FYI.
The Implications of Microglial Regulation in Neuroplasticity-Dependent Stroke Recovery

Department of Rehabilitation, Beijing Rehabilitation Hospital, Capital Medical University, Beijing 100144, China
*
Authors to whom correspondence should be addressed.
Biomolecules 2023, 13(3), 571; https://doi.org/10.3390/biom13030571
Received: 17 January 2023
/
Revised: 23 February 2023
/
Accepted: 14 March 2023
/
Published: 21 March 2023
(This article belongs to the Special Issue Protection, Plasticity, and Physical Rehabilitation in Ischemic Injury (Volume II))
Abstract
Stroke causes varying degrees of neurological deficits, leading to corresponding dysfunctions. There are different therapeutic principles for each stage of pathological development. Neuroprotection is the main treatment in the acute phase,(Except that it doesn't exist and should be called the neuronal cascade of death signifying extreme urgency while neuroprotection means nothing to survivors and doctor use that to bamboozle patients; 'We didn't get neuroprotection to work'. As compared to the statement; 'We failed at stopping the neuronal cascade of death thus allowing millions to billions of your neurons to die'
WHICH STATEMENT WILL GET YOUR DOCTORS TO SOLVE STROKE? )
and functional
recovery becomes primary in the subacute and chronic phases.
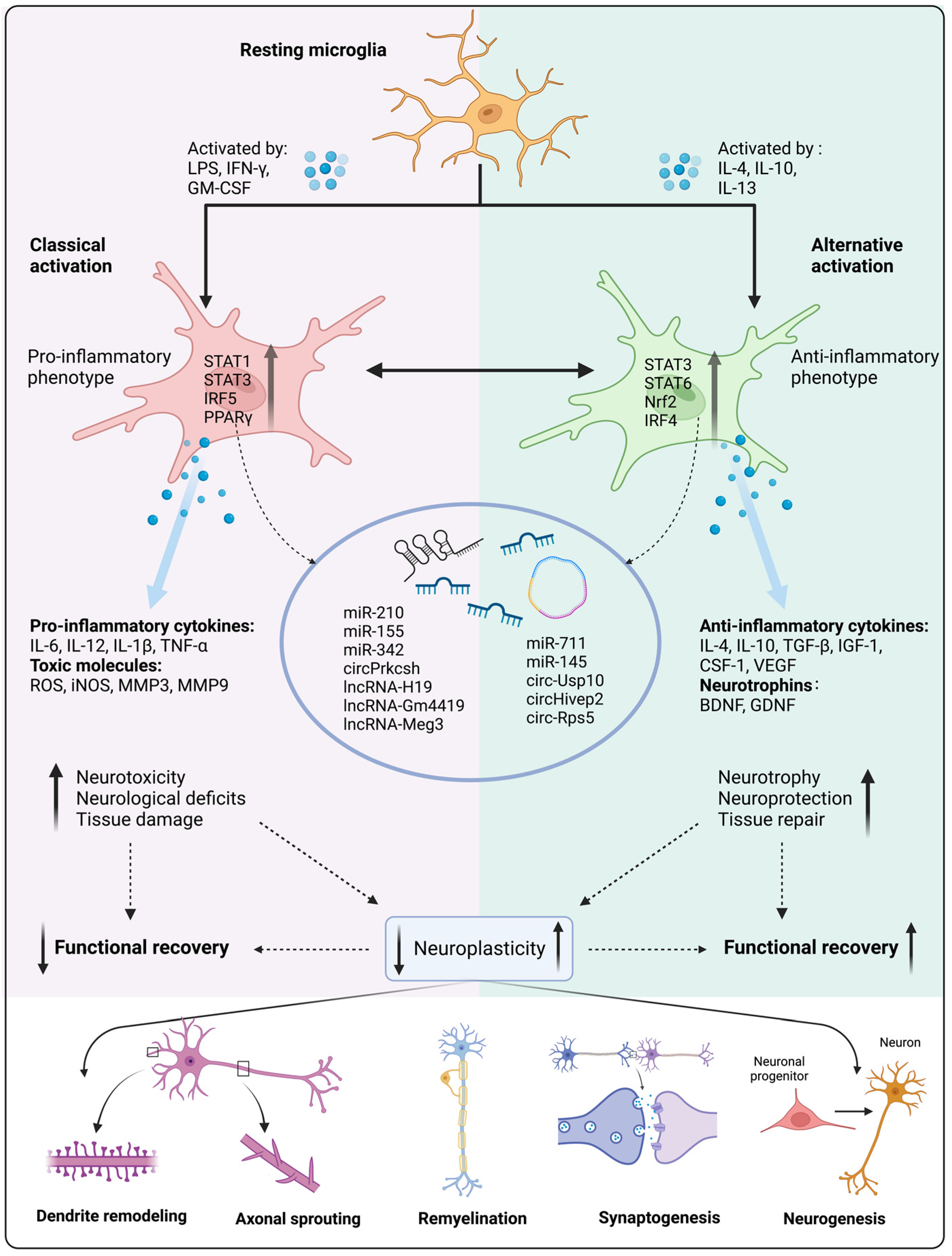
Neuroplasticity is considered the basis of functional restoration(But your doctor knows nothing on how to make it repeatable on demand.) and
neurological rehabilitation after stroke, including the remodeling of
dendrites and dendritic spines, axonal sprouting, myelin regeneration,
synapse shaping, and neurogenesis. Spatiotemporal development affects
the spontaneous rewiring of neural circuits and brain networks.
Microglia are resident immune cells in the brain that contribute to
homeostasis under physiological conditions. Microglia are activated
immediately after stroke, and phenotypic polarization changes and
phagocytic function are crucial for regulating focal and global brain
inflammation and neurological recovery. We have previously shown that
the development of neuroplasticity is spatiotemporally consistent with
microglial activation, suggesting that microglia may have a profound
impact on neuroplasticity after stroke and may be a key therapeutic
target for post-stroke rehabilitation. In this review, we explore the
impact of neuroplasticity on post-stroke restoration as well as the
functions and mechanisms of microglial activation, polarization, and
phagocytosis. This is followed by a summary of microglia-targeted
rehabilitative interventions that influence neuroplasticity and promote
stroke recovery.1. Introduction
Stroke
is a major cause of death and long-term disability, worldwide. Despite
constant incidence and declining mortality rates over the past 20 years,
the number of stroke survivors continues to decrease [1,2,3]. They are unable to live independently and are more likely to experience subsequent neurological sequelae [4,5].
Stroke can cause focal and global neurological deficits. Different
therapeutic principles are adopted in different periods. In the acute
stage of stroke, neuroprotection is the main treatment [6];
reducing cerebral ischemia-reperfusion injury (IRI) is also crucial. In
the subacute and chronic stages, functional recovery becomes the
primary objective. Neuroplasticity is recognized as the basis of
functional restoration and neurological rehabilitation after stroke,
including remodeling of dendrites and dendritic spines, axonal
sprouting, synapse shaping, and neurogenesis. Spontaneous
neuroplasticity begins immediately after stroke, reaches a plateau in
three to four weeks, and can be sustained in the chronic phase [7]. Spatiotemporal development profoundly affects the reconstruction of neural circuits and brain networks.
Microglia,
the resident immune cells of the central nervous system (CNS), play a
key role in brain development, homeostasis maintenance, and the disease
response of the CNS through phenotypic polarization, morphological
changes, and functional transformation. They participate in a variety of
pathophysiological processes in the brain, including the promotion of
neuronal survival, induction of programmed cell death, immune monitoring
and antigen presentation, inflammation regulation, modulation of
synaptic activity, synaptic pruning, remodeling, etc. [8,9,10,11,12].
After
stroke, the activation, polarization, and phagocytosis of microglia are
crucial for regulating the neuroinflammatory microenvironment and
enhancing neuroplasticity. Our previous study presented that the
development of neuroplasticity overlaps both temporally and spatially
with microglial activation [7],
suggesting that microglia may have a profound impact on neuroplasticity
following stroke and that they may be key therapeutic targets for
stroke rehabilitation. In this review, we explore therapeutic targeting
at different stages after stroke and the impact of neuroplasticity
during this process. We then discuss the functions and mechanisms of
microglial activation, polarization, and phagocytosis under
physiological and pathological conditions. Finally, we provide a summary
of microglia-targeted therapeutic interventions for promoting stroke
recovery.
2. Pathophysiology and Therapeutic Target of Stroke Recovery
2.1. Pathophysiology of Stroke in Different Phases
Stroke
commonly comprises two pathological subtypes. Hemorrhagic stroke
accounts for approximately 10–15% of stroke cases. During this process,
stress in the brain and internal injury cause the rupture of blood
vessel [13].
Hematomas compressing brain tissue form for blood leakage into the
brain parenchyma. The mass effect of the hematoma combined with
neurotoxic effects further causes increased intracranial pressure,
cerebral herniation, or death [14,15].
Ischemic
stroke is caused by abrupt occlusion of the cerebral artery. The
consequent interruption of blood flow and obstruction of the supply of
oxygen lead to glutamate excitotoxicity, calcium overload, oxidative and
nitrosative stress, and the release of inflammatory mediators, thereby
activating a series of detrimental signaling cascades that induce
neuronal injury or death [1,2,16,17].
Reversible neuronal impairment occurs after an ischemic attack, leading
not only to relevant symptoms but also functional deficits
corresponding to the location of the ischemia [18].
The progression of brain damage involves irreversibly injured necrotic
tissue in the ischemic core, followed by injury development in the
penumbral area, and then expanding to the entire ischemic territory [1,19].
Due to focal and global brain neurological damage following stroke,
patients have different degrees of neurological deficits after stroke,
such as dyskinesia, sensory dysfunction, swallowing dysfunction,
dysarthria, aphasia, cognitive impairment, impaired cardiopulmonary
function, mental disorders, and many complications, which further leads
to a decline in quality of life and social participation [3,20].
Aside
from revascularization therapy(thrombolysis and thrombectomy) and
neuroprotective therapies (non-pharmaceutical and pharmaceutical
therapies) for managing stroke in different phases [21],
rehabilitative therapy helps to alleviate disability by promoting the
recovery of impairment, activity, or participation after stroke [22]
and is formally associated with a “time frame”, which coincides with
the development of stroke and the period of maximal spontaneous recovery
[23]. Thus, although rehabilitation plays a key role after stroke, not all stages are suitable for rehabilitative interventions [24]. According to both animal models and human trials, intensive rehabilitation within 24 h is potentially harmful [23].
In a clinical trial, a four-week intervention of physical fitness
training did not result in an improvement in activities during the
subacute period (days 5–45 after stroke) [25].
The therapeutic targets of stroke recovery vary according to the developmental pathophysiological process (Table 1).
In the acute phase (minutes to days), a series of detrimental events
occur after acute ischemic injury, including infiltration of peripheral
immune cells, activation of resident glial cells, disturbance of ionic
homeostasis, oxidative stress, mitochondrial dysfunction, and DNA
damage. These processes involve cell necrosis within the lesion core and
peri-infarct area. Therapeutic strategies have focused on
neuroprotection to prevent neuronal injury and death, reduce infarct
volume, and limit the decrease in neuronal density in the penumbra [16,26,27,28,29,30,31].
In addition, reducing IRI is critical. During the restoration of blood
perfusion, IRI can lead to cerebral edema and even hemorrhage, thereby
exacerbating the detrimental biological cascade response and causing
irreversible tissue damage [21,32].
Therefore, besides neuroprotection, effective reduction of IRI is also a
key target in the treatment of the acute phase of ischemic stroke [33].
Table 1.
Pathophysiology and therapeutic targets of ischemic stroke in the acute,
subacute, and chronic phases. BBB, blood-brain barrier; ROS, reactive
oxygen species.

{kind=link}
{kind=link}
{kind=link}
In the subacute phase (days to weeks), the
mechanisms are more complicated than in the acute phase and include
amplification of local and systemic immune responses, increased cytokine
and reactive oxygen species (ROS) production, cell edema, and ion
imbalances [28,34].
The activation of several protective mechanisms triggers beneficial
repair processes, including neurogenesis and angiogenesis [27].
In addition, many endogenous processes are active, including axonal
sprouting, dendrite remodeling, increased levels of growth factors, and
altered synaptic and cortical excitability. Some of these processes have
been demonstrated to mediate behavioral changes [35].
In
the chronic phase (weeks to months), the end of spontaneous structural
recovery is marked by stabilization of the post-stroke neurological
deficits [35].
The therapeutic priorities should shift from neuroprotection to
functional rehabilitation. Post-ischemic inflammatory responses appear
to exacerbate tissue damage at an early stage, whereas they are assumed
to promote tissue repair and functional restoration during the chronic
phase [36].
During this stage, excitotoxicity decreases and the brain milieu
becomes primarily inhibitory, and neural repair and excitability
enhancement come to the forefront of post-stroke intervention [22,35].
More at link.
No comments:
Post a Comment