FYI.
Intensive Rehabilitation Program in Older Adults with Stroke: Therapy Content and Feasibility—Preliminary Results from the BRAIN-CONNECTS Study


1
Rehabilitation Research Group, Hospital del Mar Research Institute, Dr. Aiguader, 88, 08003 Barcelona, Catalonia, Spain
2
Physical Medicine and Rehabilitation
Department, Parc de Salut Mar (Hospital de l’Esperança), Sant Josep de
la Muntanya 12, 08024 Barcelona, Catalonia, Spain
3
Department of Medicine, Universitat
Autònoma de Barcelona, Passeig de la Vall d’Hebron, 119-129, 08035
Barcelona, Catalonia, Spain
4
Geriatrics Department, Brugmann
University Hospital, Université Libre de Bruxelles, Place A. Van
Gehuchten 4, 1020 Brussels, Belgium
5
WHO Collaborating Centre for Public
Health Aspects of Musculo-Skeletal Health and Ageing, Division of Public
Health, Epidemiology and Health Economics, University of Liège, 4000
Liège, Belgium
6
Faculty of Health and Life Sciences, Universitat Pompeu Fabra, Aiguader 80, 08003 Barcelona, Catalonia, Spain
7
Department of Radiology, Biomedical
Research Institute Imaging Research Unit, Diagnostic Imaging Institute,
Doctor Josep Trueta University Hospital of Girona, Avinguda de França,
s/n, 17007 Girona, Catalonia, Spain
*
Author to whom correspondence should be addressed.
Int. J. Environ. Res. Public Health 2023, 20(6), 4696; https://doi.org/10.3390/ijerph20064696
Received: 22 January 2023
/
Revised: 23 February 2023
/
Accepted: 28 February 2023
/
Published: 7 March 2023
(This article belongs to the Special Issue Promoting Geriatric Care: Comprehensive Geriatric Assessment, Frailty and Resilience)
{kind=link}
Abstract
The main objective was to assess the feasibility of
an intensive rehabilitation program (IRP) for stroke patients; and
secondly, to detect eventual age-related differences in content,
duration, tolerability, and safety in a prospective observational cohort
of patients diagnosed with subacute stroke, admitted to inpatient
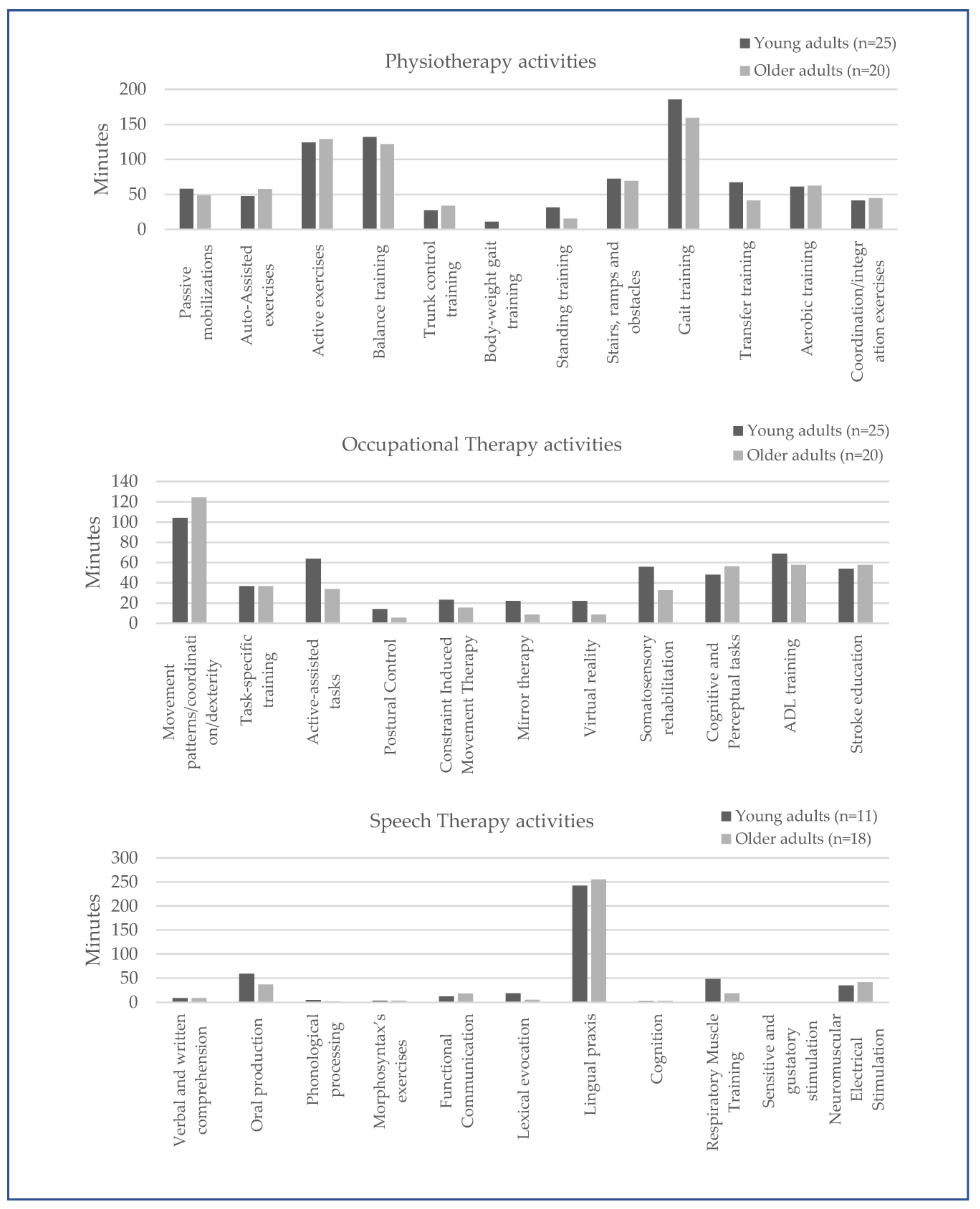
rehabilitation (BRAIN-CONNECTS project). Activities during physical,
occupational and speech therapy, and time dedicated to each one were
recorded. Forty-five subjects (63.0 years, 77.8% men) were included. The
mean time of therapy was 173.8 (SD 31.5) minutes per day. The only
age-related differences when comparing patients ≥65 and <65 years
were a shorter time allocated for occupational therapy (−7.5 min (95% CI
−12.5 to −2.6), p = 0.004) and a
greater need of speech therapy (90% vs. 44%) in the older adults. Gait
training, movement patterns of upper limbs, and lingual praxis were the
most commonly performed activities. Regarding tolerability and safety,
there were no losses to follow-up, and the attendance ratio was above
95%. No adverse events occurred during any session in all patients.
Conclusion: IRP is a feasible intervention in patients with subacute
stroke, regardless of age, and there are no relevant differences on
content or duration of therapy.
1. Introduction
There
are more than 101 million stroke survivors in the world, and every
year, more than 12.2 million individuals suffer a new stroke [1].
As the population increases and lives longer, the incidence of stroke,
long-term sequelae, and associated costs are expected to grow
dramatically; about one of every four people over the age of 25 will
have a stroke in their lifetime [1].
Many survivors experience motor, sensory, perceptual, and cognitive
impairments, and require rehabilitation in the months following the
stroke [2].
The
intensive rehabilitation programs (IRP) offer multidisciplinary care
for patients with subacute stroke, and lead to better functional results
and less institutionalization. The individual’s cognitive status,
comorbidity, and previous functional level are determining factors for
admitting patients to IRP [3].
Advanced age is considered a risk of receiving poorer quality of care
and a limitation for rehabilitation outcomes following stroke [4].
The influence of age on stroke rehabilitation has been a controversial
issue, with studies showing a negative effect on outcomes, whereas
others have not found any relationship. Although older patients present
more dependence in activities of daily living (ADL) three months after
stroke, no significant differences in the efficacy of the rehabilitation
have been found in older stroke survivors [5].
Some quality care indicators such as the number of computerized
tomography head scans and carotid image analyses in older patients with
stroke seem to be lower than in younger adults [4],
but there is presently no evidence showing that content and/or
intensity of rehabilitation therapies are different in the oldest
patients with stroke [6].
Current
guidelines recommend that rehabilitation programs should provide at
least 3 h per day of physiotherapy, occupational therapy, and speech
therapy, 5 days a week [7,8].
Although age in itself is not considered as a selection criterion for
IRP, in daily practice, older patients, who might have higher medical
and social needs, are often referred to nursing homes and intermediate
care settings where rehabilitation programs are of lower intensity.
The
medical literature on stroke IRP does not usually report the intensity
and content of interventions. Factors such as patient tolerance, the
resources of each facility, and the physical environment can modify the
intensity of the given therapies [3,7,9,10,11,12].
The measurement of the interventions included in the rehabilitation
programs represents a challenge for professionals, and it is essential
to advance in the demonstration of their benefits. In daily practice,
the rehabilitation process starts with a clinical and functional
assessment of patients, followed by the establishment of objectives
according to individual needs and a therapeutic plan to achieve them.
However, the exact content and description of the interventions are
usually unknown. The complex variety of treatment goals and therapies
have been called the “black box” of rehabilitation [10,11,12]. There is a need for an adequate system to classify the wide range of interventions [13].
Moreover, the standardization of the therapies will provide the
external validity necessary for clinical trials. Several objective
systems to measure the activities and the time dedicated to each of them
have been proposed [12,14,15], but only one study gives detailed information about physical, occupational, and speech therapies [3]. Feasibility studies are important, especially in the development of complex interventions and multidisciplinary programs [10].
Before testing the efficacy of an intervention through a clinical
trial, it is recommended to verify that it can be carried out as
proposed in clinical settings [16].
Based
on these considerations, this study aimed at assessing the feasibility
of an IRP for stroke patients by recording the type of activities and
quantifying the time dedicated to each one during physiotherapy,
occupational, and speech therapy; and secondly, to assess eventual
differences according to age.
More at link.
No comments:
Post a Comment