https://www.frontiersin.org/articles/10.3389/fneur.2018.00283/full?
 Eugene Lin
Eugene Lin Victoria Calderon
Victoria Calderon Julie Goins-Whitmore
Julie Goins-Whitmore Vibhav Bansal2 and
Vibhav Bansal2 and  Osama Zaidat
Osama Zaidat- 1Neuroscience Institute, Mercy Health-St. Vincent Medical Center, Toledo, OH, United States
- 2Neuroscience Institute, Mercy Health-St. Rita’s Medical Center, Lima, OH, United States
Background and purpose: As the fourth mobile stroke unit (MSU) in the nation, and the first 24/7 unit worldwide, we review our initial experience with the Mercy Health MSU and institutional protocols implemented to facilitate rapid treatment of acute stroke patients and field triage for patients suffering other time-sensitive, acute neurologic emergencies in Lucas County, Ohio, and the greater Toledo metropolitan area.
Methods: Data was prospectively collected for all patients transported and treated by the MSU during the first 6 months of service. Data was abstracted from documentation of on-scene emergency medical services (EMS) personnel, critical care nurses, and onboard physicians, who participated through telemedicine.
Results: The MSU was dispatched 248 times and transported 105 patients after on-scene examination with imaging. Intravenous (IV) tissue plasminogen activator (tPA) was administered to 10 patients; 8 patients underwent successful endovascular therapy after a large vessel occlusion was identified using CT performed within the MSU without post treatment symptomatic hemorrhage. Moreover, 14 patients were treated with IV anti-epileptics for status epilepticus, and 19 patients received IV anti-hypertensive agents for malignant hypertension. MSU alarm to on-scene times and treatment times were 34.7 min (25–49) and 50.6 min (44.4–56.8), respectively.
Conclusion: The world’s first 24/7 MSU has been successfully implemented with IV-tPA administration rates and times comparable to other MSUs nation-wide(wrong endpoint), while demonstrating rapid triage and treatment in the field for neurologic emergencies, including status epilepticus. With the rising number of MSUs worldwide, further data will drive standardized protocols that can be adopted nationwide by EMS.
Introduction
Stroke has fallen from the third to the fifth leading cause of death over the past decade because of advances in prevention and treatment (1). Organizations including the American Heart Association and American Stroke Association have increased community awareness of stroke symptoms by popularizing the “FAST” and “BE-FAST” acronym. Moreover, hospitals have made stroke-care a priority by implementing policies that have significantly improved (reduced) door-to-needle times (2). There is still room for improvement, as IV-tPA can only be administered after imaging excludes a hemorrhagic stroke. The process of transporting acute stroke patients to the hospital to obtain this imaging often delays therapy by more than an hour—the equivalence of 120 million neurons dying (3).
The introduction of a mobile stroke unit (MSU), a specialized neuro-critical care ambulance with a portable CT scanner and telemedicine capabilities, circumvents this delay. They provide physicians the information and resources necessary to safely screen patients for IV-tPA eligibility and initiate thrombolytics in the field, significantly improving symptom onset to treatment times. During 2016, six MSUs were operational in U.S. metropolitan cities: Houston, Cleveland, Denver, Toledo, Memphis, and New York City, in order of launch. However, the number of MSUs continues to increase every year in the U.S. and abroad. Toledo continues to operate the only unit worldwide that is operational 24/7.
Using data from the BEnefits of Stroke Treatment Delivered Using a Mobile Stroke Unit (BEST-MSU) study, which details Houston’s implementation of its MSU, and Cleveland Clinic’s published experience from its MSU, Mercy Health introduced the world’s first 24/7 MSU in Toledo, OH, USA. In this study, we review and summarize the steps needed to establish, implement, and maintain an operational 24/7 MSU. We also present data that demonstrates the timesaving benefits our MSU has provided the community, in treating acute stroke and other neurological emergencies. We included comparisons of our patient demographics and treatment metrics to data from other MSUs. Several areas of improvements to further enhance our response and treatment times are also identified and discussed.
Materials and Methods
Data was prospectively collected for all patients transported and treated by the MSU during the first 6 months of its operation. Patient and treatment information was documented by the Mercy Health MSU team on a standardized MSU run sheet in EPIC (Verona, WI, USA). Data was abstracted and correlated retrospectively from the run sheet and patient records. Descriptive statistical analysis was then used to organize the data (Microsoft).
Emergency Medical Services (EMS) and Fire Department Training
Our Mercy Health MSU is located in northwest Ohio in Lucas County, which encompasses 596 square miles and has an estimated population of 433,689 (2015 U.S. Census). In addition, a bordering county to the west of the operating base is Fulton County, which covers 407 square miles and has a population of 42,537 (2015 U.S. Census).
Working with the Lucas County Emergency Medical Services (LCEMS) leadership, we elected to base our MSU near the northwest area of Lucas County. This area had the highest density of stroke diagnoses from Medicare diagnostic codes based on discharge diagnosis and patient zip codes. However, due to our MSU’s moving target radius, training was initiated with all 464 Lucas County EMS paramedic personnel, inclusive of the multiple fire departments within Lucas County. These EMS personnel had already received initial stroke training, including a 2-h interactive training with video demonstration and hands-on Rapid Arterial oCclusion Evaluation (RACE) scale assessment (2) using mock patients as a part of the RACE protocol implementation in July 2015. With adjunct training, prior to the launch of the MSU, we introduced them to the vehicle, updated scene interaction and goals, and reinforced potential stroke identification with the Cincinnati Prehospital Stroke and RACE scale. In addition, there has been ongoing training with individual squads and Toledo Fire stations since the initiation of the MSU to provide ongoing workflow improvements and feedback.
Protocol
Our MSU is alerted as a part of the LCEMS dispatch if a patient is identified as having a suspected stroke on the initial call, or upon arrival by a first responder in a 15-min radius from the MSU location (Figure 1A). The MSU and the vascular neurologist (VN) on call are notified concurrently when a run is initiated. Then every patient with possible stroke symptoms is evaluated on-scene with a focused neurological examination by our EMS personnel and critical care nurse, who are both dually trained in the NIH Stroke Scale and Emergency Neurological Life Support. If a patient is deemed to have a stroke, or was determined as a RACE candidate by the initial EMS team, a head CT is acquired (Figure 1B). During the evaluation with the MSU team, the InTouch Health Express Device is available with a VN to actively participate in performing the examination and obtain further history from the EMS team, patient, and the patient’s family.
FIGURE 1
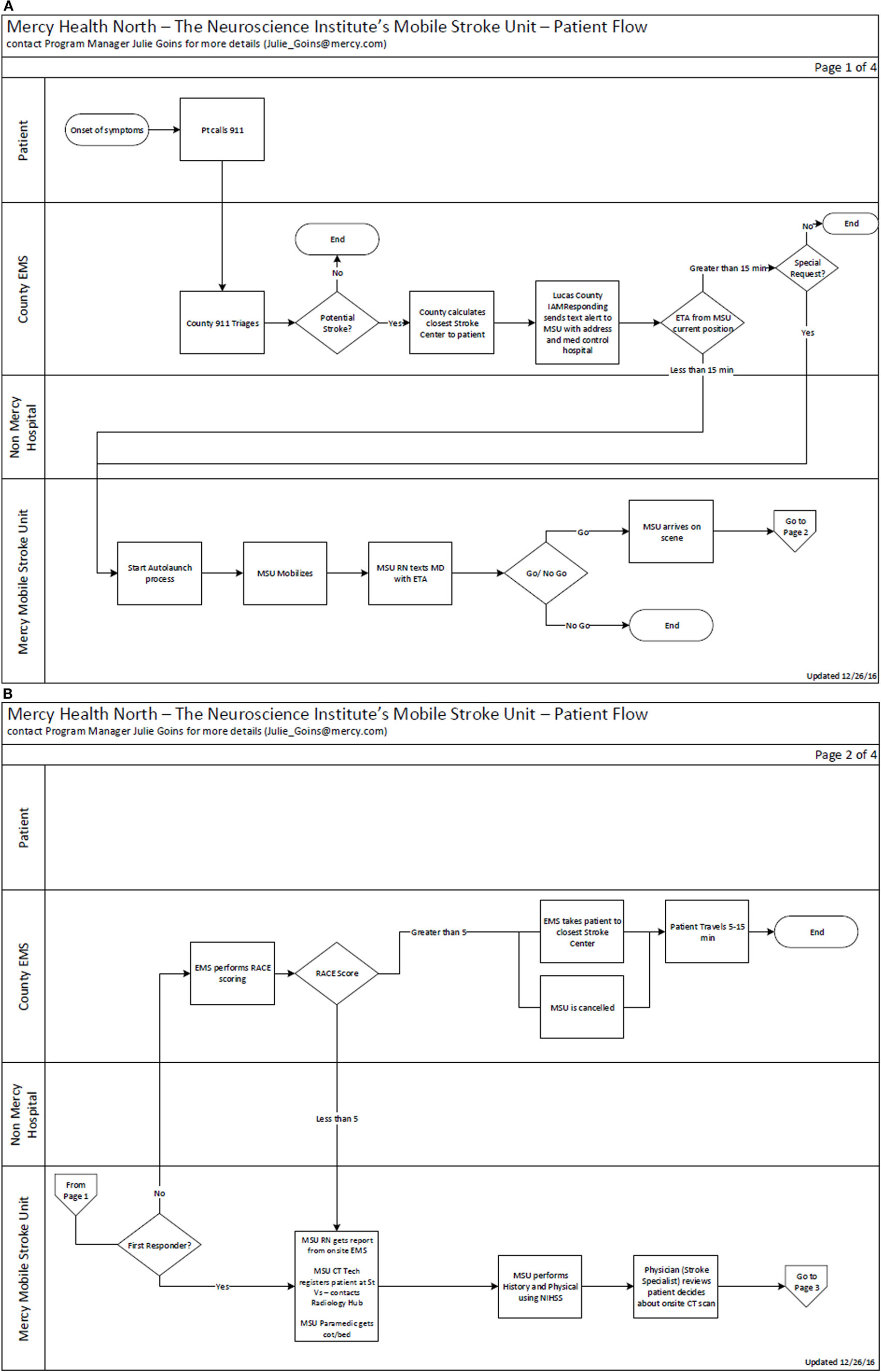
Figure 1. (A) Mercy Health Mobile Stroke Unit (MSU) workflow and triage algorithm from activation. (B) Mercy Health MSU activation and triage algorithm part 2.
After the on-scene neurological assessment is completed and the patient is transported to the MSU, the scan is completed and uploaded both to the cloud for access by mobile device and to our PACS system for evaluation by our neuroradiologist within 5 min. Based on the results, history, and examination, the proper course of treatment is initiated, and the patient is subsequently transported to the nearest appropriate hospital (4–6).
Results
During the initial 6 months, our MSU transported a total of 105 patients. Another 143 dispatches were cancelled enroute to the scene after first responders evaluated the patient. The average age of our patient was 70.8 with a median of 73. When compared with initial published MSU papers from Bowry et al., Wendt et al., and Walter et al., we treated patients within a similar age range (Table 1) (3–5). In addition, we treated almost equal numbers of men and women in our first 6 months. Reviewing the risk factors for these same patients, the proportion evaluated with HTN (60%), DM (25.7%), and prior strokes (32.4%) were comparable to Charité-Universitätsmedizin MSU and University of the Saarland MSU (4, 5). Patients with a history of atrial fibrillation (18.1%) were similar to the BEST-MSU results (3).
No comments:
Post a Comment