NO, NO, NO! Don't predict failure to recover. Deliver interventions that lead to recovery. I can predict nonuse of the arm with one question; Is your hand functional? Y/N? If not there then deliver the protocols that allow full use of the hand. Do the research in the correct order; hand, then arm.
So solve the problems in the correct order! Duh! And don't give me crap about proximal to distal.
Predicting Arm Nonuse in Individuals with Good Arm Motor Function after Stroke Rehabilitation: A Machine Learning Study


1
School of Occupational Therapy, National Taiwan University College of Medicine, 17, F4, Xu-Zhou Road, Taipei 100, Taiwan
2
Department of Speech Language Pathology
and Audiology, National Taipei University of Nursing and Health
Sciences, 365, Mingde Road, Taipei 112, Taiwan
3
Department of Occupational Therapy,
I-Shou University College of Medicine, 8, Yida Road, Jiaosu Village,
Yanchao District, Kaohsiung 824, Taiwan
4
Department of Physical Medicine and Rehabilitation, College of Medicine, National Taiwan University, Taipei 10048, Taiwan
5
Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, Taipei 10048, Taiwan
6
Institute of Biomedical Engineering and
Nanomedicine, National Health Research Institutes, 35, Keyan Road,
Zhunan District, Miaoli 350, Taiwan
7
Department of Physical Medicine and
Rehabilitation, Chang Gung Memorial Hospital at Linkou, 5 Fusing Street,
Gueishan District, Taoyuan 333, Taiwan
8
Graduate Institute of Early
Intervention, College of Medicine, Chang Gung University, 259 Wenhua 1st
Road, Gueishan District, Taoyuan 333, Taiwan
9
Division of Occupational Therapy,
Department of Physical Medicine and Rehabilitation, National Taiwan
University Hospital, 7 Chung-Shan South Road, Taipei 100, Taiwan
*
Author to whom correspondence should be addressed.
Int. J. Environ. Res. Public Health 2023, 20(5), 4123; https://doi.org/10.3390/ijerph20054123
Received: 16 January 2023
/
Revised: 17 February 2023
/
Accepted: 23 February 2023
/
Published: 25 February 2023
(This article belongs to the Section Disabilities)
{kind=link}
{kind=link}
Abstract
Many stroke survivors demonstrate arm nonuse despite
good arm motor function. This retrospective secondary analysis aims to
identify predictors of arm nonusers with good arm motor function after
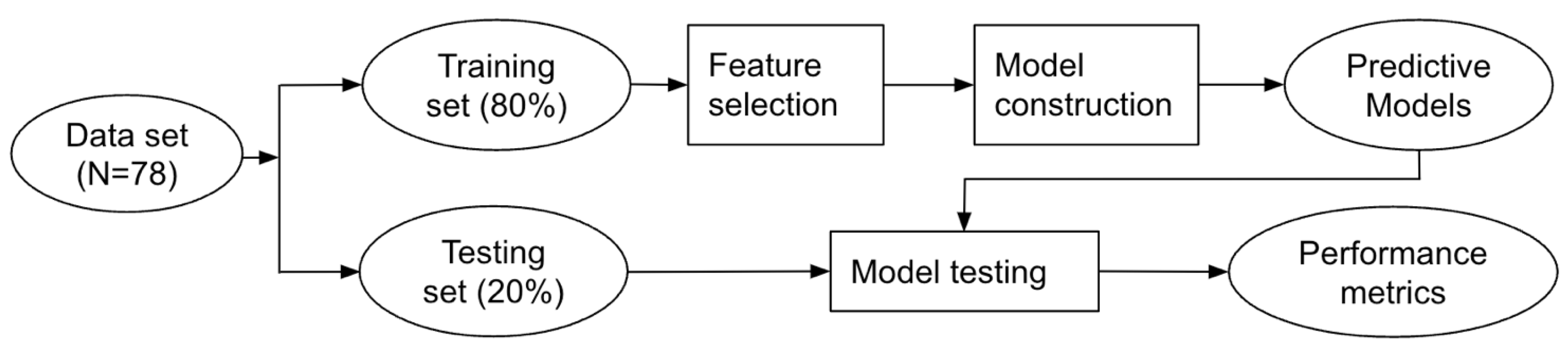
stroke rehabilitation. A total of 78 participants were categorized into 2
groups using the Fugl-Meyer Assessment Upper Extremity Scale (FMA-UE)
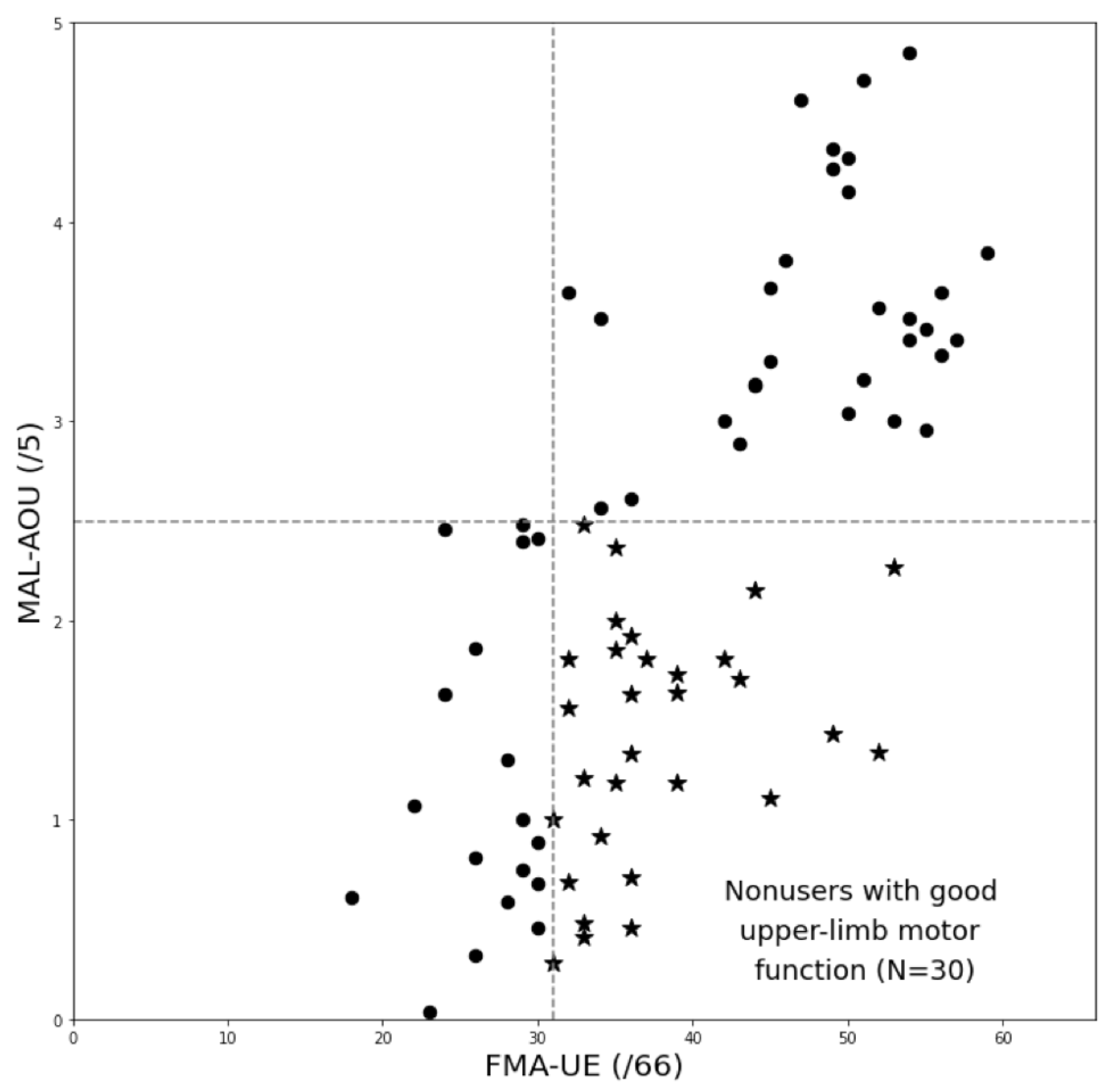
and the Motor Activity Log Amount of Use (MAL-AOU). Group 1 comprised
participants with good motor function (FMA-UE ≥ 31) and low daily upper
limb use (MAL-AOU ≤ 2.5), and group 2 comprised all other participants.
Feature selection analysis was performed on 20 potential predictors to
identify the 5 most important predictors for group membership.
Predictive models were built with the five most important predictors
using four algorithms. The most important predictors were
preintervention scores on the FMA-UE, MAL–Quality of Movement, Wolf
Motor Function Test-Quality, MAL-AOU, and Stroke Self-Efficacy
Questionnaire. Predictive models classified the participants with
accuracies ranging from 0.75 to 0.94 and areas under the receiver
operating characteristic curve ranging from 0.77 to 0.97. The result
indicates that measures of arm motor function, arm use in activities of
daily living, and self-efficacy could predict post intervention arm
nonuse despite good arm motor function in stroke. These assessments
should be prioritized in the evaluation process to facilitate the design
of individualized stroke rehabilitation programs to reduce arm nonuse.
1. Introduction
Stroke is a leading cause of disability [1] that can lead to chronic arm impairment [2,3]. Reduced arm function negatively affects stroke survivors’ quality of life [4].
A significant proportion of stroke survivors perceived nonuse in the
affected arm as a major problem at 4 years after stroke [2].
Studies have reported constraint-induced movement therapy and its
variants were effective in reducing arm nonuse and improving functional
independence and quality of life in individuals with stroke [5,6].
Neurobiological changes corresponding to improvement in arm use after
constraint-induced therapy were also observed with brain imaging [6].
Recently, researchers also advocated for a paradigm shift in stroke
rehabilitation toward self-practice to reduce arm nonuse following motor
rehabilitation [7].
However, early identification of individuals with stroke who may
benefit the most from these programs is challenging. In the context of
precision medicine, if individuals who are likely to develop arm nonuse
can be identified early in the course of rehabilitation, the information
would be able to guide and shape the individualized rehabilitation
program.
Researchers have strived to
investigate the prediction of arm nonuse in individuals with stroke.
Many factors were found or proposed as being associated with the
development of arm nonuse across the phases (i.e., acute, subacute, and
chronic) after stroke. The factor with the most empirical support was
upper-limb motor function. Substantial evidence supports the association
between baseline or postintervention arm motor function and the amount
of use or postintervention amount of use in the affected limb [8,9,10].
In the acute phase, age, stroke severity, sensory impairment, degree of
disability at discharge, and hand grip strength were associated with
the development of arm nonuse at 90 days after discharge [11,12].
In chronic stroke, upper-limb motor dysfunction, dependence in
activities of daily living, and participants’ own perceived upper-limb
function were associated with activities in the affected upper limb
measured by wrist-worn accelerometers [13,14]. Self-efficacy was found to predict arm nonuse in a small group of participants [8] and to moderate the predicting relationship between upper-limb motor function and ratings of daily upper-limb use [15].
Emotional state, such as depression, was discussed as a potential
factor in the context that it may affect compliance with
constraint-induced movement therapy [16].
Other factors for daily upper-limb use after stroke rehabilitation,
such as motivation, health behaviors, and environmental support, were
also proposed but not explicitly tested [17].
Despite
strong evidence suggesting the association between upper-limb motor
function and daily use, good upper-limb motor function does not
translate directly into more use of the affected limb. Studies have
identified participants who demonstrated low daily use of the affected
limb despite having good upper-limb motor function [18,19].
Some patients showed improvement in upper-limb function after
rehabilitation, but continued to demonstrate low daily use of the
affected limb [13,20].
This makes the prediction of nonuse a particularly challenging task.
There are a few possible reasons behind the challenge. First, the
relationship between arm function and arm use after stroke may be
nonlinear [21,22] and may be subject to the moderating effects of other factors [15]. Second, the theoretical background that arm nonuse after stroke is learned [23]
predicts that upper-limb motor function cannot be a sole predictor.
Findings from earlier studies supported factors other than upper-limb
motor function played a role in daily upper-limb activity [13,18].
Nevertheless, it may be a strong enough predictor to mask others,
making it difficult to detect ancillary but important factors using
traditional regression models.
The advances in
artificial intelligence have provided us with another tool for data
analysis, machine learning. Unlike traditional statistics, machine
learning uses multidimensional linear and nonlinear methods to find
patterns in the data [24],
striving to achieve as high an accuracy as possible. It has the
potential to identify factors that have nonlinear, complex relationships
with upper-limb activity and achieve a high predicting capacity.
This
study used machine learning methods to investigate predictors that can
help identify individuals that were likely to develop arm nonuse but had
good arm motor function after stroke rehabilitation. As discussed in
the previous paragraphs, many potential predictors could be considered.
We searched our database accumulated in the past few years to locate
data with a set of likely predictors according to the literature.
Furthermore, we grouped our participants in the database into two
predefined groups according to their postintervention assessment
results: those with low upper-limb use and good upper-limb motor
function in the affected arm, and all others. We were interested in
using preintervention measures to predict which patients would be likely
to develop arm nonuse despite good upper-limb motor function after
intervention. We hypothesize that measures other than motor function
will emerge as important predictors for the classification. By doing so,
we anticipate the results will inform clinical care planning when
addressing personal and environmental factors in addition to motor
function in the design of client-centered individualized rehabilitation
programs.
More at link.
No comments:
Post a Comment