potential problems ahead. Diabetes and obesity are rising, smoking is still a major issue, and people are still not doing enough physical activity. The continent is also growing older. Today's figures are good, very good, but they must not lead to complacency".
The report contains a range of European comparators, giving the latest available figures on mortality, morbidity, treatment, smoking, diet, physical activity, alcohol, blood pressure, cholesterol, overweight and obesity, diabetes, and financial implications for each country. Key statistics include:
Professor Vardas concluded: "The drop in CVD mortality across Europe is due to a range of factors, not just a single initiative. For example, over the last few years we have taken steps to lower blood pressure and cholesterol levels, and to highlight the dangers of smoking. These measures have helped enormously, but at the same time many lifestyle-linked changes, such as increasing obesity and diabetes, will make it harder for us to stand still. Most of cardiovascular related deaths are preventable. EHN, the ESC and its partners will continue to lobby for the implementation of changes in legislation and for population interventions in order to promote a healthier environment".
http://www.eurekalert.org/pub_releases/2012-09/esoc-whd092612.php
Figures show significant drop in mortality, but the scale of the problem is huge and will increase
The statistics show that efforts to reduce heart disease deaths are successful, with mortality now falling in most of the continent. At the same time, the report shows the huge burden CVD presents to Europe's health, and suggests that underlying factors may cause CVD to increase in the near future.The figures show some progress. Since the 2008 report there has been a substantial drop in the number of deaths attributed to heart disease. CVD is now responsible for four million European deaths annually, down from 4.3 million in 2008 (which represents a drop from 48% to 47% of total European deaths). Within the EU, it is responsible for 1.8 million deaths per year, down from two million in 2008 (40% of all EU deaths, down from 42%)2.
Commenting, ESC President, Professor Panos Vardas said:
"There is good news here, but it needs to be approached with some caution. Fewer lives are being lost to cardiovascular disease than in 2008. At the same time, the scale of the problem is enormous. CVD is still responsible for four million European deaths per year. This is a real human tragedy and a significant economic burden. We anticipate this burden will continue to increase in the coming years due to ageing populations and unhealthy lifestyles".
Dr. Hans Stam, President of the European Heart Network, said:
"This reduction in CVD mortality is a real success story. A few years ago it seemed that the rise in cardiovascular disease was unstoppable; this report shows that we have reversed that trend, and that lives are being saved. At the same time, we know that there are potential problems ahead. Diabetes and obesity are rising, smoking is still a major issue, and people are still not doing enough physical activity. The continent is also growing older. Today's figures are good, very good, but they must not lead to complacency".
The report contains a range of European comparators, giving the latest available figures on mortality, morbidity, treatment, smoking, diet, physical activity, alcohol, blood pressure, cholesterol, overweight and obesity, diabetes, and financial implications for each country. Key statistics include:
- CVD hits women especially hard – it is the main cause of death for women in each of the 27 EU countries3.
- CVD is the leading cause of death for men in all the EU countries except France, the Netherlands, Slovenia and Spain3.
- Stroke is the second single most common cause of death in Europe: accounting for almost 1.1 million deaths each year. Over one in seven women (15%) and one in ten men (10%) die from the disease3.
- There are huge differences in CVD mortality within Europe. For example, for men CVD causes between 60% (Bulgaria) and 25% of deaths (France) and for women between 70% (Bulgaria) and 30% of deaths (France and the Netherlands)4.
- The prevalence of diabetes is high, with more than 50% rises in some countries in the last decade. This, plus increasing obesity levels, is threatening to reverse the improvements of recent years5.
- The economic burden of CVD is huge, estimated €196 billion a year, of which around 54% is due to direct health expenditure; 24% to productivity losses and 22% to the informal care of people with CVD. The impact on national health care systems is approximately €212 per year6, per person, in the EU.
- The figures also show substantial regional differences. Central and Eastern Europe saw large increases in CVD deaths in the years up to the turn of the century, but now mortality rates in this region are declining significantly. For example, over the 2003-2009 period, the rate of coronary heart disease (CHD) deaths in Russian men dropped from 251 to 186 (per 100,000). Nevertheless, these figures are still huge in comparison with other areas in Europe: for example, the UK has a male mortality rate of 33 per 100,000, and in the Netherlands this rate is 16 per 100,000 (2009 figures)7.
Professor Vardas concluded: "The drop in CVD mortality across Europe is due to a range of factors, not just a single initiative. For example, over the last few years we have taken steps to lower blood pressure and cholesterol levels, and to highlight the dangers of smoking. These measures have helped enormously, but at the same time many lifestyle-linked changes, such as increasing obesity and diabetes, will make it harder for us to stand still. Most of cardiovascular related deaths are preventable. EHN, the ESC and its partners will continue to lobby for the implementation of changes in legislation and for population interventions in order to promote a healthier environment".
Friday, September 28, 2012
Preventing falls in older people could save the economy up to €500 million per annum
I covered this in my slide presentation on dangerous stroke rehab. So ask your therapist/doctor why they are pushing you into walking when the end result is so dangerous. I bet you didn't sign a therapy release for this.
http://www.alphagalileo.org/ViewItem.aspx?ItemId=124413&CultureCode=en
The TRIL Centre with Get Ireland Active announces Falls Awareness Day, Thursday 4th October 2012.
One in three people over the age of 65 will fall every year in Ireland. Two-thirds of this group will fall again within six months, leading to risk of hospitalisation and significant health decline. As well as physical injuries suffered, the psychological and social consequences of falling can have a huge impact on the faller.
People who fall may suffer depression, anxiety, isolation and loss of independence. In addition a recent study by The Irish Centre for Social Gerontology showed that the cost to the economy of falls and fractures in older people is about €500 million annually. This includes costs associated with emergency department visits, hospital stays, GP and outpatient visits and long-term care.
To raise awareness of the importance of falls prevention, the TRIL Centre will demonstrate its technology at a stand in St. James’s Hospital Dublin on Falls Awareness Day, Thursday 4th October, with support from the Falls and Black Out Unit (FABU) at the hospital. In addition the centre has created a webpage with information and links about falls awareness and prevention. www.trilcentre.org/fallsawareness2012.
Falls in older people can be prevented by increasing awareness of falls risks. The TRIL Centre is at the forefront of using novel sensor technology and algorithms to quantify risk of falling. This technology, the Falls Risk Assessment Suite, aims to improve accuracy in assessing falls risk and mobility, resulting in more targeted interventions. The technology suite has been developed on a mobile platform using wireless sensors; this model enables sophisticated falls risk assessment to be undertaken in the home or community.
Speaking about the need to predict risk of falling, Consultant Physician and Director of the Falls and Blackout Unit at St. James’s Hospital, Professor Rose Anne Kenny, TRIL Principal Investigator for Falls Prevention and Professor of Geriatric Medicine in Trinity College Dublin said: "the EU has targeted falls prevention as one of its main priorities for health research in ageing. Falls become more common as we age and the consequences of falls, such as fractures, also increase. Unfortunately recurrent falls often result in admission to long term care. Therefore early detection of treatable conditions which cause falls can prevent these serious consequences. These new technologies provide such early detection."
Coinciding with Positive Ageing week, the message from the TRIL Centre and Get Active Ireland is Keep physically active. Exercise can help to improve your balance and your strength, if you are worried about falling contact your GP. Professor Kenny added: “Falls are very common in older people, however they are preventable. We have many treatments that can help people back to full health and independence, particularly if risk assessment and intervention is provided at an early stage.”
http://www.alphagalileo.org/ViewItem.aspx?ItemId=124413&CultureCode=en
The TRIL Centre with Get Ireland Active announces Falls Awareness Day, Thursday 4th October 2012.
One in three people over the age of 65 will fall every year in Ireland. Two-thirds of this group will fall again within six months, leading to risk of hospitalisation and significant health decline. As well as physical injuries suffered, the psychological and social consequences of falling can have a huge impact on the faller.
People who fall may suffer depression, anxiety, isolation and loss of independence. In addition a recent study by The Irish Centre for Social Gerontology showed that the cost to the economy of falls and fractures in older people is about €500 million annually. This includes costs associated with emergency department visits, hospital stays, GP and outpatient visits and long-term care.
To raise awareness of the importance of falls prevention, the TRIL Centre will demonstrate its technology at a stand in St. James’s Hospital Dublin on Falls Awareness Day, Thursday 4th October, with support from the Falls and Black Out Unit (FABU) at the hospital. In addition the centre has created a webpage with information and links about falls awareness and prevention. www.trilcentre.org/fallsawareness2012.
Falls in older people can be prevented by increasing awareness of falls risks. The TRIL Centre is at the forefront of using novel sensor technology and algorithms to quantify risk of falling. This technology, the Falls Risk Assessment Suite, aims to improve accuracy in assessing falls risk and mobility, resulting in more targeted interventions. The technology suite has been developed on a mobile platform using wireless sensors; this model enables sophisticated falls risk assessment to be undertaken in the home or community.
Speaking about the need to predict risk of falling, Consultant Physician and Director of the Falls and Blackout Unit at St. James’s Hospital, Professor Rose Anne Kenny, TRIL Principal Investigator for Falls Prevention and Professor of Geriatric Medicine in Trinity College Dublin said: "the EU has targeted falls prevention as one of its main priorities for health research in ageing. Falls become more common as we age and the consequences of falls, such as fractures, also increase. Unfortunately recurrent falls often result in admission to long term care. Therefore early detection of treatable conditions which cause falls can prevent these serious consequences. These new technologies provide such early detection."
Coinciding with Positive Ageing week, the message from the TRIL Centre and Get Active Ireland is Keep physically active. Exercise can help to improve your balance and your strength, if you are worried about falling contact your GP. Professor Kenny added: “Falls are very common in older people, however they are preventable. We have many treatments that can help people back to full health and independence, particularly if risk assessment and intervention is provided at an early stage.”
Optimizing muscle power after stroke: a cross-sectional study
Ask your therapist and doctor to use this in your therapy protocol.
http://www.jneuroengrehab.com/content/9/1/67/abstract
http://www.jneuroengrehab.com/content/9/1/67/abstract
Abstract (provisional)
Background
Stroke remains a leading cause of disability worldwide and results in muscle performance
deficits and limitations in activity performance. Rehabilitation aims to address muscle
dysfunction in an effort to improve activity and participation. While both muscle
strength and power have an impact on activity performance, power has recently been
acknowledged as contributing significantly to activity performance in this population.
Therefore, rehabilitation efforts should include training of muscle power. However,
little is known about what training parameters optimize muscle power performance in
people with stroke. The purpose of this study was to investigate lower limb muscle
power performance at differing loads in people with and without stroke.
Methods
A cross-sectional study design investigated muscle power performance in 58 hemiplegic
and age matched control participants. Lower limb muscle power was measured using a
modified leg press machine at 30, 50 and 70% of one repetition maximum (1-RM) strength.
Results
There were significant differences in peak power between involved and uninvolved limbs
of stroke participants and between uninvolved and control limbs. Peak power was greatest
when pushing against a load of 30% of 1RM for involved, uninvolved and control limbs.
Involved limb peak power irrespective of load (Mean:220 [PLUS-MINUS SIGN] SD:134 W)
was significantly lower (p < 0.05) than the uninvolved limb (Mean:466 [PLUS-MINUS
SIGN] SD:220 W). Both the involved and uninvolved limbs generated significantly lower
peak power (p < 0.05) than the control limb (Mean:708 [PLUS-MINUS SIGN] SD:289 W).
Conclusions
Significant power deficits were seen in both the involved and uninvolved limbs after
stroke. Maximal muscle power was produced when pushing against lighter loads. Further
intervention studies are needed to determine whether training of both limbs at lighter
loads (and higher velocities) are preferable to improve both power and activity performance
after stroke.
The complete article is available as a provisional PDF. The fully formatted PDF and HTML versions are in production.
Practical Stroke Rehabilitation Care: Staying on the Cutting Edge
An RIC course, the most interesting would be
Management of the Neurological Hand at Various Stages of
Recovery
- Marilyn Harvey, OTR/L
Molly Listenberger, OTD, OTR/L
Kim Eberhardt Muir, MS, OTR/L
Katie Polo, MHS, OTR/L, CLT-LANA
That would be worth sitting in on.
Practical Stroke Rehabilitation Care: Staying on the Cutting Edge
COURSE OBJECTIVES
Upon completion of this course, participants will be able to:
• Summarize the research published over the past year(Thats all?) in stroke recovery and rehabilitation, discuss their implications to future research and apply them to clinical practice
• Describe a model of care for stroke rehabilitation that integrates clinical practice and research
• Discuss the purpose and use of commonly prescribed medications in stroke patients during rehabilitation
• Develop evidence-based outcomes for therapeutic management of attentional, perceptual and cognitive-communication interventions for right hemisphere stroke.(What about left hemisphere?)
• Summarize the research related to using non-invasive brain stimulation for neurorehabilitation of motor recovery (upper limb, lower limb and speech) following stroke
• Discuss strategies for increasing the number of steps in gait training for persons with stroke
• Apply various modalities and treatment options for persons post-stroke with mild-moderate levels of upper extremity recovery
• Summarize how families cope and adapt after stroke
• Describe the survivor’s perspective on returning to and maintaining work after stroke and provide recommendations to clinicians as to how to address these issues with their patients
• Demonstrate awareness and knowledge of the barriers and facilitators associated with limitations in access to exercise and physical activity in people with stroke
Canadian Stroke Congress to take place from Sept. 30 to Oct. 2
You will notice they failed to include survivor experts in their consideration
http://www.news-medical.net/news/20120928/Canadian-Stroke-Congress-to-take-place-from-Sept-30-to-Oct-2.aspx
Researchers from across Canada and around the world are gathering in Calgary for the largest-ever Canadian Stroke Congress, drawing much-needed attention to one of society's leading health issues. The Canadian Stroke Congress runs from Sept. 30 to Oct. 2 at the Calgary Telus Convention Centre.
A joint initiative of the Canadian Stroke Network, Heart and Stroke Foundation and Canadian Stroke Consortium, the congress brings together leading experts from basic research, prevention, treatment, rehabilitation and health promotion.
http://www.news-medical.net/news/20120928/Canadian-Stroke-Congress-to-take-place-from-Sept-30-to-Oct-2.aspx
Researchers from across Canada and around the world are gathering in Calgary for the largest-ever Canadian Stroke Congress, drawing much-needed attention to one of society's leading health issues. The Canadian Stroke Congress runs from Sept. 30 to Oct. 2 at the Calgary Telus Convention Centre.
A joint initiative of the Canadian Stroke Network, Heart and Stroke Foundation and Canadian Stroke Consortium, the congress brings together leading experts from basic research, prevention, treatment, rehabilitation and health promotion.
Thursday, September 27, 2012
Neuralstem Gets Approval To Commence Ischemic Stroke Trial In China
Read this on stem cells first;
http://www.nasdaq.com/article/neuralstem-gets-approval-to-commence-ischemic-stroke-trial-in-china-20120927-00705
Neuralstem, Inc. (CUR), Thursday said it was granted approval to commence a clinical trial, through its subsidiary, Neuralstem China, to treat motor deficits due to ischemic strokes with its spinal cord stem cells NSI-566 at BaYi Brain Hospital, in Beijing, China.
The approved trial will include a combined phase I/II design and will witness direct injections of NSI-566 cells into the brain. The trial is expected to begin early next year.
Ischemic strokes, one of the most common type of strokes, occur as a result of an obstruction within a blood vessel supplying blood to the brain.
Stem Cell Fraud: A 60 Minutes investigation
http://www.nasdaq.com/article/neuralstem-gets-approval-to-commence-ischemic-stroke-trial-in-china-20120927-00705
Neuralstem, Inc. (CUR), Thursday said it was granted approval to commence a clinical trial, through its subsidiary, Neuralstem China, to treat motor deficits due to ischemic strokes with its spinal cord stem cells NSI-566 at BaYi Brain Hospital, in Beijing, China.
The approved trial will include a combined phase I/II design and will witness direct injections of NSI-566 cells into the brain. The trial is expected to begin early next year.
Ischemic strokes, one of the most common type of strokes, occur as a result of an obstruction within a blood vessel supplying blood to the brain.
Neurohospitalists Improve Door-to-Needle Times for Patients With Ischemic Stroke Receiving Intravenous tPA
I was actually incredibly disappointed in their analysis, they didn't go outside their area of expertise to find a completely newer and better way to identify ischemic vs. hemorrhagic. Try this; 1. here, 2. here, 3. here, 4. here, 5. here, 6. here, 7. here, 8. here, 9. here, 10. here, 11. here, Don't these people keep up with research at all? And we are supposed to trust them with our lives?
http://nho.sagepub.com/content/2/4/119.full
http://nho.sagepub.com/content/2/4/119.full
Introduction
Patients with ischemic stroke benefit from intravenous tissue plasminogen activator (tPA), when given expeditiously.1
Current best practice strategy identified by American Heart
Association/American Stroke Association (AHA/ASA) sponsored Target:
Stroke program is to achieve a door-to-needle time
(DNT) ≤60 minutes for at least 50% of patients with acute ischemic
stroke.
However, less than one third of patients with acute
ischemic stroke who receive tPA are treated within the
guideline-recommended
60 minutes.2
This program has identified 10 key strategies to improve DNT. These
include emergency medical service prenotification, activating
the stroke team with a single call, rapid
acquisition and interpretation of brain imaging, use of specific
protocols and tools,
premixing tPA, a team-based approach, and rapid
data feedback.(I bet my 11 ways would be faster and easier) Neurohospitalists are inpatient site-specific specialists
mainly
responsible for managing inpatient neurological
conditions.3
Community neurologists, who are chiefly outpatient based and
periodically cover the hospital on call, may not have time or
interest to focus on inpatient quality and safety
metrics on top giving optimal care to their outpatient population.
Neurohospitalist
model has been associated with reduced length of
stay in patients with ischemic stroke.4
Limited data are available regarding whether inpatient neurohospitalist
evaluation has an impact on DNT for intravenous thrombolysis
in patients with ischemic stroke within 4.5 hours
of symptom onset. We know that most inpatient neurologists are vascular
neurologists.2
But, there is no specific data comparing vascular neurologists and
community neurologists on the quality of inpatient care.
Our aim is to retrospectively compare DNT for
intravenous thrombolysis in ischemic stroke between nonneurohospitalists
and
neurohospitalists at a single institution in the
emergency department (ED).
A multi-pad electrode based functional electrical stimulation system for restoration of grasp
See if this is enough evidence-based medicine for your therapists to use on you. If they are really good they'll know about this before you do.
http://www.jneuroengrehab.com/content/9/1/66/abstract
http://www.jneuroengrehab.com/content/9/1/66/abstract
Abstract (provisional)
Background
Functional electrical stimulation (FES) applied via transcutaneous electrodes is a
common rehabilitation technique for assisting grasp in patients with central nervous
system lesions. To improve the stimulation effectiveness of conventional FES, we introduce
multi-pad electrodes and a new stimulation paradigm.
Methods
The new FES system comprises an electrode composed of small pads that can be activated
individually. This electrode allows the targeting of motoneurons that activate synergistic
muscles and produce a functional movement. The new stimulation paradigm allows asynchronous
activation of motoneurons and provides controlled spatial distribution of the electrical
charge that is delivered to the motoneurons. We developed an automated technique for
the determination of the preferred electrode based on a cost function that considers
the required movement of the fingers and the stabilization of the wrist joint. The
data used within the cost function come from a sensorized garment that is easy to
implement and does not require calibration. The design of the system also includes
the possibility for fine-tuning and adaptation with a manually controllable interface.
Results
The device was tested on three stroke patients. The results show that the multi-pad
electrodes provide the desired level of selectivity and can be used for generating
a functional grasp. The results also show that the procedure, when performed on a
specific user, results in the preferred electrode configuration characteristics for
that patient. The findings from this study are of importance for the application of
transcutaneous stimulation in the clinical and home environments.
The complete article is available as a provisional PDF. The fully formatted PDF and HTML versions are in production.
Tuesday, September 25, 2012
Neural correlates of interspecies perspective taking in the post-mortem Atlantic Salmon
fMRI of dead salmon. A winner in this years Ig Nobels
You will need to confirm with your doctor that their reading of your fMRI is better than a dead salmon. Ask them if you have better brain activity.
The paper here:
http://prefrontal.org/files/posters/Bennett-Salmon-2009.pdf
A bloggers writeup here:
You will need to confirm with your doctor that their reading of your fMRI is better than a dead salmon. Ask them if you have better brain activity.
The paper here:
http://prefrontal.org/files/posters/Bennett-Salmon-2009.pdf
A bloggers writeup here:
Dead Fish Wins Ig Nobel
Its actually serious science if researchers and doctors can't read scans properly.
See acupuncture using fMRIs scans to prove efficacy. Not that I believe these studies.
Neuronal specificity of acupuncture response: a fMRI study with electroacupuncture.
An fMRI study showing the effect of acupuncture in chronic stage stroke patients with aphasia.
Nonstick trick in the brain Coated particles can slip past brain’s barriers
With this news we should be able to get any drug into the brain.
http://www.medical-blogs.org/blog-crawler?bci=561986&url=http://www.sciencenews.org/view/generic/id/345326/title/Nonstick_trick_in_the_brain
Getting drugs into the brain has proved to be a nanoscale puzzle: Anything bigger than 64 nanometers — about the size of a small virus — gets stuck in the space between brain cells once it gets through the blood-brain barrier. Justin Hanes of Johns Hopkins University School of Medicine and colleagues got around this rule by coating particles destined for brain cells in a dense layer of a polymer called polyethylene glycol. PEG acts like a Teflon coating for the particles, preventing them from sticking to structures within the brain and allowing them to move around more freely. When the researchers injected particles 100 nanometers across coated with either PEG (green) or negatively charged water-hating molecules (red) into the brain of a living mouse, the PEG particles easily penetrated the brain while the negatively charged particles got stuck. Larger nanoparticles would give doctors a more effective way to deliver drugs for brain cancers, strokes and other brain diseases, the team reports in the Aug. 29 Science Translational Medicine.
http://www.medical-blogs.org/blog-crawler?bci=561986&url=http://www.sciencenews.org/view/generic/id/345326/title/Nonstick_trick_in_the_brain
Getting drugs into the brain has proved to be a nanoscale puzzle: Anything bigger than 64 nanometers — about the size of a small virus — gets stuck in the space between brain cells once it gets through the blood-brain barrier. Justin Hanes of Johns Hopkins University School of Medicine and colleagues got around this rule by coating particles destined for brain cells in a dense layer of a polymer called polyethylene glycol. PEG acts like a Teflon coating for the particles, preventing them from sticking to structures within the brain and allowing them to move around more freely. When the researchers injected particles 100 nanometers across coated with either PEG (green) or negatively charged water-hating molecules (red) into the brain of a living mouse, the PEG particles easily penetrated the brain while the negatively charged particles got stuck. Larger nanoparticles would give doctors a more effective way to deliver drugs for brain cancers, strokes and other brain diseases, the team reports in the Aug. 29 Science Translational Medicine.
Acupuncture for Shoulder Pain After Stroke: A Systematic Review
You have to analyze this yourself.
Full text here: I was able to see it all
online.liebertpub.com/doi/pdfplus/10.1089/acm.2011.0457
abstract here:
http://online.liebertpub.com/doi/abs/10.1089/acm.2011.0457
This line proves that nothing was proven in the study due to dual therapies.
It is concluded from this systematic review that acupuncture combined with exercise is effective for shoulder pain after stroke.
This puff piece from a acupuncture web site is unbelievable;
http://www.healthcmi.com/index.php/acupuncturist-news-online/618-acupunctureceushoulderpainstrokenccaom
Full text here: I was able to see it all
online.liebertpub.com/doi/pdfplus/10.1089/acm.2011.0457
abstract here:
http://online.liebertpub.com/doi/abs/10.1089/acm.2011.0457
This line proves that nothing was proven in the study due to dual therapies.
It is concluded from this systematic review that acupuncture combined with exercise is effective for shoulder pain after stroke.
This puff piece from a acupuncture web site is unbelievable;
http://www.healthcmi.com/index.php/acupuncturist-news-online/618-acupunctureceushoulderpainstrokenccaom
Success Seen for tPA in Carotid Artery Stroke
I'm sure someone medical can explain this to me. But how do you have a stroke when a carotid artery is blocked and you have a functioning Circle of Willis? My carotid is totally blocked and I did not have a stroke whenever it closed up 4 years ago.
Success Seen for tPA in Carotid Artery Stroke
Intravenous thrombolysis should be considered a preferred first-line
treatment for acute occlusion of the cervical internal carotid artery
(ICA), a small retrospective study suggested.
Among 13 patients treated with recombinant tissue plasminogen
activator (rtPA) within the recommended treatment window, seven had good
functional recovery at 3 months, compared with only one of eight given
primary endovascular treatment, according to Raymond C.S. Seet, MD, of
the National University of Singapore, and colleagues.
Predictors of favorable functional outcome in patients treated with
rtPA included good collateral distal blood flow, with an odds ratio of
20 (95% CI 2 to 242, P=0.02) and neurologic recovery within 24 hours, with an odds ratio of 77 (95% CI 3 to 500, P=0.02), the researchers reported online in Archives of Neurology.
Statins and cerebral perfusion in patients with leukoaraiosis–a translational proof‐of‐principal MRI study
No abstract available so your doctor will need to buy the article.
http://onlinelibrary.wiley.com/doi/10.1111/j.1747-4949.2012.00807.x/abstract
Statins and cerebral perfusion in patients with
leukoaraiosis–a translational proof-of-principal MRI study.
http://onlinelibrary.wiley.com/doi/10.1111/j.1747-4949.2012.00807.x/abstract
Statins and cerebral perfusion in patients with
leukoaraiosis–a translational proof-of-principal MRI study.
B-cell Lymphoma-2 (Bcl-2) is an Essential Regulator of Adult Hippocampal Neurogenesis
Get your researcher involved to increase the number of surviving neurogenesis neurons. Another good dissertation. Only 89 pages.
http://www.ruor.uottawa.ca/fr/bitstream/handle/10393/23287/Ceizar_Maheen_2012_thesis.pdf?sequence=3
ABSTRACT
Of the thousands of dividing progenitor cells (PCs) generated daily in the adult
brain only a very small proportion survive to become mature neurons through the
process of neurogenesis. Identification of the mechanisms that regulate cell
death associated with neurogenesis would aid in harnessing the potential
therapeutic value of PCs. Apoptosis, or programmed cell death, is suggested to
regulate death of PCs in the adult brain as overexpression of B-cell lymphoma 2
(Bcl-2), an anti-apoptotic protein, enhances the survival of new neurons. To
directly assess if Bcl-2 is a regulator of apoptosis in PCs, this study examined the
outcome of removal of Bcl-2 from the developing PCs in the adult mouse brain.
Retroviral mediated gene transfer of Cre into adult floxed Bcl-2 mice eliminated
Bcl-2 from developing PCs and resulted in the complete absence of new neurons
at 30 days post viral injection. Similarly, Bcl-2 removal through the use of nestininduced
conditional knockout mice resulted in reduced number of mature
neurons. The function of Bcl-2 in the PCs was also dependent on Bcl-2-
associated X (BAX) protein, as demonstrated by an increase in new neurons
formed following viral-mediated removal of Bcl-2 in BAX knockout mice. Together
these findings demonstrate that Bcl-2 is an essential regulator of neurogenesis in
the adult hippocampus.
Authorizations .............................................................................................. i
Abstract........................................................................................................ xi
List of Tables ............................................................................................... xiv
List of Figures .............................................................................................. xv
List of Abbreviations..................................................................................... xvii
Acknowledgements...................................................................................... xx
Chapter 1: Introduction ............................................................................ 1
1.1 ..Adult Neurogenesis ........................................................................ 1
1.2 Progenitor Cell (PC) Development in the Hippocampus................. 2
1.3 Cell Death Occurring During Adult Neurogenesis........................... 7
1.4 Apoptosis ....................................................................................... 9
1.5 The Intrinsic Apoptotic Pathway ..................................................... 12
1.6 Players Involved with Apoptosis in Adult Neurogenesis ................. 15
Objectives and Statement of Hypothesis ................................................ 18
Chapter 2: Materials and Methods ........................................................... 19
2.1 Animals .......................................................................................... 19
2.2 Genotyping .................................................................................... 19
2.3 Retroviral Vectors & Injections ....................................................... 20
2.4 Tamoxifen Treatments ................................................................... 22
2.5 Perfusion and Tissue Collection .................................................... 23
2.6 Immunohistochemistry.................................................................... 23
2.7 Quantification Using Microscopy ................................................... 26
2.8 Statistical Analysis ......................................................................... 27
Chapter 3: Results
3.1 Retroviral-Mediated Removal of Bcl-2 Prevents the
Survival of Newborn Mature Neurons ............................................ 28
3.2 Bcl-2 Functions in the Adult Hippocampus in a BAX
xiii
Dependent Manner ........................................................................ 33
3.3 Generation of the Inducible Triple Transgenic Bcl-2
Knockout Mouse ............................................................................ 35
3.4 Removal of Bcl-2 in Nestin-Expressing Cells and their
Progeny Reduces the Recombined, Stem and Immature
Neurons at 12 days ....................................................................... 37
3.5 Removal of Bcl-2 in Nestin-Expressing Cells and Their
Progeny Altered the Mature Neuron Population 30
Days After Removal ....................................................................... 45
Chapter 4: Discussion .............................................................................. 51
4.1 Bcl-2 has a Cell-Autonomous Essential Role in
Adult Neurogenesis ........................................................................ 51
4.2 Bcl-2-Mediated Effects on the Stem-cell Like
Population ...................................................................................... 53
4.3 Differences in Neurogenesis between Floxed
Bcl-2 Mice Infected with Retroviral Cre and
nBcl-2 KO Mice............................................................................... 55
4.4 The Expression of Bcl-2 During Adult Neurogenesis .................... 56
4.5 The Role of Bcl-2 in Regulating Apoptosis in
Adult Neurogenesis ........................................................................ 56
References ................................................................................................. 59
http://www.ruor.uottawa.ca/fr/bitstream/handle/10393/23287/Ceizar_Maheen_2012_thesis.pdf?sequence=3
ABSTRACT
Of the thousands of dividing progenitor cells (PCs) generated daily in the adult
brain only a very small proportion survive to become mature neurons through the
process of neurogenesis. Identification of the mechanisms that regulate cell
death associated with neurogenesis would aid in harnessing the potential
therapeutic value of PCs. Apoptosis, or programmed cell death, is suggested to
regulate death of PCs in the adult brain as overexpression of B-cell lymphoma 2
(Bcl-2), an anti-apoptotic protein, enhances the survival of new neurons. To
directly assess if Bcl-2 is a regulator of apoptosis in PCs, this study examined the
outcome of removal of Bcl-2 from the developing PCs in the adult mouse brain.
Retroviral mediated gene transfer of Cre into adult floxed Bcl-2 mice eliminated
Bcl-2 from developing PCs and resulted in the complete absence of new neurons
at 30 days post viral injection. Similarly, Bcl-2 removal through the use of nestininduced
conditional knockout mice resulted in reduced number of mature
neurons. The function of Bcl-2 in the PCs was also dependent on Bcl-2-
associated X (BAX) protein, as demonstrated by an increase in new neurons
formed following viral-mediated removal of Bcl-2 in BAX knockout mice. Together
these findings demonstrate that Bcl-2 is an essential regulator of neurogenesis in
the adult hippocampus.
Authorizations .............................................................................................. i
Abstract........................................................................................................ xi
List of Tables ............................................................................................... xiv
List of Figures .............................................................................................. xv
List of Abbreviations..................................................................................... xvii
Acknowledgements...................................................................................... xx
Chapter 1: Introduction ............................................................................ 1
1.1 ..Adult Neurogenesis ........................................................................ 1
1.2 Progenitor Cell (PC) Development in the Hippocampus................. 2
1.3 Cell Death Occurring During Adult Neurogenesis........................... 7
1.4 Apoptosis ....................................................................................... 9
1.5 The Intrinsic Apoptotic Pathway ..................................................... 12
1.6 Players Involved with Apoptosis in Adult Neurogenesis ................. 15
Objectives and Statement of Hypothesis ................................................ 18
Chapter 2: Materials and Methods ........................................................... 19
2.1 Animals .......................................................................................... 19
2.2 Genotyping .................................................................................... 19
2.3 Retroviral Vectors & Injections ....................................................... 20
2.4 Tamoxifen Treatments ................................................................... 22
2.5 Perfusion and Tissue Collection .................................................... 23
2.6 Immunohistochemistry.................................................................... 23
2.7 Quantification Using Microscopy ................................................... 26
2.8 Statistical Analysis ......................................................................... 27
Chapter 3: Results
3.1 Retroviral-Mediated Removal of Bcl-2 Prevents the
Survival of Newborn Mature Neurons ............................................ 28
3.2 Bcl-2 Functions in the Adult Hippocampus in a BAX
xiii
Dependent Manner ........................................................................ 33
3.3 Generation of the Inducible Triple Transgenic Bcl-2
Knockout Mouse ............................................................................ 35
3.4 Removal of Bcl-2 in Nestin-Expressing Cells and their
Progeny Reduces the Recombined, Stem and Immature
Neurons at 12 days ....................................................................... 37
3.5 Removal of Bcl-2 in Nestin-Expressing Cells and Their
Progeny Altered the Mature Neuron Population 30
Days After Removal ....................................................................... 45
Chapter 4: Discussion .............................................................................. 51
4.1 Bcl-2 has a Cell-Autonomous Essential Role in
Adult Neurogenesis ........................................................................ 51
4.2 Bcl-2-Mediated Effects on the Stem-cell Like
Population ...................................................................................... 53
4.3 Differences in Neurogenesis between Floxed
Bcl-2 Mice Infected with Retroviral Cre and
nBcl-2 KO Mice............................................................................... 55
4.4 The Expression of Bcl-2 During Adult Neurogenesis .................... 56
4.5 The Role of Bcl-2 in Regulating Apoptosis in
Adult Neurogenesis ........................................................................ 56
References ................................................................................................. 59
The molecular mechanisms of Nogo signaling
Another great dissertation, only 24 pages for your doctor to figure out.
The molecular mechanisms of Nogo signaling
Summary 3
Inhibition of axon regeneration in the CNS 4
Astrocytes and the glial scar 4
Myelin associated inhibitors 4
Nogo, the principal myelin associated inhibitor 5
Nogo is a member of the RTN protein family 6
Nogo structure 6
The stucture of the Nogo RTN domain 6
Nogo-A and B specific domains 7
Membrane topology 7
Nogo receptors 8
Downstream signaling in the CNS 9
Activation of RhoA, the second messenger for cytoskeletal dynamics 9
The RhoA-ROCK pathway and its downstream effectors 10
Activation of Ca2+ and cAMP signaling pathways 11
Signal transduction downstream of Ca2+ and cAMP mediates a switch in axonal response 12
Downstream effectors of cAMP influence neurite outgrowth 12
cAMP levels control regenerative capacity after a preconditioning lesion and during maturation 13
Nogo functions in the nervous system 13
Nogo-A hampers axonal regeneration after CNS injury 13
Roles of Nogo in the developing CNS 14
Nogo regulates plasticity of the adult CNS 15
Nogo-B and C in myelin associated inhibition 15
Specific functions of Nogo-B and C 15
Discussion 17
List of Abbreviations 18
Refrences 19
Summary
Damage to the adult central
nervous system often leads to permanent loss of function. Several inhibitory
factors specific for the CNS prevent regeneration of severed axons and network
connectivity is lost permanently. One obstacle for regenerating neurons is
formed by myelin associated inhibitors; the proteins Nogo, MAG and OMgp, which
are expressed by myelinating oligodendrocytes in the CNS. Of these three, Nogo
is believed to be the main mediator of growth inhibition in the adult CNS. The
nogo gene gives rise to three protein products, the Nogo isoforms A, B and C.
Nogo-A the isoform that functions as an inhibitor for neuronal growth, during
development Nogo-A is involved in axonal guidance and in the uninjured adult
CNS Nogo regulates functional plasticity. Nogo-B and C are less well studied
jet some specific functions are known. Signaling by Nogo-A involves multiple receptors
that activate parallel cascades of downstream effectors. These signaling
pathways ultimately lead to a halt in axon growth. Signaling commences when
Nogo binds to one of its receptors. To date, two receptors for Nogo-A have been
identified, NgR1 and co-receptors LINGO-1 and p75 or TROY, and the receptor
PirB. Via these receptors, multiple signaling routes involving RhoA, cAMP and
Ca2+ are activated. These second messengers and their downstream
effectors determine growth direction and induce growth cone collapse. In vitro studies of Nogo function
confirm its role as an inhibitor of neuronal growth and regeneration. However, in vivo studies of Nogo function in animals
lacking one or more Nogo isoforms show inconsistent regeneration phenotypes. In
contrast, treatment with function blocking anti-Nogo antibodies has profound
and consistent positive effects on regeneration of the CNS and recovery of
motor function. These Nogo blocking antibodies have great therapeutic potential
and are currently being evaluated in clinical trials. The antibodies may soon
be available to patients with CNS injuries and greatly improve their
rehabilitation.
Longitudinal Evaluation of Resting-State fMRI After Acute Stroke With Hemiparesis
I'm not sure what use this is so ask your doctor to figure it out.
http://nnr.sagepub.com/content/early/2012/09/14/1545968312457827.abstract
. Within hours poststroke, patients with motor deficits exhibited significantly lower connectivity than controls (P = .02) and patients with no motor impairment (P
= .03). Connectivity was reestablished after 7 days in recovered (ie,
NIHSS score = 0) participants. After 90 days, recovered
patients exhibited normal motor connectivity;
however, reduced connectivity with subcortical regions associated with
effort
and cognitive processing remained. Conclusion.
Resting-state fMRI within hours of ischemic stroke can demonstrate the
impact of stroke on functional connections throughout
the brain. This tool has the potential to help
select appropriate stroke therapies in an acute imaging setting and to
monitor
the efficacy of rehabilitation.
http://nnr.sagepub.com/content/early/2012/09/14/1545968312457827.abstract
Abstract
Background. Functional magnetic
resonance imaging (fMRI) of motor impairment after stroke strongly
depends on patient effort and capacity
to make a movement. Hence fMRI has had limited use
in clinical management. Alternatively, resting-state fMRI (ie, with no
task) can elucidate the brain’s functional
connections by determining temporal synchrony between brain regions. Objective.
The authors examined whether resting-state fMRI can elucidate the
disruption of functional connections within hours of ischemic
stroke as well as during recovery. Methods.
A total of 51 ischemic stroke patients—31 with mild-to-moderate hand
deficits (National Institutes of Health Stroke Scale
[NIHSS] motor score ≥1) and 20 with NIHSS score of
0—underwent resting-state fMRI at less than 24 hours, 7 days, and 90 days poststroke;
15 age-matched healthy individuals participated in 1
session. Using the resting-state fMRI signal from the ipsilesional
motor
cortex, the strength of functional connections with
the contralesional motor cortex was computed. Whole-brain maps of the
resting-state motor network were also generated and
compared between groups and sessions. Results. Within hours poststroke, patients with motor deficits exhibited significantly lower connectivity than controls (P = .02) and patients with no motor impairment (P
= .03). Connectivity was reestablished after 7 days in recovered (ie,
NIHSS score = 0) participants. After 90 days, recovered
patients exhibited normal motor connectivity;
however, reduced connectivity with subcortical regions associated with
effort
and cognitive processing remained. Conclusion.
Resting-state fMRI within hours of ischemic stroke can demonstrate the
impact of stroke on functional connections throughout
the brain. This tool has the potential to help
select appropriate stroke therapies in an acute imaging setting and to
monitor
the efficacy of rehabilitation.
Results
Myelin associated inhibitors; molecular mechanisms and therapeutic potential
A great thesis, why can't regular stroke researchers come up with novel ideas to research like this? Only 59 pages for your doctor to read and explain to you.
Myelin associated inhibitors; molecular mechanisms and therapeutic potential
Summary
Whereas the peripheral nervous system can readily regenerate after injury, regeneration is very limited in the central nervous system of adult vertebrates. Over the past three decades, it has become clear that this lack of regeneration has a molecular basis. The myelin that provides electrical insulation of neuronal fibers has a different composition in the central nervous system, as compared to peripheral nervous system myelin. Several proteins expressed on myelin have been found to have inhibitory effects for neuronal regeneration and were dubbed myelin-associated inhibitors. The three classical myelin-associated inhibitors (Nogo, MAG and OMgp) were found to signal all three through two distinct receptor complexes, providing a puzzling redundancy for these interactions. This signaling is speculated to be important for stabilizing neuronal circuitry in healthy adult organisms. Other proteins known to be involved in axonal guidance, such as semaphorins, ephrins, netrins and Wnts, as well as extracellular matrix components such as the chondroitin sulfate proteoglycans, have also been shown to have regeneration inhibitory effects. Downstream signaling by neuronal effector proteins culminates in modulation of the cytoskeleton and transcription, explaining the morphological changes of the neurons that are observed upon signaling. The fact that the lack of regeneration has a molecular basis provides prospects for therapeutic intervention to stimulate regeneration for injuries of the central nervous system, like spinal cord injury or stroke. Indeed, a substantial body of different proteins, peptides and small molecules that intervene with the different steps involved in the inhibition of regeneration shows promising effects, both in vitro and in vivo.
This review will discuss the advances made on understanding the lack of regeneration in the central nervous system. After an introduction on the nervous system, injury and regeneration, the molecular mechanisms of inhibition will be discussed. A special focus will be on the three classical myelin associated inhibitors and their receptor complexes, but other molecules that are inhibitory for regeneration will be discussed as well. The current understanding of the downstream signaling cascades of the myelin associated inhibitors will be reviewed and finally, different strategies that demonstrate the therapeutic potential of interfering with these mechanisms will be discussed.
Table of content
Summary ................................................................................................... 2
Table of content .......................................................................................... 3
Introduction ............................................................................................... 4
Molecular Mechanisms ................................................................................. 9
Downstream Events ................................................................................... 32
Therapeutic Potential ................................................................................. 39
Conclusion and Perspectives ....................................................................... 46
List of Abbreviations .................................................................................. 47
Effects of the Sigma-1 Receptor Agonist 1-(3,4-Dimethoxyphenethyl)-4-(3-Phenylpropyl)-Piperazine Dihydro-Chloride on Inflammation after Stroke
Get your researcher to propose a stroke therapy protocol based on this research.
Effects of the Sigma-1 Receptor Agonist 1-(3,4-Dimethoxyphenethyl)-4-(3-Phenylpropyl)-Piperazine Dihydro-Chloride on Inflammation after Stroke
Abstract Top
Activation of the sigma-1 receptor (Sig-1R) improves functional recovery in models of experimental stroke and is known to modulate microglia function. The present study was conducted to investigate if Sig-1R activation after experimental stroke affects mediators of the inflammatory response in the ischemic hemisphere. Male Wistar rats were subjected to transient occlusion of the middle cerebral artery (MCAO) and injected with the specific Sig-1R agonist 1-(3,4-dimethoxyphenethyl)-4-(3-phenylpropyl)piperazinedihydrochloride (SA4503) or saline for 5 days starting on day 2 after MCAO. Treatment did not affect the increased levels of the pro-inflammatory cytokines interleukin 1 beta (IL-1β), tumor necrosis factor alpha (TNF-α), interferon gamma (IFN-γ), interleukin 4 (IL-4), interleukin 5 (IL-5), and interleukin 13 (IL-13) in the infarct core and peri-infarct area after MCAO. In addition, treatment with SA4503 did not affect elevated levels of nitrite, TNF-α and IL-1β observed in primary cultures of microglia exposed to combined Hypoxia/Aglycemia, while the unspecific sigma receptor ligand 1,3-di-o-tolylguanidine (DTG) significantly decreased the production of nitrite and levels of TNF-α. Analysis of the ischemic hemisphere also revealed increased levels of ionized calcium binding adaptor molecule 1 (Iba1) levels in the infarct core of SA4503 treated animals. However, no difference in Iba1 immunoreactivity was detected in the infarct core. Also, levels of the proliferation marker proliferating cell nuclear antigen (PCNA) and OX-42 were not increased in the infarct core in rats treated with SA4503. Together, our results suggest that sigma-1 receptor activation affects Iba1 expression in microglia/macrophages of the ischemic hemisphere after experimental stroke but does not affect post-stroke inflammatory mediators.Maroubra stroke victim recovering with Fishing 4 Therapy
You have to go all the way to Australia to get unusual and decent stroke rehab. Ask your therapist for this.
http://southern-courier.whereilive.com.au/news/story/top-supporting-cast/
Maroubra's Sam Pavone struggled to leave the house after he suffered a stroke two years ago but he has never looked back since discovered Fishing 4 Therapy.
An experienced fisherman, he felt frustrated sitting at home every day for 12 months watching fishing TV shows longing to get back out there.
"I used to get very upset and angry," he said. "Now I'm positive and as the fishing day gets closer I feel more happy and excited."
Not even experiencing another stroke in January this year could stop Mr Pavone from picking up the rod again four months ago.
Australian National Sportsfishing Association NSW made a rehabilitation tool for him out of an old fishing rod recently so he can build-up arm strength and movement.
ANSA NSW special projects officer Tony Steiner said everyone was blown away with Mr Pavone's results.
"Sam had gone from 'Mr Shy' to moving his frame around to all the other attendees making sure baits were on correctly," he said.
"Sam shed a few tears of joy after being able to get back to his passion - that's the power of fishing."
http://southern-courier.whereilive.com.au/news/story/top-supporting-cast/
Maroubra's Sam Pavone struggled to leave the house after he suffered a stroke two years ago but he has never looked back since discovered Fishing 4 Therapy.
An experienced fisherman, he felt frustrated sitting at home every day for 12 months watching fishing TV shows longing to get back out there.
"I used to get very upset and angry," he said. "Now I'm positive and as the fishing day gets closer I feel more happy and excited."
Not even experiencing another stroke in January this year could stop Mr Pavone from picking up the rod again four months ago.
Australian National Sportsfishing Association NSW made a rehabilitation tool for him out of an old fishing rod recently so he can build-up arm strength and movement.
ANSA NSW special projects officer Tony Steiner said everyone was blown away with Mr Pavone's results.
"Sam had gone from 'Mr Shy' to moving his frame around to all the other attendees making sure baits were on correctly," he said.
"Sam shed a few tears of joy after being able to get back to his passion - that's the power of fishing."
Sunday, September 23, 2012
Reneuron (RENE.L) Files 2 Clinical Trial Applications in UK
Up to you in the UK if you want to get involved. Ask about the intramuscular injection site, why there?
http://www.proactiveinvestors.com/columns/scimitar-equity/2101/reneuron-renel-files-2-clinical-trial-applications-in-uk-2101.html
http://www.proactiveinvestors.com/columns/scimitar-equity/2101/reneuron-renel-files-2-clinical-trial-applications-in-uk-2101.html
ReNeuron submitted 2 applications to UK regulatory authority to commence multi-site ischemic stroke P2 clinical trial to examine efficacy of ReN001 and ReN009 for Critical Limb Ischemia (CLI).
The
ReN001 ischemic stroke trial is designed to recruit from a well-defined
population of patients between 2 and 4 months after their stroke, which
they believe will be the optimum treatment window for the therapy.
The
ongoing PISCES study with ReN001 continues on plan following the
commencement of treatment of patients in the penultimate dose cohort
last month, there remain no cell-related serious adverse events reported
in any of the patients treated to date. The independent Data Safety
Monitoring Board for the study will shortly make its recommendation
regarding treatment of the remaining patients in the penultimate dose
cohort. In June of this year, interim data from the PISCES study from
the first 5 patients treated was presented by the Glasgow clinical team
at the 10th Annual Meeting of the International Society for Stem Cell
Research (ISSCR) in Yokohama, Japan. Reductions in neurological
impairment and spasticity were observed in all 5 patients compared with
their stable pre-treatment baseline performance and these improvements
were sustained in longer term follow-up.
RENE.L
also submitted application to UK regulatory authority to commence a P1
clinical trial of ReN009 stem cell therapy for critical limb ischemia
(CLI). These patients will be administered via straightforward
intramuscular injection of the cells.
The Bottom Line: But … it is a competitive trial and market arena … Athersys (ATHX) is
also pursuing a P2 clinical trial in ischemic stroke. ATHX believes its
MultiStem therapy can help limit the associated damage that occurs post
ischemic stroke by down-regulating the immune response that follows.
ATHX is now conducting a 140-patient trial with data expected in 2H13.
MultiStem is a drug-like stem cell product that is produced by obtaining
a special class of stem cells from healthy, consenting donors. These
cells express proteins and other factors involved in tissue repair and
immune system regulation and act through multiple mechanisms, such as
protecting damaged or injured cells, reducing inflammation and promoting
new blood vessel formation in areas of ischemic injury. Aastrom (ASTM)is
recruiting for its P3 CLI trial which is on-going and headed to
completion. This trial will assess the efficacy and safety of
ixmyelocel-T in CLI patients. REVIVE will be conducted in the United
States across 80 sites and is targeting an enrollment of just under 600
no-option CLI patients. REVIVE represents the largest randomized,
double-blind, placebo controlled, multicenter study ever conducted in
patients with CLI. Pluristem (PSTI) reported
CLI P1 results in 11/11 of 27 patients in Germany. The PLX-PAD cells
therapy failed in 4 of the 27 patients, giving a rate was 85.2% after 12
months for the PLX-PAD cells therapy. However, little has been heard
since … stated it was planning to conduct its P2/3 trials for CLI in the
2H11.
Neocortical neurogenesis and neuronal migration
This is way over my head so ask your researcher to dumb it down to a stroke protocol.
http://onlinelibrary.wiley.com/doi/10.1002/wdev.88/full
http://onlinelibrary.wiley.com/doi/10.1002/wdev.88/full
INTRODUCTION
A
prominent trait of the neocortex is its complex yet well-organized
cellular architecture, the formation of which relies on the production
and positioning of its diverse neuronal populations. There are two major
groups of neurons in the neocortex—glutamatergic excitatory neurons and
γ-aminobutyric acid (GABA)-ergic inhibitory interneurons,
which are responsible for generating excitation and inhibition,
respectively. Excitatory neurons constitute the vast majority (∼70–80%)
of neocortical circuit neurons and are responsible for generating the
output. On the other hand, inhibitory interneurons provide a rich
variety of inhibitions that shape the output of functional circuits.
Proper neocortex function critically depends on the production and
positioning of a correct number of excitatory and inhibitory neurons,
which largely occur during the embryonic stages.
With
the advent of improved fate-mapping tools, including genetically
engineered mice, excitatory and inhibitory neurons in the neocortex were
found to arise from different developmental lineages. In rodents, the
progenitor cells of these two neuronal populations are fully segregated
in space (Figure 1).
Excitatory neurons are generated in the proliferative zone of the
dorsal telencephalon and then migrate radially to constitute the future
neocortex. In contrast, inhibitory interneurons are produced in the
proliferative zone of the ventral telencephalon and migrate tangentially
to reach the neocortex, where they coassemble with excitatory neurons
into functional circuits. This spatial segregation in the excitatory and
inhibitory neuron progenitors no doubt further complicates the
coordinated production and positioning of these neurons.
Neurogenesis, inflammation and behavior
Ask your doctor to apply this to your recovery.
http://www.sciencedirect.com/science/article/pii/S0889159112004308
http://www.sciencedirect.com/science/article/pii/S0889159112004308
Abstract
Before
the 1990s it was widely believed that the adult brain was incapable of
regenerating neurons. However, it is now established that new neurons
are continuously produced in the dentate gyrus of the hippocampus and
olfactory bulb throughout life. The functional significance of adult
neurogenesis is still unclear, but it is widely believed that the new
neurons contribute to learning and memory and/or maintenance of brain
regions by replacing dead or dying cells. Many different factors are
known to regulate adult neurogenesis including immune responses and
signaling molecules released by immune cells in the brain. While immune
activation (i.e., enlargement of microglia, release of cytokines) within
the brain is commonly viewed as a harmful event, the impact of immune
activation on neural function is highly dependent on the form of the
immune response as microglia and other immune-reactive cells in the
brain can support or disrupt brain function depending on the phenotype
and behavior of the cells. For instance, microglia that express an
inflammatory phenotype generally reduce cell proliferation, survival and
function of new neurons whereas microglia displaying an alternative
protective phenotype support adult neurogenesis. The present review
summarizes current understanding of the role of new neurons in cognition
and behavior, with an emphasis on the immune system’s ability to
influence adult hippocampal neurogenesis during both an inflammatory
episode and in the healthy uninjured brain. It has been proposed that
some of the cognitive deficits associated with inflammation may in part
be related to inflammation-induced reductions in adult hippocampal
neurogenesis. Elucidating how the immune system contributes to the
regulation of adult neurogenesis will help in predicting the impact of
immune activation on neural plasticity and potentially facilitate the
discovery of treatments to preserve neurogenesis in conditions
characterized by chronic inflammation.
Saturday, September 22, 2012
A complex study of the movement biomechanics in patients with post-stroke hemiparesis
I don't know what this means, that's what your doctor is for. And demand to have it explained to you. The original seems to be in Russian so don't back down when they profess not to be able to do it. I expect my medical staff to know more than I do and so should you.
http://www.ncbi.nlm.nih.gov/pubmed/22983241
http://www.ncbi.nlm.nih.gov/pubmed/22983241
Abstract
The authors present results of a pilot study on biomechanics of non-cyclic movements of the human consequent verticalization in the ontogenesis of patients with post-stroke hemiparesis (10 patients in the acute stage of cerebral stroke) and 10 healthy volunteers without neurologic and orthopedic pathology. Some movements of therapeutic exercises Balance (a model of ontogenetic kinesitherapy) have been selected for the study. Cinematic parameters have been recorded using a system of motion 3D video analysis, a kinematic model was build in accordance to standard protocols. The skin (native and straightened) electromyogram (EMG) was recorded synchronously with kinematic data using 16-channel electromyography from the following pairs of muscles: mm. sternocleido-mastoideus, trapezius (горизонтальная порция), biceps brachii, triceps brachii, rectus femoris, adductor magnus. Major differences in the EMG picture between patients and controls were: 1) the EMG "monotony" with the involvement of multiple additional muscles in locomotions with the prevalence of the peculiar "tonic" muscle activity (low amplitudes without distinct peaks), stretching along the whole cycle of movement. In controls, EMG demonstrated variability and had mostly "phasic" character with distinct 1 or 2 peaks; 2) the asymmetry of EMG profile in symmetric movements. i.e. when performed simultaneously from the right and from the left sides. The latter feature may be considered as predictive because it was never found in healthy people. It allows to identify objectively weak muscles even in the absence of visible parethis during the routine neurological examination.PETS HELP STROKE PATIENTS
Mostly assumptions and feel good comments in the article. No scientific backup at all.
http://www.observer.org.sz/index.php?news=43264
http://www.observer.org.sz/index.php?news=43264
Is early speech and language therapy after stroke a waste?
In we follow evidence-based medicine then we are going to need lots more research if we want therapy at all.
http://www.bmj.com/content/345/bmj.e4870?view=long&pmid=22807163
http://www.bmj.com/content/345/bmj.e4870?view=long&pmid=22807163
Research
into rehabilitation is a relatively young discipline and there are
still few centres of academic excellence in stroke rehabilitation.
Randomised trials are difficult to conduct in this area. Large
variations in patients and disease characteristics make designing trials
tricky(So What); blinding may be difficult; and identifying appropriate control
interventions and ensuring that interventions are standardised,
especially in multi-site studies, is challenging. However, such problems
are not unique to rehabilitation research and can be overcome using
complex intervention evaluation methods, as has been shown in other
areas of stroke care.1 In a linked
research paper (doi:10.1136/bmj.e4407), Bowen and colleagues report the
findings of the ACT NoW (Assessing Communication Therapy in the North
West) study, which is a large scale multicentre randomised controlled
trial of speech and language therapy in the rehabilitation of patients
after stroke.2 This study is welcome
because, as with other treatment interventions, it is essential that
rehabilitation is subjected to rigorous scrutiny.
Single
case studies, observational studies, and small single centre randomised
trials provide weak evidence for guiding clinicians and planners of
care, and they cannot answer fundamental questions about how and what
services should …
Subscribe to:
Posts (Atom)