No mention of stroke and CPSP(Central post-stroke pain) so ask your doctor to followup and see if this would work for stroke.
What Is the Role of the Placebo Effect for Pain Relief in Neurorehabilitation? Clinical Implications From the Italian Consensus Conference on Pain in Neurorehabilitation
 Gianluca Castelnuovo1,2*,
Gianluca Castelnuovo1,2*,  Emanuele Maria Giusti1,2,
Emanuele Maria Giusti1,2,  Gian Mauro Manzoni1,3,
Gian Mauro Manzoni1,3,  Donatella Saviola4,
Donatella Saviola4,  Samantha Gabrielli5,
Samantha Gabrielli5,  Marco Lacerenza5,
Marco Lacerenza5,  Giada Pietrabissa1,2,
Giada Pietrabissa1,2,  Roberto Cattivelli1,2,
Roberto Cattivelli1,2,  Chiara Anna Maria Spatola1,2,
Chiara Anna Maria Spatola1,2,  Alessandro Rossi1,
Alessandro Rossi1,  Giorgia Varallo1,
Giorgia Varallo1,  Margherita Novelli1,
Margherita Novelli1,  Valentina Villa1, Francesca Luzzati6, Andrea Cottini6,
Valentina Villa1, Francesca Luzzati6, Andrea Cottini6,  Carlo Lai7,
Carlo Lai7,  Eleonora Volpato2,8,
Eleonora Volpato2,8,  Cesare Cavalera2,
Cesare Cavalera2,  Francesco Pagnini2,9,
Francesco Pagnini2,9,  Valentina Tesio10,
Valentina Tesio10,  Lorys Castelli10, Mario Tavola11,
Lorys Castelli10, Mario Tavola11,  Riccardo Torta12,
Riccardo Torta12,  Marco Arreghini13,
Marco Arreghini13,  Loredana Zanini13,
Loredana Zanini13,  Amelia Brunani13, Ionathan Seitanidis13, Giuseppe Ventura13,
Amelia Brunani13, Ionathan Seitanidis13, Giuseppe Ventura13,  Paolo Capodaglio13,
Paolo Capodaglio13,  Guido Edoardo D’Aniello1,2,
Guido Edoardo D’Aniello1,2,  Federica Scarpina1, Andrea Brioschi14, Matteo Bigoni14, Lorenzo Priano12,14,
Federica Scarpina1, Andrea Brioschi14, Matteo Bigoni14, Lorenzo Priano12,14,  Alessandro Mauro12,14,
Alessandro Mauro12,14,  Giuseppe Riva1,2,
Giuseppe Riva1,2,  Daniele Di Lernia2,
Daniele Di Lernia2,  Claudia Repetto2, Camillo Regalia2,
Claudia Repetto2, Camillo Regalia2,  Enrico Molinari1,2,
Enrico Molinari1,2,  Paolo Notaro15,
Paolo Notaro15,  Stefano Paolucci16,
Stefano Paolucci16,  Giorgio Sandrini17,18, Susan Simpson19,20,
Giorgio Sandrini17,18, Susan Simpson19,20,  Brenda Kay Wiederhold21,
Brenda Kay Wiederhold21,  Santino Gaudio22,
Santino Gaudio22,  Jeffrey B. Jackson23,
Jeffrey B. Jackson23,  Stefano Tamburin24 and Fabrizio Benedetti12 On Behalf of the Italian Consensus Conference on Pain in Neurorehabilitation
Stefano Tamburin24 and Fabrizio Benedetti12 On Behalf of the Italian Consensus Conference on Pain in Neurorehabilitation - 1Istituto Auxologico Italiano IRCCS, Psychology Research Laboratory, San Giuseppe Hospital, Verbania, Italy
- 2Department of Psychology, Catholic University of Milan, Milan, Italy
- 3Faculty of Psychology, eCampus University, Novedrate, Italy
- 4Cardinal Ferrari Rehabilitation Center, Santo Stefano Rehabilitation Istitute, Fontanellato, Italy
- 5Pain Medicine Center, San Pio X Clinic, Humanitas, Milan, Italy
- 6IRCCS Galeazzi Orthopedic Institute, Milan, Italy
- 7Department of Dynamic and Clinical Psychology, Sapienza University of Rome, Rome, Italy
- 8HD Respiratory Rehabilitation Unit, IRCCS Fondazione Don Carlo Gnocchi, Milan, Italy
- 9Department of Psychology, Harvard University, Cambridge, MA, United States
- 10Department of Psychology, University of Turin, Turin, Italy
- 11Anesthesia and Intensive Care, ASST Lecco, Lecco, Italy
- 12Department of Neuroscience "Rita Levi Montalcini", University of Turin, Turin, Italy
- 13Istituto Auxologico Italiano IRCCS, Rehabilitation Unit, San Giuseppe Hospital, Verbania, Italy
- 14Istituto Auxologico Italiano IRCCS, Department of Neurology and Neurorehabilitation, San Giuseppe Hospital, Verbania, Italy
- 15Pain Medicine, Anesthesiology Department, A.O. Ospedale Niguarda ca Granda, Milan, Italy
- 16Fondazione Santa Lucia IRCCS, Rome, Italy
- 17C. Mondino National Neurological Institute, Pavia, Italy
- 18Department of Brain and Behavioral Sciences, University of Pavia, Pavia, Italy
- 19University of South Australia, Adelaide, SA, Australia
- 20Regional Eating Disorders Unit, NHS Lothian, Livingston, United Kingdom
- 21Virtual Reality Medical Institute, Brussels, Belgium
- 22Department of Neuroscience, Functional Pharmacology, Uppsala University, Uppsala, Sweden
- 23Virginia Tech, Falls Church, VA, United States
- 24Department of Neurosciences, Biomedicine and Movement Sciences, University of Verona, Verona, Italy
Background: It is increasingly acknowledged that the outcomes of medical treatments are influenced by the context of the clinical encounter through the mechanisms of the placebo effect. The phenomenon of placebo analgesia might be exploited to maximize the efficacy of neurorehabilitation treatments. Since its intensity varies across neurological disorders, the Italian Consensus Conference on Pain in Neurorehabilitation (ICCP) summarized the studies on this field to provide guidance on its use.
Methods: A review of the existing reviews and meta-analyses was performed to assess the magnitude of the placebo effect in disorders that may undergo neurorehabilitation treatment. The search was performed on Pubmed using placebo, pain, and the names of neurological disorders as keywords. Methodological quality was assessed using a pre-existing checklist. Data about the magnitude of the placebo effect were extracted from the included reviews and were commented in a narrative form.
Results: 11 articles were included in this review. Placebo treatments showed weak effects in central neuropathic pain (pain reduction from 0.44 to 0.66 on a 0–10 scale) and moderate effects in postherpetic neuralgia (1.16), in diabetic peripheral neuropathy (1.45), and in pain associated to HIV (1.82). Moderate effects were also found on pain due to fibromyalgia and migraine; only weak short-term effects were found in complex regional pain syndrome. Confounding variables might have influenced these results.
Clinical implications: These estimates should be interpreted with caution, but underscore that the placebo effect can be exploited in neurorehabilitation programs. It is not necessary to conceal its use from the patient. Knowledge of placebo mechanisms can be used to shape the doctor–patient relationship, to reduce the use of analgesic drugs and to train the patient to become an active agent of the therapy.
Introduction
The placebo effect can be defined as the improvement in the patient’s symptoms after the administration of an inert substance in a context inducing positive expectations about its effects (1, 2). This phenomenon is raising a growing interest in the field of pain management in patients with neurological disorders. Neurorehabilitation treatments could be delayed or hampered by pain symptoms, whose management could be particularly difficult since the available treatments may provide only a moderate relief at the cost of various undesirable side effects (3–5). In this context, knowledge of the mechanisms of the placebo effect could be important. Rather than representing an alternative treatment modality, this phenomenon can be exploited to enhance the effectiveness of the care (6).
In the last decades, research has shifted its focus from the inert substance to the psychosocial context surrounding its administration. The placebo response can be considered as a form of contextual healing, since the beneficial outcome is due to the context of the clinical encounter, rather than to a specific efficacy of the actual treatment (7–9). This complex phenomenon can be described as the emerging effect of the doctor–patient relationship and of the psychosocial context in which it takes place (10). The patient’s memory of previous treatments, personal characteristics, and expectations modulate and are modulated by the interaction with the doctor, whose characteristics and expectations, in turn, influence the context of the encounter. Therefore, the therapeutic ritual itself is the trigger of the placebo effect (11).
The placebo effect is grounded in physiological mechanisms. Different processes can be involved, depending both on the physical or psychological state of the patient and on the context. Various theoretical frameworks have been proposed to understand them, each focusing on a different set of variables, such as conditioning processes, patient expectations, individual attributions, and contextual factors (2, 12). Each of these processes was found to involve different neurobiological mechanisms, including opioid, endocannabinoid, or dopamine ones (13–20). The presence of various mechanisms seems to reflect the complexity of the phenomenon, as well as the variety of neurobiological, psychological, and psychosocial processes involved.
The placebo effect varies across individuals and disorders. Studies are increasingly shedding some light on the individual differences, focusing on the role of genetics (21–23), on differences in the activation of the reward system (16), on differences in expectancy mechanisms and in the emotional appraisal of situations (24), or on the role of psychological variables. Among them, preliminary data corroborate the role of dispositional optimism and state anxiety (25–27), various personality traits (28, 29), hypnotizability and suggestibility (30, 31), reappraisal ability (32), beliefs (33), learning mechanisms (34), and traits linked to dopaminergic mechanisms such as novelty seeking (35).
On the other hand, differences across disorders have received less attention, especially in the field of neurorehabilitation. To exploit the analgesic potential of placebo treatments in this field, knowledge about its differential effects is required. On behalf of The Italian Consensus Conference on Pain in Neurorehabilitation (ICCPN), a multidisciplinary board aimed at developing the national guidelines on the assessment and treatment of pain in neurorehabilitation, our working group was established to summarize the available studies on this topic.
Methods
A review of the existing reviews and meta-analyses examining the role of the placebo effect in disorders that may undergo neurorehabilitation treatment was performed. This research design was chosen since (a) it allowed to summarize a high amount of studies on such a broad topic and (b) literature reviews focusing on each disorder were already present. Both systematic and non-systematic reviews were considered for inclusion since it was hypothesized that the quality of the existing literature about each disorder would be heterogeneous. Studies were, therefore, included if they reported reviews, with or without meta-analysis, presenting data about the effects of a placebo treatment on pain intensity in disorders that may undergo neurorehabilitation treatment. Only articles written in English language were considered. Studies were excluded if they did not report summary data about the effects of placebo treatments.
An initial search was performed on July 2014, imposing no restraints on the articles’ publication date. Subsequently, a research update took place on March 2017, restraining the search to articles published from 2014 to 2017. Both the searches were performed on PubMed using the following keywords: “placebo” (research restricted to the title) “nervous system disease” (as a MeSH word), the names of the primary neurological disorders and “pain.” The inclusion and exclusion criteria were used by one of the authors to judge the eligibility of the studies based on the articles’ titles, abstracts and, finally, full texts. The bibliographies of the selected articles were analyzed to identify other potentially relevant reviews. The methodological quality of included studies was then assessed using the Critical Appraisal Checklist for Systematic Reviews (Table 1) (36). When assessing the methodological quality of non-systematic reviews, items from 5 to 8 of this checklist were not considered.
TABLE 1
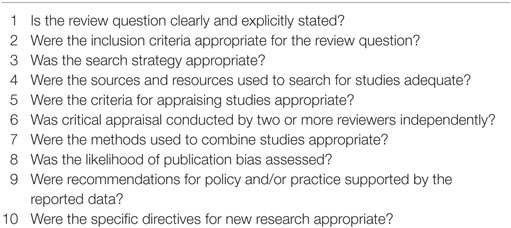 Table 1. Critical Appraisal Checklist for Systematic Reviews.
Table 1. Critical Appraisal Checklist for Systematic Reviews.
The following data were extracted from the included reviews: study design of the review, disorder addressed by the review, participants’ details, study design of the included studies, number of electronic databases accessed during the search, date range of the search, number of studies included, number of subjects included in placebo arms, total number of subjects, instruments used by the studies to assess pain intensity, and quantitative results. Since the aim of the present review was not to assess if placebo treatments are evidence-based interventions, the quality of evidence was not graded and no recommendations were made. Instead, the results of the reviews were synthesized in a narrative form. Results from excluded reviews or from primary studies that were found during the search that were considered relevant to give insight to areas not explored by the included reviews were also commented.
Results
Overall, the searches yielded 872 records. From this sample, 11 reviews were included in the present review. The flowchart of the study search and selection is reported in Figure 1.
FIGURE 1
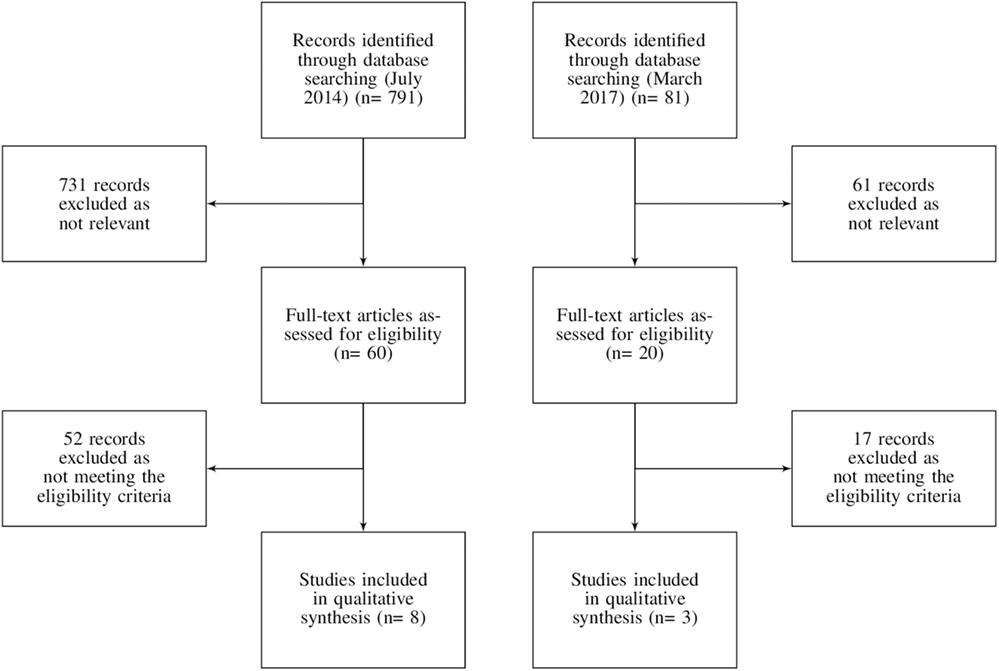 Figure 1. Flowchart of the records search and selection.
Figure 1. Flowchart of the records search and selection.
Among the included reviews, 10 out of 11 were systematic and 9 included a meta-analysis. Five of these reviews focused on peripheral and/or central neuropathic pain disorders, three on migraine and the remaining on chronic regional pain syndrome, fibromyalgia, or mixed chronic pain conditions. The characteristics of the studies are reported in Table 2.
TABLE 2
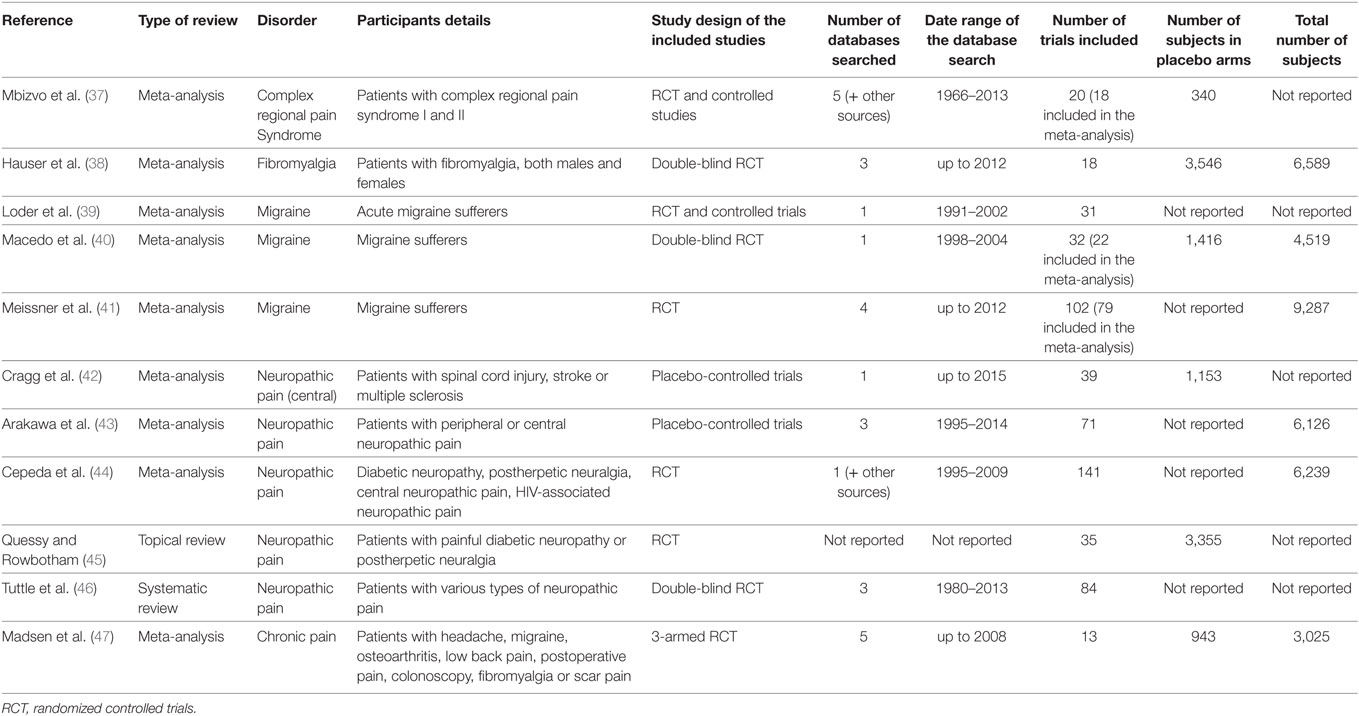 Table 2. Description of the included reviews.
Table 2. Description of the included reviews.
The methodological quality of the included reviews was variable (Table 3). Among the systematic reviews, three studies did not meet at least six items of the critical appraisal checklist (39, 40, 44), but none of them showed substantial biases that may hinder the interpretation of their results.
TABLE 3
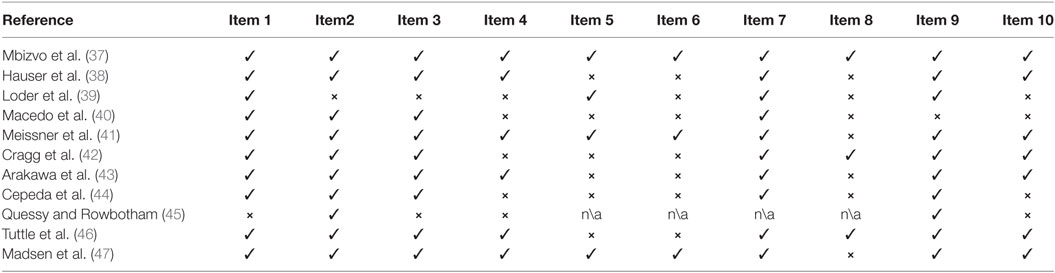 Table 3. Quality assessment of the included reviews.
Table 3. Quality assessment of the included reviews.Placebo Effect in Pain Conditions in Neurorehabilitation
The main quantitative results of the included reviews generally show that the placebo effect has a low to moderate effect on pain across the various disorders (Table 4). However, differences are visible, especially when neuropathic and non-neuropathic pain disorders are contrasted.
TABLE 4
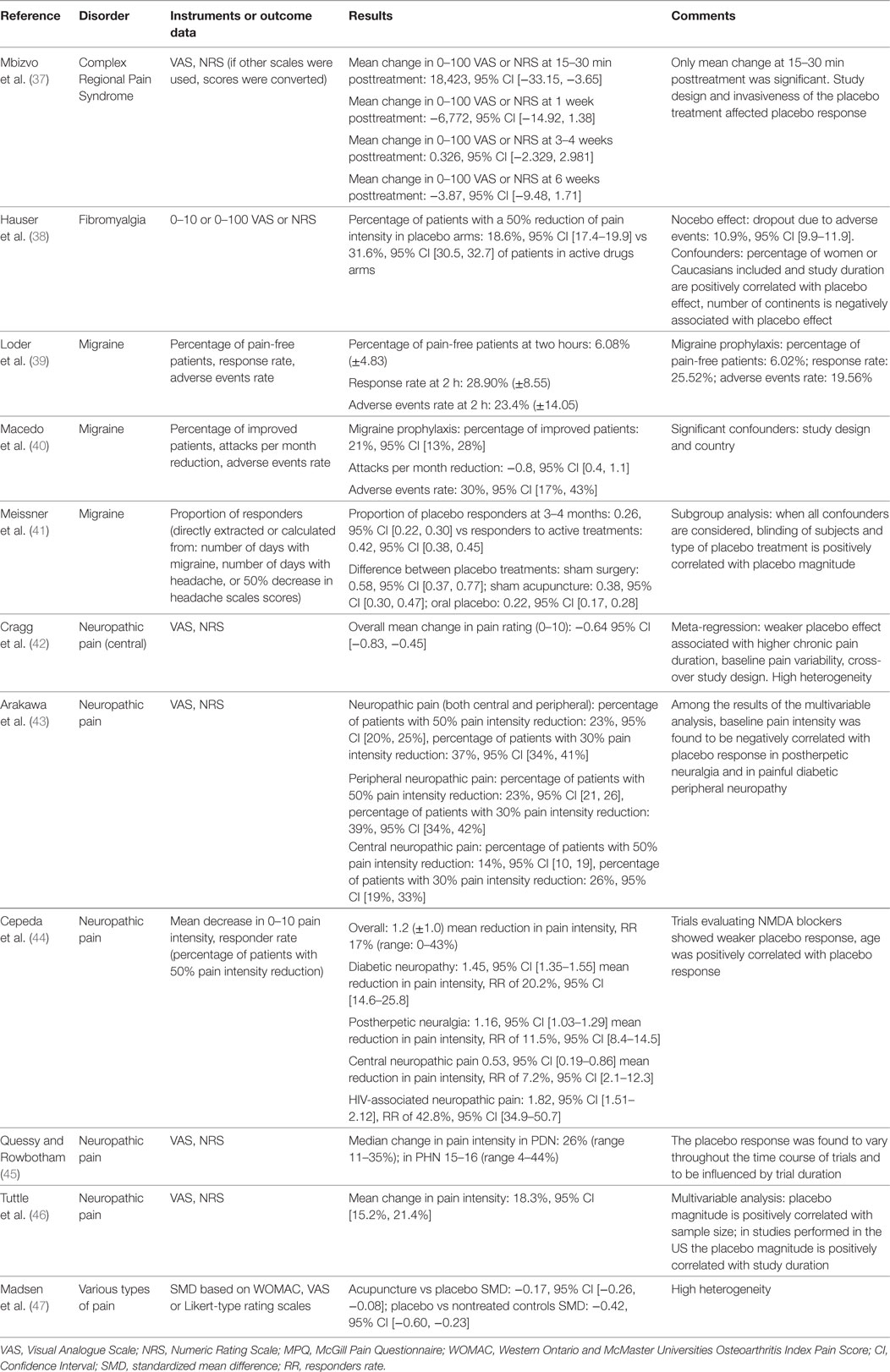 Table 4. Quantitative findings of the included reviews.
Table 4. Quantitative findings of the included reviews.
Various reviews and meta-analyses addressed the role of placebo in neuropathic pain disorders and found a noticeable heterogeneity between peripheral and central ones (43–46). In general, the placebo effect was found to be more intense in the former than in the latter. A meta-analytic study estimated the intensity of the placebo effect in various neuropathic pain disorders, and explored both the average pain reduction and the percentage of patients who positively responded to the placebo treatment (44). On a 0–10 scale, the average decrease in pain severity was 1.82 in pain associated with HIV (percentage of positive responders: 48.2%), 1.45 in painful diabetic peripheral neuropathy (percentage of positive responders: 20%), 1.16 in postherpetic neuralgia (percentage of positive responders: 11.5%), and between 0.44 and 0.64 in central neuropathic pain (percentage of positive responders: 7.2%) (42, 44). Other studies confirmed that, among the disorders associated with peripheral neuropathic pain, the placebo effect was higher in painful diabetic peripheral neuropathy than in postherpetic neuralgia (43). In contrast, the placebo effect in complex regional pain syndrome, a disorder with some neuropathic characteristics (48), seems to be nearly absent, with only weak short-term effects (37). In neuropathic pain disorders, the intensity of the placebo effect is modulated by the duration of treatment, with longer treatments associated with increased effects, and by the duration and intensity of initial pain, with longer duration of and higher intensity associated with a reduced placebo response (42, 43, 45).
The intensity of the placebo effect is generally higher in non-neuropathic pain disorders. A meta-analysis by Madsen et al. (47) compared the effects of acupuncture, placebo acupuncture, and a no-treatment condition on pain from various disorders, including headache (tension type, migraine), nociceptive pain (osteoarthritis, low back pain), iatrogenic pain (postoperative, procedural pain during colonoscopy, abdominal scar pain), and fibromyalgia. In this study, acupuncture was found to have slightly stronger effects (i.e., 0.4 points on a 0–10 scale) than placebo acupuncture, whereas a moderate difference (i.e., 1.0 points) was found between placebo acupuncture and no acupuncture conditions.
Hauser et al. (38) studied both the placebo and the nocebo effect in the management of fibromyalgia, and estimated that the percentage of patients experiencing a 50% pain reduction after a placebo treatment was 18.6% and that the dropout rate due to adverse events was 10.9%. In contrast, groups receiving a true drug showed a higher rate of responders (31.6%) and a higher dropout rate due to adverse events (20.4%). This study did not compare the improvement in the placebo group with that in the untreated groups.
Despite the variability of their effects, placebo treatments were found to be associated with both short- and long-term improvements in migraine sufferers (39, 41). Placebo groups showed an improvement of pain symptoms in 26% of cases, and 21% of patients taking placebo for migraine prophylaxis improved. For both outcomes, the efficacy of the placebo treatment was estimated to be half of that of active drugs. The placebo treatment type influenced its efficacy, with sham acupuncture and sham surgery being more effective than oral placebos (41). These effects were accompanied by a high rate of adverse events (39–41). The presence of adverse events in case of placebo administration is in line with the nature of placebo, since their characteristics are generally similar to the characteristics of the active drugs against which placebo is compared (49).
The size of the placebo effect and its variability across disorders and type of placebo treatment is apparent also when non-neurological disorders are considered. It was estimated that placebo treatments for osteoarthritis resulted in an overall moderate effect (effect size = 0.51) and that topical and intra-articular placebos are more effective than oral ones (effect size differences of 0.20 and 0.29, respectively) (50, 51). Other estimates show that the size of the placebo effect is equivalent to 72% of that of the drug treatment in burning mouth syndrome (52) and that it leads to pain remission rates of 19.9% in chronic pancreatitis (53).
Implications for Clinical Practice
The effectiveness of placebo treatments should not be overestimated. Most of the studies on this topic showed high heterogeneity and did not take into account confounding variables, such as spontaneous remission of symptoms or regression toward the mean, thus potentially overestimating the intensity of the placebo response. In addition, various authors underlined that (a) placebo effect is higher when subjective rather than objective outcome measures are explored (54); (b) bias may be present in patients’ responses (54); (c) each individual responds differently to placebos (55, 56), and (d) outcomes vary consistently across studies and methodological design (57). These limitations are prominent in studies on placebo treatments, and may impede to predict their effects in routine clinical practice. It is recommended to take these treatments into consideration in neurorehabilitation settings only after traditional ones have failed or are contraindicated (58–64).
Rather than simply representing an alternative type of treatment, the placebo effect is a phenomenon that can increase the effectiveness of the care, since it constitutes the process through which the doctor–patient relationship becomes therapeutic. The knowledge of relevance of the placebo effect for each specific pain disorder is recommended to exploit its potential. For example, placebo response is generally small in central neuropathic pain, where pharmacological and non-pharmacological treatments have also limited efficacy, while it appears to represent half of the effect of active treatments in the prophylaxis of primary headaches. This information is central to shape the communication with the patient, allowing to provide a trustworthy explanation of the positive effects of the therapeutic context.
It is increasingly acknowledged that concealment is not necessary for the placebo effect to take place. Research on open-label placebos treatments, i.e., non-deceptive treatments in which the participants are alerted that the therapeutic mean is inert, but are informed about the effects of the administration of placebos, corroborates this claim. Further studies are needed, but open-label placebo treatments seem to have a similar or even higher efficacy than deceptive ones and are associated with marked improvement of symptoms of a variety of conditions (65–70). These treatments are more easily accepted by patients (71) and overcome the ethical and legal implications of the deceitful prescription of placebos, which violates the principle of the informed consent and may affect the trust that shape the doctor–patient relationship (72, 73).
Various techniques can be used to improve the patient’s symptoms through placebo mechanisms. A possible strategy is to maximize the patient’s expectations regarding the treatment. This can be done by informing the patient on the nature and effects of placebo analgesia, by assessing the appropriateness of the patient’s beliefs about his disorder and its treatment and providing information in case they are excessively positive or negative. In this case, it would be important to balance the information regarding the positive and negative effects of the treatment, underlying the role of the positive ones despite its undesired effects, and by cognitively reinforcing the impact of the positive outcomes as they appear (74–76). Furthermore, it is possible to exploit conditioning mechanisms to support the pharmacological therapy. Once the person associates the characteristics of the analgesic agent, such as appearance and taste, to the reduction of pain, it could be possible to employ inert substitutes with the same characteristics to obtain similar results (6). Using similar methods, it would be possible, after an adequate initial conditioning, to progressively reduce the administration of medication by alternatively switching to a placebo with similar characteristics (74, 77). Finally, the patient can also be trained to create those conditions that maximize the placebo effect, for example by focusing on the characteristics of the analgesic agent or by increasing his own expectations through appropriate information (75).
It should be underscored that all these techniques need to take place within the context of a doctor–patient relationship. The relational aspect of the placebo effect resides in the person’s feeling of being taken care for and in the process by which he himself becomes an active agent of the therapy (78). Having an empathic attitude, reassuring the patient, helping him to self-manage his symptoms, emphasizing the role of interpersonal resources and creating therapeutic rituals during therapy represent key aspects of the relationship.
In conclusion, the neurorehabilitation team needs to address a variety of disorders, each of which responds differently to the placebo effect. It is, therefore, necessary to personalize all these features depending on the disorder and on the patient’s characteristics. Studies are beginning to clarify the genetic, biological, psychological, and contextual factors that may enable to identify subjects with high or low likelihood of experiencing a placebo response (22, 28). To exploit the placebo effect, the doctor should collect information regarding not only about the patient’s disorder, but also about his personal characteristics and his context (74). The context of the doctor–patient relationship should be shaped so that the doctor does not focus only on the treatment of pain as a symptom of the neurological disorder, but is able to take care of the person as a whole.
No comments:
Post a Comment