Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 32,416 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke. DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
Tuesday, December 10, 2019
Relearning functional and symmetric walking after stroke using a wearable device: a feasibility study
Sounds cool and if this can be done in 12 training sessions then if might be the only therapy that can be successfully accomplished in the hospital. But is your stroke doctor up-to-date enough to bring this in for use?
Gait
impairment is a common consequence of stroke and typically involves a
hemiparetic or asymmetric walking pattern. Asymmetric gait patterns are
correlated with decreased gait velocity and efficiency as well as
increased susceptibility to serious falls and injuries.
Research Question
This
paper presents an innovative device worn on a foot for gait
rehabilitation post stroke. The device generates a backward motion to
the foot, which is designed to exaggerate the existing step length
asymmetry while walking over ground. We hypothesize this motion will
decrease gait asymmetry and improve functional walking in individuals
with chronic stroke.
Methods
Six
participants with chronic stroke, more than one year post stroke,
received four weeks of gait training with three sessions per week. Each
session included 30 min of walking over ground using the wearable
device. Gait symmetry and functional walking were assessed before and
after training.
Results
All
participants improved step length symmetry, and four participants
improved double limb support symmetry. All participants improved on all
three functional outcomes (gait velocity, Timed Up and Go Test, and
6-Minute Walk Test), and five participants improved beyond the minimal
detectable change or meaningful change in at least one functional
outcome.
Conclusion
The
results indicate that the presented device may help improve stroke
patients’ walking ability and warrant further study. A gait training
approach using this new device may enable and expand long-term
continuous gait rehabilitation outside the clinic following stroke.
Each
year approximately 800,000 Americans experience a new or recurrent
stroke, and an estimated six million are living with gait impairments
from a stroke [1]. One such disability is a ‘hemiparetic’ gait [2], which can be characterized by asymmetries in gait measures such as step length and support times [3, 4]. Hemiparetic gait is correlated with decreased gait velocity [5, 6], reduced walking efficiency [7], increased joint and bodily degradation [8], and increased susceptibility to injuries and falls [9, 10].
While
patients and health providers desire effective gait therapy, few
effective long-term remedies have been identified. Treatments of gait
commonly rely on traditional rehabilitation approaches, such as the
Bobath method [11, 12] and lower limb strength training [13, 14],
to re-train walking patterns. Unfortunately, results are inconsistent
across patient populations with these treatment options, and there are
not set devices facilitating these treatments. Some other gait
correction methods currently being studied include Constraint Induced
Movement Therapy [15, 16], body-weight support [17], robotic [18], functional electrical stimulation [19], transcranial magnetic stimulation [20], and full-body gait exoskeletons [21].
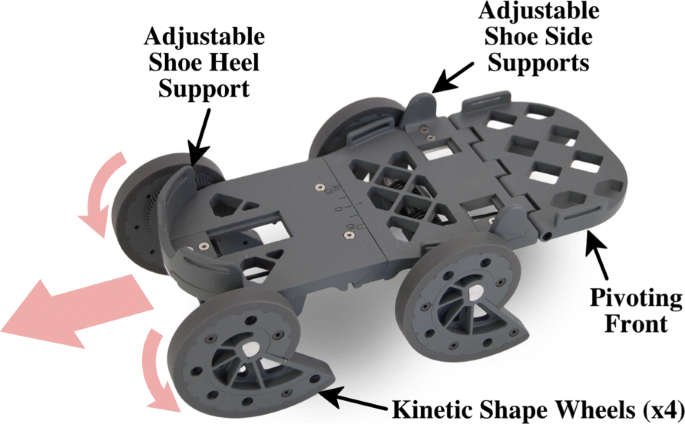
In this paper, we present a novel device (shown in Fig. 1)
designed to help individuals post stroke re-learn how to walk with
little to no therapeutic infrastructure needed. Unlike many of the
existing gait rehabilitation devices, this device is passive, portable,
wearable, and does not require any external energy. It functions by
moving the nonparetic foot backward while the individual walks over
ground [22]. The backward motion of the shoe is generated passively by redirecting the wearer’s downward force during stance phase [23].
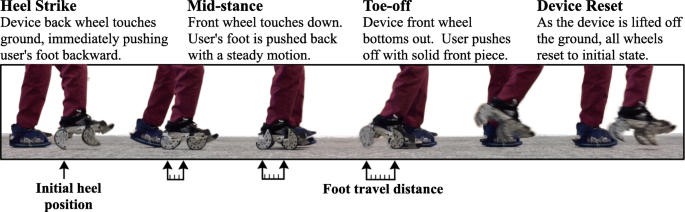
Since the motion is generated by the wearer’s force, the person is in
control, which allows easier adaptation to the motion, but this also
causes the speed to vary slightly from person to person. The generated
motion is demonstrated in Fig. 2. A height and weight matched shoe is attached to the paretic foot, but does not generate any motion.
Fig. 1
Photo of the rehabilitative shoe that is worn on the nonparetic foot
As
the wearer takes a step, the device pushes the nonparetic foot backward
during stance. This exaggeration of the step length asymmetry is
hypothesized to result in a more symmetric gait pattern once the shoe is
removed. In addition, the shoe works to strengthen the paretic leg by
slightly destabilizing the nonparetic leg, which encourages the wearer
to use their paretic leg more. A flexible height and weight matched
platform worn on the paretic foot equalizes the added height and weight
of the device
We
hypothesize that this shoe helps with gait relearning in several ways.
First, the backward motion exaggerates step length asymmetry such that
some of the resulting spatiotemporal aspects of gait will be more
symmetric once the shoe is taken off. This can be thought of as a
version of error augmentation [18, 24]
where the asymmetric step length is exaggerated. Secondly, the motion
of the shoe encourages the use of the paretic side by making it harder
to walk on the nonparetic side. Thirdly, it is untethered and portable,
so it enables rehabilitation in a variety of locations. Making
rehabilitation available in more locations should improve the
context-dependent learning [25]
so patients are relearning gait in the same places that they will
generally be walking. This context should also help generalize the
knowledge to real-world scenarios instead of just the laboratory
setting. Fourthly, the device could enable patients to work on their
rehabilitation with greater frequency and for a longer duration than
currently available methods. Consistent, regular rehabilitation sessions
have been shown to lead to enhanced rehabilitation effects [26].
Furthermore, neural repatterning is known to improve with just one
session per sleep cycle through motor memory consolidation [27],
and thus the increased ability to use the device daily should have
beneficial learning effects compared to less frequent visits to a
clinic. This feasibility study is conducted in the clinic to focus on
the first two points. A future study to be done in participants’ own
homes will evaluate the third and fourth points.
The shoe design has been presented previously [28, 29] along with evaluations on unimpaired participants [30],
and a model of passive dynamics of walking was used to compare the shoe
motions to a split-belt treadmill and normal walking [22].
This paper presents a feasibility study showing how the gait of six
individuals with chronic stroke changed when using the device for 12
sessions over four weeks.
Methods
Participants
Details about the six participants recruited into the study are shown in Table 1.
All participants signed a consent form that was approved by the Western
Institutional Review Board prior to the study. Consent took place at
the University of South Florida. Recruitment of participants occurred
from 2015–2016. All experiments were completed by 2017.
Inclusion
criteria included: (1) age 21–80, (2) one or more cerebral strokes, (3)
a stroke at least six months prior to enrollment, (4) gait asymmetry
greater than 2.5% step length or stance phase based on the pre-test, but
able to walk either with or without a cane for at least five minutes,
(5) no evidence of uncompensated hemianopsia, tested by using Pedretti’s
method [31], (6) no evidence of severe (less than 16 in the Folstein Mini-Mental Status Exam) cognitive impairment [32]
or language dysfunction that would interfere with understanding the
instructions, and (7) no evidence of neglect, tested by being asked to
copy a simple drawing of a house [33].
Exclusion criteria included: (1) orthopedic or pain conditions, (2)
uncontrolled seizures, (3) metal implants (e.g., stents, clips,
pacemaker), (4) pregnancy, (5) any condition that makes balance
unstable, and (6) uncorrected visual impairments.
Experimental setup
The
study consisted of one baseline gait evaluation (pre-test) followed by
four weeks of training on the rehabilitative shoe for three sessions per
week. A post training gait evaluation (post-test) was conducted three
to five days after the last training session. All trainings and tests
were performed at the Tampa campus of the University of South Florida.
Training sessions
Each
of the 12 training sessions consisted of six bouts of walking while
wearing the rehabilitative shoe for five minutes with approximately two
minute breaks in between bouts. The device was attached to the
participant’s nonparetic foot. A height and weight matched shoe was
attached to the paretic foot. Each shoe was secured to the foot with
Velcro straps. Figure 2
shows an example of a participant walking during the training session. A
licensed physical therapist trained for walking assistance walked next
to each participant and loosely held a gaitbelt that the participant was
wearing during all training bouts to ensure participant safety. Vital
signs (i.e., heart rate, blood pressure, respiratory rate, and oxygen
saturation) were measured before the first training bout and after each
bout of walking on the device to ensure participant safety and monitor
their response. The modified Borg Rating of Perceived Exertion Scale [34] was also used as a self-reported subjective measure of physical exertion.
Gait evaluations and data analysis
We
evaluated three spatiotemporal gait measures and three functional
measures of gait before and after training. An 8 meter ProtoKinetics
Zeno Walkway System (ProtoKinetics LLC, Havertown, PA) measured the gait
patterns during each evaluation. The participant was instructed to walk
over the walkway five times at his/her comfortable gait velocity. The
three functional measures included three repetitions of the Timed Up and
Go (TUG) test, one 6-Minute Walk Test (6MWT), and gait velocity was
measured during the five repetitions on the ProtoKinetics Zeno Walkway
System. Note that participant 5 did not complete the TUG or 6MWT during
the followup visit.
The percentage of asymmetry for the three gait
measures (i.e., step length, stance phase, and double limb support) are
calculated by:
\% of Asymmetry=abs(Mparetic−Mnonparetic)12∗(Mparetic+Mnonparetic)∗100%
(1)
where M is the measure, and a value of 0
indicates symmetry. Step length is calculated as the anterior-posterior
distance between the heel centers of two successive feet specified based
by which leg is leading. Stance phase is calculated as the percent of
the gait cycle (i.e., between two successive heel strikes of the same
foot) between heel strike and toe off of the same foot. Double limb
support (DLS) phase is calculated as the percent of the gait cycle that
both feet are touching the ground specified by which leg is leading. The
asymmetry measures were determined during the five repetitions on the
ProtoKinetics Zeno Walkway System. Descriptive analyses were used to
identify the effects of gait training with the device on gait symmetry
and functional outcomes.
Results
The individual gait asymmetry measures are shown in Table 2.
All six participants improved step length symmetry. Four participants
improved DLS symmetry. Four participants improved stance phase symmetry
although the amount of change was relatively small.
Table 2 Changes in gait asymmetry measures after training
The individual functional measures are shown in Table 3.
All participants improved on all three functional outcomes (gait
velocity, TUG, and 6MWT). Four participants demonstrated larger than a
small meaningful change in gait velocity (≥ 6 cm/s) [35]. Two of the participants’ improvements were larger than the minimal detectable change (MDC) in TUG (≤− 3.5 sec) [36]. Altogether, five of the participants improved more than at least one of these MDC or small meaningful change limits.
Table 3 Changes in functional measures after training
Walking
on the rehabilitative shoe may benefit gait symmetry. All participants
improved step length symmetry after training, and the average change in
step length symmetry found in our study is similar to that shown in a
study focused on gait symmetry during split-belt treadmill (SBT)
training [37].
Four participants improved DLS symmetry; the two that did not improve
were the severely impaired participant (initial gait velocity of 9.0
cm/s) and the highly functional participant (initial gait velocity of
113.5 cm/s). Although these two did not respond with a DLS asymmetry
change, participant 3 improved step length asymmetry and had a
substantial decrease on the TUG, and participant 6 improved on the 6MWT
and had a substantial increase in gait velocity. For comparison, related
studies show no change in DLS symmetry following SBT training [37, 38].
Our results suggest that over-ground gait training using the
rehabilitative shoe could provide an additional benefit to the recovery
of DLS symmetry for some individuals after stroke.
The literature
does not provide estimates of the clinical relevance of gait asymmetry
measures while walking over ground, but does provide some spatiotemporal
measures for treadmill walking [39]. However, gait asymmetry has been associated with balance [40, 41]
and is considered a major cause of future degenerative issues with
hips, knees, and backs for stroke survivors with gait hemiparesis [42, 43].
Functional measures
Walking
on the rehabilitative shoe may help individuals with hemiparetic stroke
improve their functional walking. Two of the participants’ gait
velocity increased beyond a substantial meaningful change (≥ 14 cm/s),
two other participants’ gait velocity increased beyond a small
meaningful change (≥ 6 cm/s), and the remaining two improved less than
these ranges. These ranges are based on people 30 to 150 days post
stroke [35, 44].
One participant improved gait velocity beyond the clinically meaningful
change of ≥ 16 cm/s that another study reported for people less than 60
days post stroke [45].
All the participants in our study were more than one year post stroke,
which is much greater than the groups reported in these studies. Another
important measure is that two out of three participants who were
initially categorized as household ambulators (i.e., gait velocity of &l; 40 cm/s) became limited community ambulators (i.e., gait velocity
of 40–80 cm/s) after training [5]; these two participants were 5 and 10 years post stroke
All participants who were assessed improved on the TUG, and two of them improved beyond the MDC of − 3.5 sec [36].
Although all five participants assessed improved the distance walked in
the 6MWT following training, none of them surpassed the smallest
minimal clinically important difference (MCID) of 34 m reported by Fulk
and He [46].
The four-week training with only 6 hours total walk time may not be
long enough for each participant to show a meaningful change in aerobic
capacity. Continued daily use of the device for a longer time coupled
with concomitant exercise may help them further increase aerobic
capacity over time.
Subjective evaluations
At
the conclusion of the training and post-testing, we discussed the
device and therapy with each participant and family member (if present).
All the participants were generally positive about it. One participant
was very encouraged by the amount of improvement she had following the
training. Her thoughts are summarized by the two following statements:
“I walked into church last week without a cane for the first time [since
my stroke].” Her husband followed up by stating: “Her confidence
walking around the house has increased dramatically since she started
walking on the shoe.” Another participant stated: “I am able to walk
faster and my knee moves and my toes have started to move. And those are
a couple of things that didn’t happen before.” A video interview with
one of the participants is available [47].
Therapeutic mechanisms
The
device presented is unlike any known existing rehabilitation therapies
and is thought to function through a combination of mechanisms. These
mechanisms likely benefit each individual uniquely since stroke presents
in different ways. For example, all the participants showed a shorter
stance phase with the paretic side compared to the nonparetic side, but
three of the participants (1, 2, & 6) had a shorter step length with
the paretic side. Although these three participants showed a smaller
improvement in step length asymmetry, participant 1 showed the largest
double limb support asymmetry improvement and participants 2 and 6
showed the largest gait velocity improvements. Encouraging more use of
the paretic foot likely had a larger benefit to these participants.
These unique benefits suggest that our device may have a heterogenous
set of mechanisms that can benefit a wide set of stroke patients’
specific gait impairments. Further, all of our participants benefitted
from this treatment, which is different than some of the SBT studies
that show no gait symmetry improvements, especially step length
symmetry, in approximately 40% of participants [37, 38]. Below are details on some the mechanisms we believe cause our device to help correct gait. Asymmetric Motion:
Both the presented device and the SBT cause one foot to move backward
faster than the other. In SBT training, the gait asymmetry of the
patient is increased by having two treads move at different speeds so
that the patient must compensate to stay moving on the treadmill. When
the belts are returned to the same speed, the patient will retain the
“adjusted”, now more symmetric, gait on the treadmill [37, 48].
Our presented device moves the foot backward relative to the paretic
foot, much like the motion of the fast tread of a SBT. Both the SBT and
our device beneficially change step length symmetry, but only our device
shows improvements in double limb support symmetry. This additional
gait benefit is likely due the device attaching to the foot, which
allows training in an over-ground context. Context Awareness:
The corrected walking patterns from existing therapeutic methods, such
as treadmills, do not completely transfer to over-ground walking because
the dynamic and sensorimotor aspects of walking over ground are
distinctly different than walking on a treadmill [22, 28, 49, 50].
Research has indicated that only about 60% of the gait correction from
walking on a split-belt treadmill transfers to walking over ground in
individuals with stroke [51].
When
walking over ground, an individual has complete control over velocity,
whereas the treadmill speed limits one’s ability to change velocity.
Another important difference is the amount of visual flow: on a
treadmill, the scene is not moving, so there are no visual cues
reinforcing the forward motion that would be present when walking over
ground. Since walking is highly context dependent [25, 51–54],
these visual cues indicating a different context may prevent the
learned patterns on the treadmill from being expressed during
over-ground walking. Our device allows over-ground walking in the
environment of daily activities. A user of our device experiences a
congruent dynamic optical/visual flow as opposed to an individual on a
SBT, who typically views a static scene that is incongruent to training
movements. Cueing: The benefits of this device may also
arise from the multiple cues produced by the device that guide the user
through their gait. The first cue is that the nonparetic foot height is
decreasing after first contact in stance; a second cue is that the
nonparetic foot begins moving backward during the transition to stance.
These cues start before the paretic leg transitions from stance, which
provides a set of cues that possibly indicate the type of step to take
with the paretic leg. For example, the first cue may induce more weight
bearing on the paretic leg at mid-stance, while the second cue may
foster earlier toe off of the paretic leg at terminal stance. Encouraging Paretic Leg:
The device can also increase the relearning of the paretic leg by
reducing the effective output of the nonparetic leg by generating a
backward motion. The motion induced by the device encourages the wearer
to increase the use of their paretic leg. This effect is similar to the
idea of Constraint Induced Movement Therapy [15, 16].
By slightly destabilizing their nonparetic leg, the user will naturally
start to spend more time on their paretic side, which may help to
foster those abilities and confidence in using that side of their body. Home Rehabilitation:
The literature has continued to show that patients are dissatisfied
with their options for training after they are discharged from the
rehabilitation hospital/clinic [55–59]. Moreover, most individuals with stroke prefer a home-based approach for their initial rehabilitation [60].
The ability to train at home enables individuals to more frequently
rehabilitate themselves, which leads to better results in motor
relearning [61] and can maintain individuals’ ability to perform activities of daily living [62, 63].
Our device has the potential to be used in the home setting, which
could reduce the costs and increase the access as well as the amount of
rehabilitation.
There are open questions related to the frequency
of training, the length of each session, and how many weeks the training
should continue. The intensity of the training during each session can
also be customized by adjusting the spiral wheel to make the generated
backward motion longer and/or faster. This customization could also be
adjusted at regular intervals to keep a constant intensity level. Future
studies will evaluate how to optimize the therapy further.
Safety
is vital, particularly during home care. Using the device independently
in a safe way is being evaluated in a separate home-based trial. In the
study presented here, we found that participants became comfortable
with the device within the first three sessions and needed little or no
assistance after that. Out of the over 400 bouts of walking in our
study, the attending PT only provided physical assistance twice due a
perceived need for patient support. As such, we expect that home-based
therapy could be provided for many patients after they complete a few
sessions in the clinic and become qualified for home-use. The specific
requirements of being eligible for home-use are being evaluated and will
be discussed further once the larger home-based study is complete.
Limitations
A
limitation to this study is that only six participants were evaluated. A
study with a larger sample size will provide more details about how
these effects generalize across different stroke gait patterns. Another
limitation is that this study did not have a matched control group to
compare to standard physical therapy or simply walking for a similar
amount of time [64]. Despite these limitations, the initial results are promising and suggest that further study is warranted.
Conclusions
The
presented gait training device was tested on six individuals with
chronic stroke for twelve sessions over four weeks. During this time,
all participants improved on step length symmetry, four improved on
double limb support symmetry, and all improved on all three functional
outcome measures. Five of the six participants improved beyond the MDC
or meaningful change in at least one functional outcome. These results
demonstrate the feasibility of this device to improve a chronic,
hemiparetic stroke survivor’s gait symmetry and walking function. An
additional study of this device will further understand the impact on
the post stroke survivor’s quality of life, health range, future joint
and musculature degeneration, and morale.


No comments:
Post a Comment