Totally wrong focus, you determine exactly what interventions deliver recovery and writeup the protocols on them. This trying to predict recovery is totally fucking useless. I'd fire you all!
Therapeutic Effects of Robotic-Exoskeleton-Assisted Gait Rehabilitation and Predictive Factors of Significant Improvements in Stroke Patients: A Randomized Controlled Trial


1
Department of Physical Medicine and Rehabilitation, Taichung Veterans General Hospital, Taichung City 40705, Taiwan
2
Department of Electronics and Electrical
Engineering, Institute of Electrical and Control Engineering, Center for
Intelligent Drug Systems and Smart Bio-devices (IDS2B) in College of
Biological Science and Technology, National Yang Ming Chiao Tung
University, Hsinchu 30010, Taiwan
3
Biostatistics Task Force, Taichung Veterans General Hospital, Taichung City 40705, Taiwan
4
School of Medicine, National Yang Ming Chiao Tung University, Taipei 11221, Taiwan
5
Intelligent Long Term Medical Care
Research Center, Department of Post-Baccalaureate Medicine, College of
Medicine, National Chung Hsing University, Taichung City 40227, Taiwan
*
Author to whom correspondence should be addressed.
Bioengineering 2023, 10(5), 585; https://doi.org/10.3390/bioengineering10050585
Received: 24 April 2023
/
Revised: 6 May 2023
/
Accepted: 10 May 2023
/
Published: 12 May 2023
(This article belongs to the Special Issue Extended Reality Technologies, Medical Robotics Solutions, and Deep Learning in Translational Medicine)
Abstract
Robotic-exoskeleton-assisted gait rehabilitation
improves lower limb strength and functions in post-stroke patients.
However, the predicting factors of significant improvement are unclear.
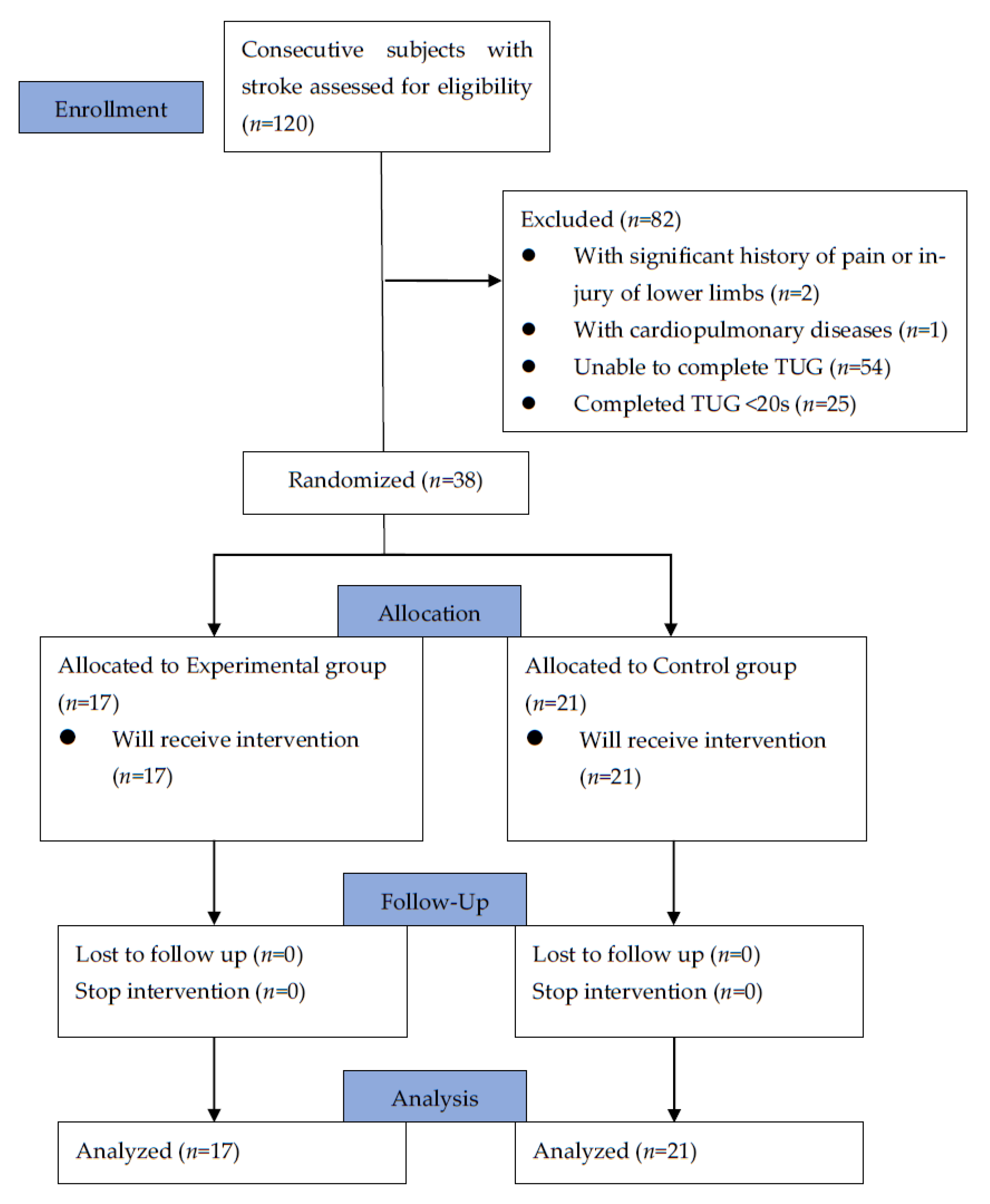
We recruited 38 post-stroke hemiparetic patients whose stroke onsets
were <6 months. They were randomly assigned to two groups: a control
group receiving a regular rehabilitation program, and an experimental
group receiving in addition a robotic exoskeletal rehabilitation
component. After 4 weeks of training, both groups showed significant
improvement in the strength and functions of their lower limbs, as well
as health-related quality of life. However, the experimental group
showed significantly better improvement in the following aspects: knee
flexion torque at 60°/s, 6 min walk test distance, and the mental
subdomain and the total score on a 12-item Short Form Survey (SF-12).
Further logistic regression analyses showed that robotic training was
the best predictor of a greater improvement in both the 6 min walk test
and the total score on the SF-12. In conclusion,
robotic-exoskeleton-assisted gait rehabilitation improved lower limb
strength, motor performance, walking speed, and quality of life in these
stroke patients.

{kind=link}
{kind=link}
{kind=link}
1. Introduction
According
to the World Health Organization, stroke continues to rank second among
the top 10 causes of death worldwide, behind only ischemic heart
disease [1]. However, while stroke prevalence has increased, its mortality has actually decreased [2,3].
Therefore, many stroke survivors are left with post-stroke sequelae,
such as pain syndromes, aphasia, dysphagia, depression, cognitive
impairment, urinary incontinence, epilepsy, apraxia, neglect syndrome,
and function impairment in upper and lower limbs. These post-stroke
sequelae can cause long-term disability [4]
and impose a great burden on their caregivers and families. Among
various post-stroke sequelae, gait disturbance is the most concerning
one for the patients [5].
Characteristics of post-stroke gait abnormality include hip hiking with
leg circumduction, reduced foot clearance during swing phase, knee
hyperextension during stance phase [6], and inadequate propulsion of the leg during pre-swing [7].
These gait abnormalities require that subjects expend more energy to
walk and perform daily activities, leading to their frustration and
depression [5,8].
Gait
rehabilitation is therefore crucial for stroke survivors. To facilitate
motor recovery, traditional approaches include neuro-developmental
treatment [9], Brunnstrom movement therapy [10], proprioceptive neuromuscular facilitation [11], motor relearning programs [12], and the Rood method’s cutaneous stimulation technique [13].
These rehabilitation programs have been practiced by physical
therapists for dozens of years. However, according to the landmark
guidelines published by the American Heart Association/American Stroke
Association in 2016, the therapeutic effects of these traditional
approaches still cannot be established (Classification of recommendation
IIb; Level of evidence B) [14].
On the contrary, it is highly recommended that post-stroke patients
with gait limitations receive intensive and repetitive task training
(Classification of recommendation I; Level of evidence A) [14],
which is very physically demanding for therapists. Therefore, the
duration of this highly helpful training technique is greatly dependent
on the physical fitness of therapists. Hence, one recommended tool to
deal with this problem is robot-assisted movement training according to
the above-mentioned guidelines (Classification of recommendation IIb;
Level of evidence A) [14].
Robotic-assisted gait training devices are attracting growing attention
as they provide repetitive and intensive training while reducing the
need for physical support by therapists [15].
Furthermore, some robotic devices can even accurately and objectively
measure a patient’s physical performance and gait parameters during
training. If combined with physiotherapy, these devices are believed to
help more stroke survivors walk independently than those receiving only
physiotherapy or standard care [16].
Recent evidence has suggested that patients in the first three months
after a stroke, or those who cannot walk initially, benefit the most
from robotic-assisted gait training [16].
Robotic-assisted
gait training is categorized into exoskeleton and end-effector types,
suitable respectively for different situations [17].
The exoskeleton type is used more frequently for patients with profound
weakness, while the end-effector type is used more often for those with
mild weakness [18].
End-effectors are attached to the distal parts of the extremities only,
while the exoskeletons are attached to bilateral whole lower limbs [19].
The exoskeleton type is further divided into two subcategories: the
treadmill-based exoskeleton robot and the orthotic exoskeleton. The
treadmill-based robotic device allows movement training in merely one
sagittal plane, which thus limits its therapeutic training effect on
trunk balance. Patients can only be guided through a predetermined gait
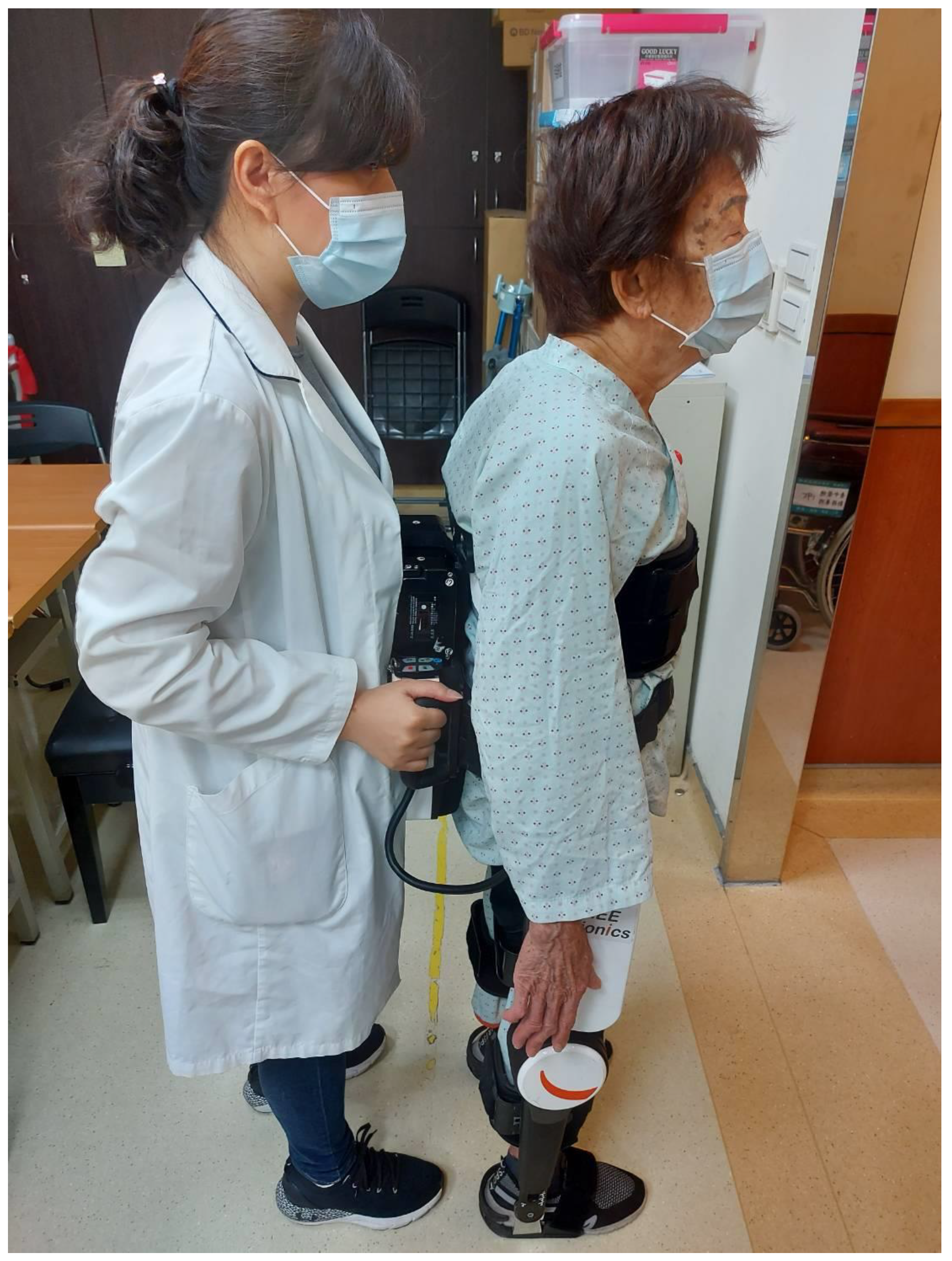
trajectory instead of walking volitionally. On the other hand, the
orthotic exoskeleton allows patients to practice daily activities such
as overground walking, sit to stand, stand to sit, and stairs climbing [19,20].
Nevertheless, a physical therapist needs to be involved more deeply
during the training session in order to maintain the balance of the
patient. The safety issue is thus more of a concern when using this type
of robotic walking device. In this study, we used an orthotic
exoskeleton for robotic-exoskeleton-assisted gait training.
Despite various studies that have been performed on the therapeutic effects of robotic gait training in the past [19],
none have yet explored the predicting factors of significant
improvement for those patients whose onset of stroke is within 6 months.
The primary purpose of this study was to examine the effectiveness of
robotic-exoskeleton-assisted gait training on the strength of lower
limbs, walking speed, motor function performance, and quality of life in
stroke rehabilitation. The second purpose was to determine predicting
factors of significant improvement in post-stroke patients. We
hypothesized that robotic-assisted gait training brings better strength
recovery and functional improvement.
More at link.
No comments:
Post a Comment