Ask your doctor to test you.
How can you tell if you are low on selenium?
What are the symptoms?
infertility in men and women.
muscle weakness.
fatigue.
mental fog.
hair loss.
weakened immune system.
The latest here:
Selenium, Stroke, and Infection: A Threefold Relationship; Where Do We Stand and Where Do We Go?


1
Department of Neurology, Nicosia New General Hospital, Nicosia 2029, Cyprus
2
Second Department of Neurology, School of
Medicine, ‘Attikon’ University Hospital, National and Kapodistrian
University of Athens, 124 62 Athens, Greece
3
Medical School, University of Cyprus, Nicosia 2024, Cyprus
*
Author to whom correspondence should be addressed.
Nutrients 2023, 15(6), 1405; https://doi.org/10.3390/nu15061405
Received: 14 December 2022
/
Revised: 8 March 2023
/
Accepted: 9 March 2023
/
Published: 15 March 2023
(This article belongs to the Special Issue The Role of Nutrition in Neurological Disorders)
{kind=link}
Abstract
Stroke is currently the second most common cause of
death worldwide and a major cause of serious long-term morbidity.
Selenium is a trace element with pleotropic effects on human health.
Selenium deficiency has been associated with a prothrombotic state and
poor immune response, particularly during infection. Our aim was to
synthesize current evidence on the tripartite interrelationship between
selenium levels, stroke, and infection. Although evidence is
contradictory, most studies support the association between lower serum
selenium levels and stroke risk and outcomes. Conversely, limited
evidence on the role of selenium supplementation in stroke indicates a
potentially beneficial effect of selenium. Notably, the relationship
between stroke risk and selenium levels is bimodal rather than linear,
with higher levels of serum selenium linked to disturbances of glucose
metabolism and high blood pressure, morbidities which are, in turn,
substrates for stroke. Another such substrate is an infection, albeit
forming a bidirectional relationship with both stroke and the
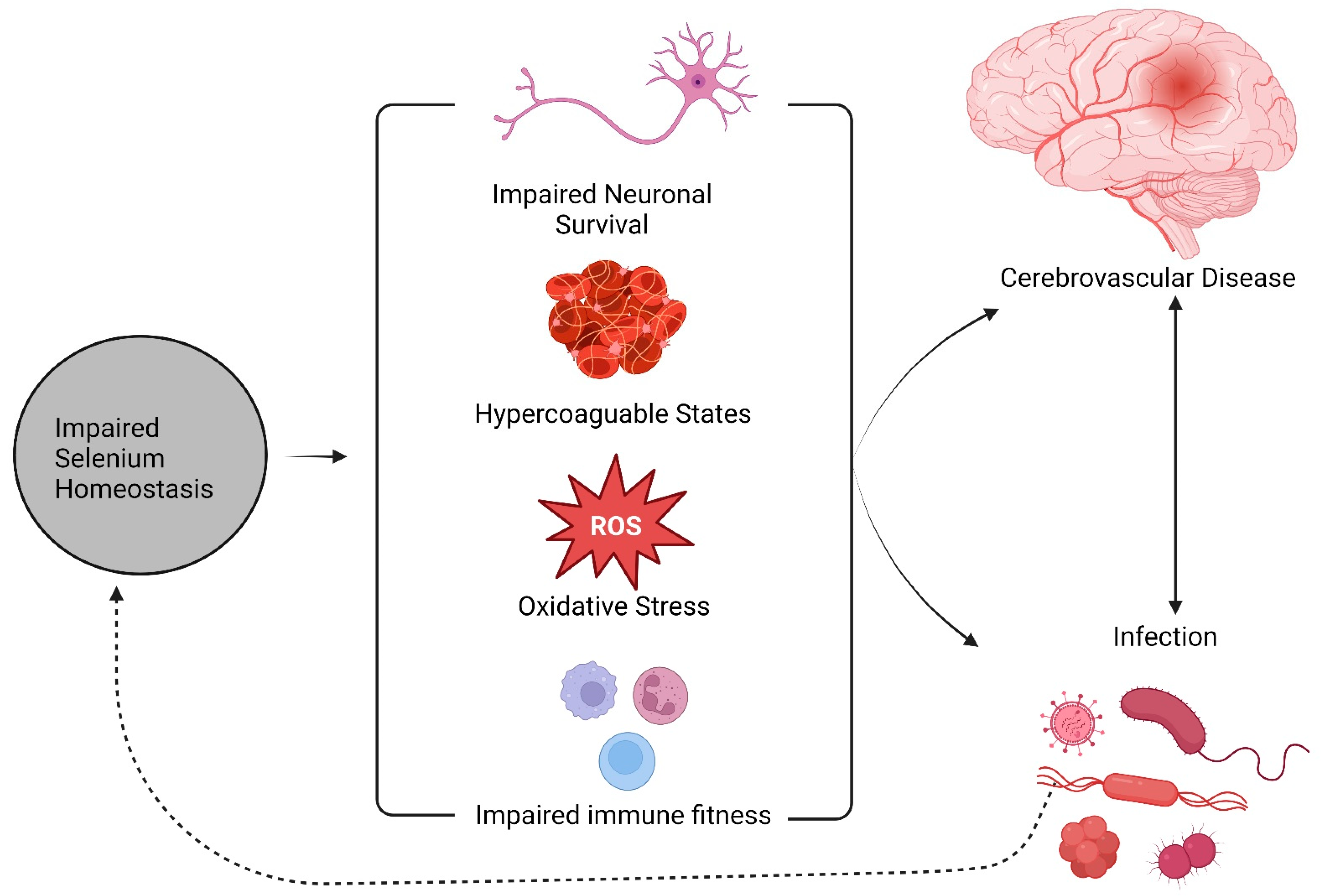
consequences of impaired selenium metabolism. Perturbed selenium
homeostasis leads to impaired immune fitness and antioxidant capacity,
which both favor infection and inflammation; specific pathogens may also
contend with the host for transcriptional control of the
selenoproteome, adding a feed-forward loop to this described process.
Broader consequences of infection such as endothelial dysfunction,
hypercoagulation, and emergent cardiac dysfunction both provide stroke
substrates and further feed-forward feedback to the consequences of
deficient selenium metabolism. In this review, we provide a synthesis
and interpretation of these outlined complex interrelationships that
link selenium, stroke, and infection and attempt to decipher their
potential impact on human health and disease. Selenium and the unique
properties of its proteome could provide both biomarkers and treatment
options in patients with stroke, infection, or both.
1. Background
Stroke
is the second most common cause of death worldwide (11.8% of all
deaths) and a major cause of serious long-term morbidity [1,2]. Ischemic stroke (IS) is the most common type of stroke, comprising about 80% of the total cerebrovascular events [3].
Despite the decline of stroke mortality over the years, the number of
IS-related deaths and morbidities and overall disability-adjusted life
years (DALY) lost remains of great importance and increases in the
course of time [4]. Although most risk factors are modifiable, including hypertension, diabetes mellitus, hyperlipidemia, and smoking [5] other non-modifiable variables such as age, sex, and genetics have also been considered as risk factors for stroke [6,7,8].
Studies on nutritional factors affecting stroke risk and outcomes have
been generally focused on dyslipidemia, with micronutrients and trace
elements being generally underexplored in the literature.
Micronutrients
or trace elements refer to nutritional factors required in specific,
minute quantities by organisms and affect specific aspects of their
physiological functions. One such micronutrient is selenium (Se) [9].
Selenium exerts multiple pleiotropic homeostatic roles on human health,
several of which are interwoven with stroke etiopathogenesis and its
outcomes, as well as infection. This tripartite relationship is not
merely observational; many of the shared pathophysiological substrates
that link infection and stroke find common grounds in Se biology.
A
central case in point for this concept arises from the observed
interrelationships between serum Se concentration, the systemic
inflammatory response, and multi-organ failure in sepsis patients. As
selenoproteins are known to mitigate oxidative stress, coagulation, and
immune fitness, these associations potentially reflect homeostatic
adaptations aimed at preserving tissues and organs affected by the
stress represented by sepsis [10].
Another example of the pertinence of Se biology arises from host–virus
interactions, where host Se biology is actively contested by viruses in
order to favor egress, with oxidative stress and hypercoagulable states
representing secondary consequences. Moreover, selenium depletion
secondary to infection may build up towards a prothrombotic state and
impaired immune fitness, a milieu that has been shown to favor viral
genomic instability potentially resulting in variants with greater
pathogenicity [11].
The
purpose of this critical review is to explore state-of-the-art evidence
on the epidemiology, potential mechanisms, and possible interventions
regarding selenium status, infection, and stroke. Furthermore, we aim to
provide a concise report on current concepts regarding selenium
supplementation in the specific setting of infectious disease and
stroke, as well as their interplay.
More at link.
No comments:
Post a Comment