And you really think predicting failure to recover is of ANY FUCKING USE AT ALL TO SURVIVORS? Do you have any usable brain cells at all? Weight change has absolutely no cause and effect for recovery. Will you please rub those two neurons you have together and get a spark of intelligence?
Weight Change during the Early Phase of Convalescent Rehabilitation after Stroke as a Predictor of Functional Recovery: A Retrospective Cohort Study;
by
1,* , 2, 3, 3, 3, 3, 3, 3 and 4
, 2, 3, 3, 3, 3, 3, 3 and 4
 , 2, 3, 3, 3, 3, 3, 3 and 4
, 2, 3, 3, 3, 3, 3, 3 and 4
1
Department of Physical Medicine and
Rehabilitation, Ibaraki Prefectural University of Health Sciences
Hospital, Ibaraki 300-0331, Japan
2
Department of Nutritional Management, Ibaraki Prefectural University of Health Sciences Hospital, Ibaraki 300-0331, Japan
3
Department of Physical Therapy, Ibaraki Prefectural University of Health Sciences Hospital, Ibaraki 300-0331, Japan
4
Department of Neurology, Ibaraki Prefectural University of Health Sciences Hospital, Ibaraki 300-0331, Japan
*
Author to whom correspondence should be addressed.
Academic Editor: Yoshihiro Yoshimura
Nutrients 2022, 14(2), 264; https://doi.org/10.3390/nu14020264
Received: 29 November 2021
/
Revised: 30 December 2021
/
Accepted: 5 January 2022
/
Published: 9 January 2022
(This article belongs to the Special Issue Recent Advances in Clinical Nutrition in Stroke Rehabilitation)
{kind=link}
It has been reported that weight gain at discharge compared with
admission is associated with improved activities of daily living in
convalescent rehabilitation (CR) patients with low body mass index.
Here, we investigated whether weight maintenance or gain during the
early phase of CR after stroke correlates with a better functional
recovery in patients with a wide range of BMI values. We conducted this
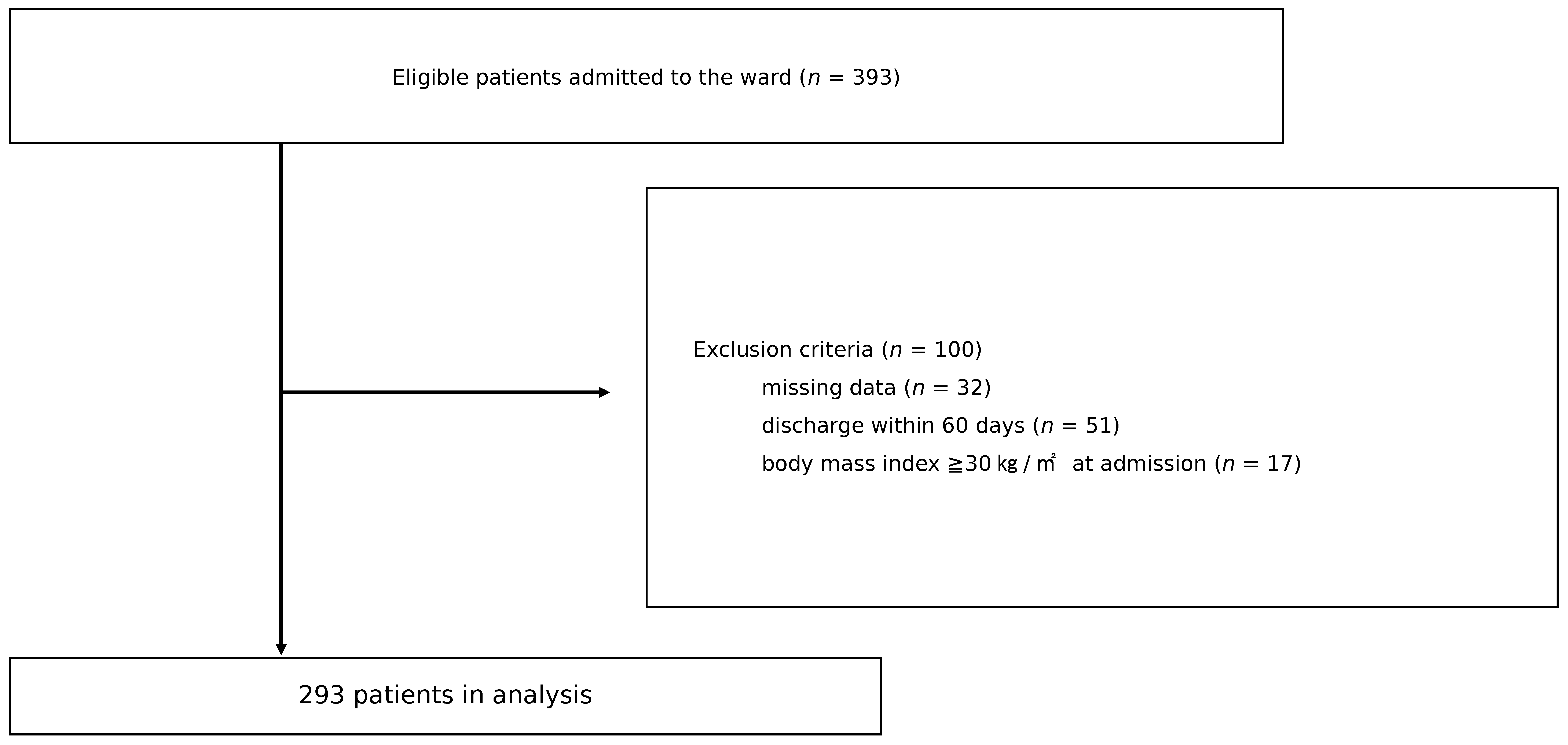
retrospective cohort study in a CR ward of our hospital and included
adult stroke patients admitted to the ward from January 2014 to December
2018. After ~1 month of hospitalization, the patients were classified
into weight loss and weight maintenance or gain (WMG) groups based on
the Global Leadership Initiative on Malnutrition criteria for weight. We
adopted the motor functional independence measure (FIM) gain as the
primary outcome. The motor FIM gain tended to be greater in the WMG
group but without statistical significance. However, multiple regression
analysis showed that WMG was significantly and positively associated
with motor FIM gain. In conclusion, weight maintenance or gain in
patients during the early phase of CR after stroke may be considered as a
predictor of their functional recovery, and nutritional management to
prevent weight loss immediately after the start of rehabilitation would
contribute to this.
Keywords:
convalescent rehabilitation; stroke; body weight; functional recovery; nutritional management
1. Introduction
The aging of the society is a global challenge today, and frailty [1] has become a critical issue. While there have been many molecular biological [2] and biochemical [3,4]
studies on frailty, various epidemiological studies have also been
conducted, and it is known that people with frailty have a higher risk
of developing strokes [5], as well as a higher risk of falls and hip fractures [6].
In Japan, the national health insurance system established a
convalescent rehabilitation (CR) ward in the year 2000, which has played
an important role in the post-acute care of patients with stroke, brain
or spinal cord injury, hip fracture, and hospital-associated
deconditioning [7].
It has been reported that the prevalence of malnutrition, malnutrition
risk status, and sarcopenia is high among patients admitted to the ward [8,9]. In addition, having malnutrition or sarcopenia has been associated with poor recovery of physical function in CR [9,10].
On the other hand, improvement of nutritional status among malnourished
elderly patients with stroke during CR has been linked to improved
activities of daily living (ADLs) [11,12].
Furthermore, we have previously reported that a group of patients whose
nutritional status was maintained at good or even slightly improved
from poor during CR had better functional recovery than a group of
patients whose nutritional status remained poor or worsened even if
their status was good at admission [13].
Among these studies, MNA -SF [14] in Ref. 11 GNRI [15] in Ref. 12, and CONUT [16]
in Ref. 13 have been used as diagnostic tools for malnutrition or
monitoring indicators of nutritional status, and recently, “GLIM(Global
Leadership Initiative on Malnutrition) criteria for the diagnosis of
malnutrition” [17]
has been proposed as a consensus report from several clinical nutrition
societies around the world. The GLIM criteria state that screening for
nutritional status should be conducted using validated tools such as the
MNA-SF [14], NRS-2002 [18], MUST [19], and SGA [20]
and that priority should be given to repeated weight measurements over
time to identify trajectories of weight loss, maintenance, and
improvement. The importance of recognizing the pace of weight loss in
the early stages of illness or injury has been emphasized in GLIM
criteria [17]. One study that focused on weight change in CR was conducted by Kokura et al. [21].
They reported that in CR patients with a low body mass index (BMI) at
admission, weight gain over the entire hospital stay up to the time of
discharge was associated with improved ADL [21].
As in the case of frailty, molecular biological analysis has been conducted on stroke patients [22], but many epidemiological studies have also been conducted [23,24,25]. The range of overweight not reaching obesity is also considered to be a risk factor for stroke [24], and it has been shown that there are not a few stroke rehabilitation patients with high BMI [25].
However, the relationship between weight change in CR and improvement
of ADL at the time of CR discharge in patients with a wide range of BMI
has not been clarified so far. In addition, we have not found any
studies that have assessed weight change in the early stages of CR and
examined its relationship with functional recovery.
This
study aims to address the clinical question of whether weight
maintenance gain or loss in the early stages of CR in patients with
stroke has a positive or negative impact, respectively, on functional
recovery at discharge.
More at link.
No comments:
Post a Comment