So where is the protocol for this located so survivors can find it and bring it to their doctor's attention?
Balance Rehabilitation through Robot-Assisted Gait Training in Post-Stroke Patients: A Systematic Review and Meta-Analysis
by
1,2,* , 1,2, 1,2, 3, 4, 5, 6, 7, 8, 8, 9, 10, 11, 12, 13, 14, 15, 8, 16, 17, add
Show full author list
, 1,2, 1,2, 3, 4, 5, 6, 7, 8, 8, 9, 10, 11, 12, 13, 14, 15, 8, 16, 17, add
Show full author list
 , 1,2, 1,2, 3, 4, 5, 6, 7, 8, 8, 9, 10, 11, 12, 13, 14, 15, 8, 16, 17, add
Show full author list
, 1,2, 1,2, 3, 4, 5, 6, 7, 8, 8, 9, 10, 11, 12, 13, 14, 15, 8, 16, 17, add
Show full author list
1 Department of Health Sciences, Università del Piemonte Orientale “Amedeo Avogadro”, 28100 Novara, Italy
2 Physical Medicine and Rehabilitation Unit, AOU Maggiore della Carità University Hospital, 28100 Novara, Italy
3 Physical Medicine and Rehabilitation Unit, Polyclinic of Bari, 70124 Bari, Italy
4 Rehabilitation Unit, Castel San Giovanni Hospital, 29015 Piacenza, Italy
5 Theology Department, Pontifical Gregorian University, 00187 Rome, Italy
6 Physical Medicine and Rehabilitation, ASST Sette Laghi, 21100 Varese, Italy
7 Casa di Cura Domus Salutis, Fondazione Teresa Camplani, 25100 Brescia, Italy
8 Robotic Rehabilitation Section, Italian Society of Physical and Rehabilitative Medicine (SIMFER), 00187 Rome, Italy
9 Neurorehabilitation Department, IRCCS Fondazione Don Carlo Gnocchi, 20148 Milan, Italy
10 Experimental and Clinic Medicine Department, Università Politecnica delle Marche (UNIVPM), 60126 Ancona, Italy
*
Author to whom correspondence should be addressed.
Brain Sci. 2023, 13(1), 92; https://doi.org/10.3390/brainsci13010092
Received: 1 December 2022
/
Revised: 21 December 2022
/
Accepted: 29 December 2022
/
Published: 3 January 2023
(This article belongs to the Special Issue Robot-,
Virtual Reality- and Sensor-Based Therapies Boosting Neuroplasticity in
the Context of Motor and Cognitive Neurorehabilitation: Current State
of the Art and Applications)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Background:
Balance impairment is a common
disability in post-stroke survivors, leading to reduced mobility and
increased fall risk. Robotic gait training (RAGT) is largely used, along
with traditional training. There is, however, no strong evidence about
RAGT superiority, especially on balance. This study aims to determine
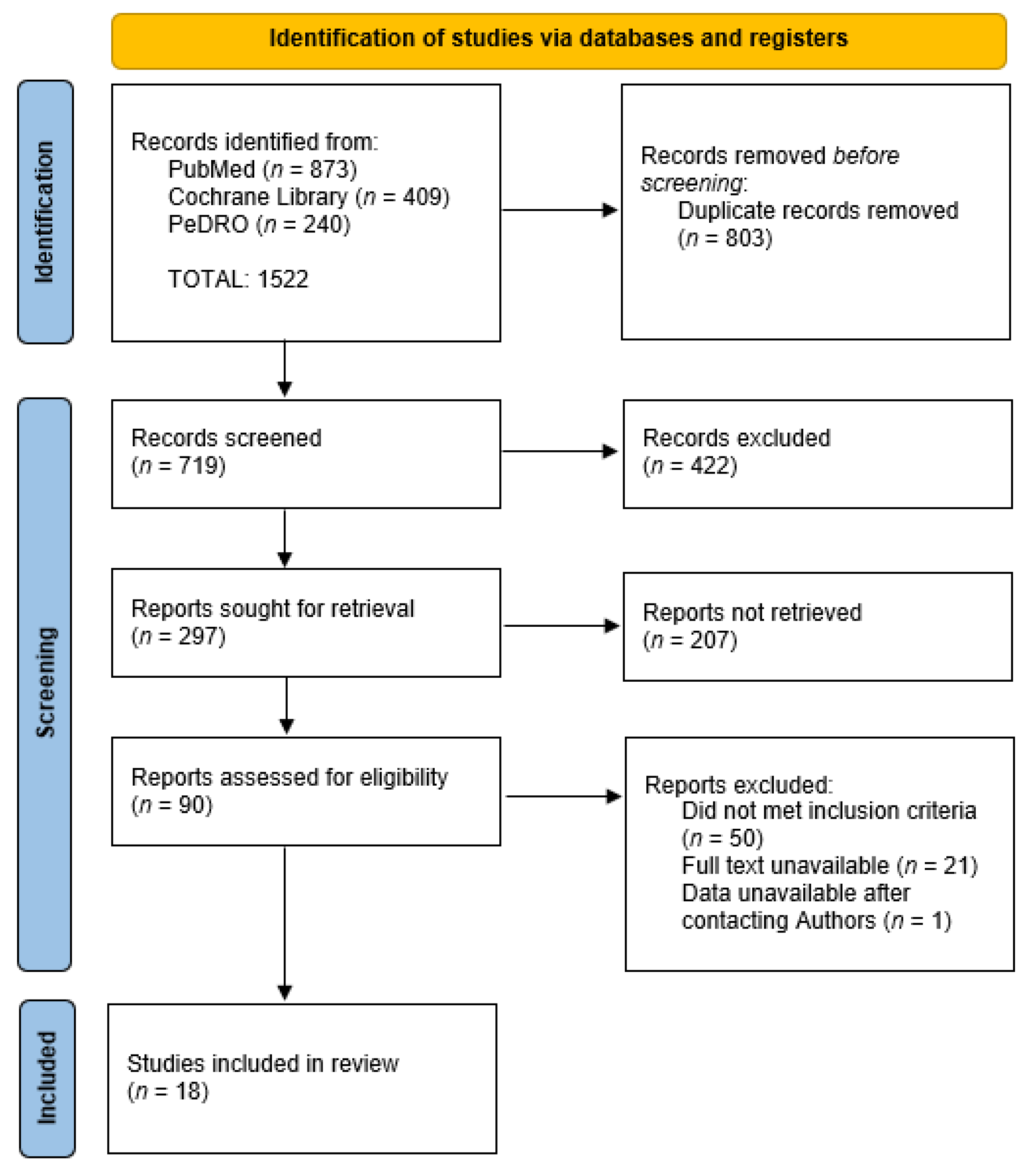
RAGT efficacy on balance of post-stroke survivors. Methods: PubMed,
Cochrane Library, and PeDRO databases were investigated. Randomized
clinical trials evaluating RAGT efficacy on post-stroke survivor balance
with Berg Balance Scale (BBS) or Timed Up and Go test (TUG) were
searched. Meta-regression analyses were performed, considering weekly
sessions, single-session duration, and robotic device used. Results:
A
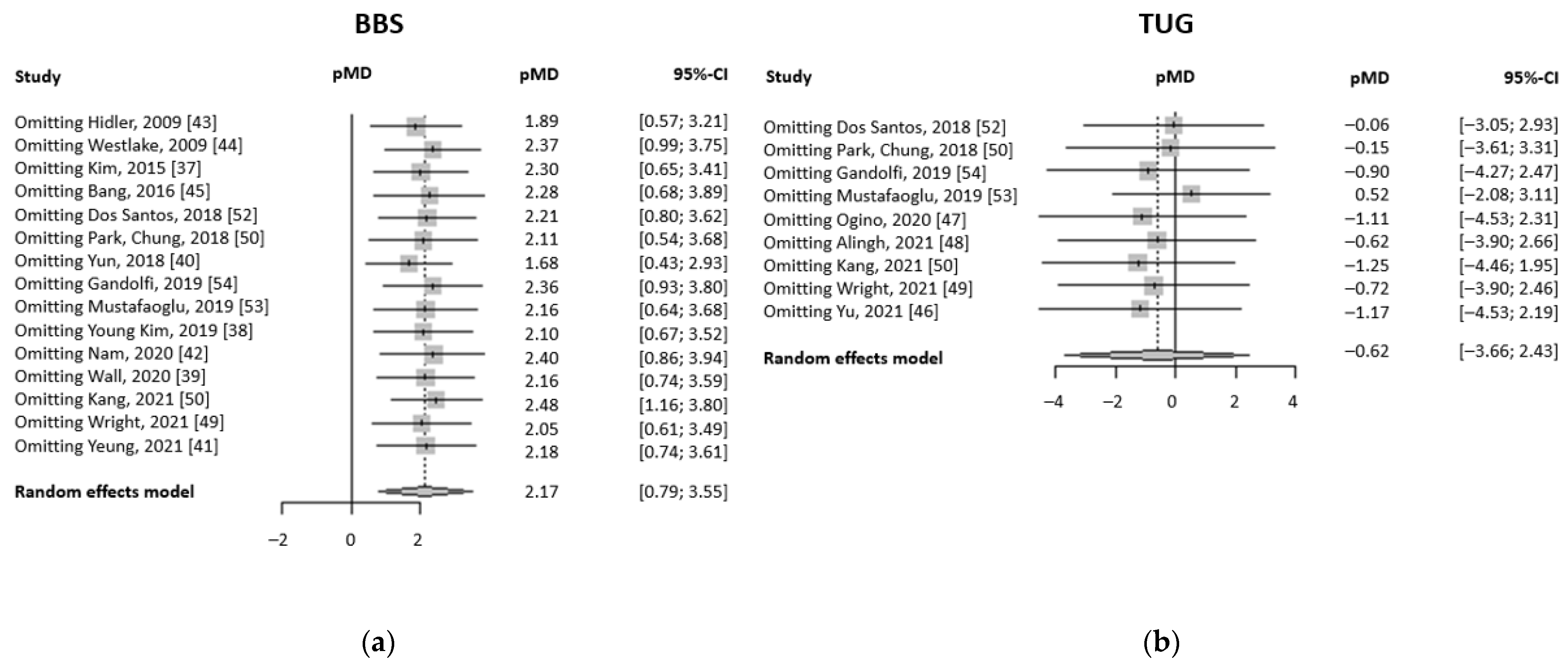
total of 18 trials have been included. BBS pre-post treatment mean
difference is higher in RAGT-treated patients, with a pMD of 2.17 (95%
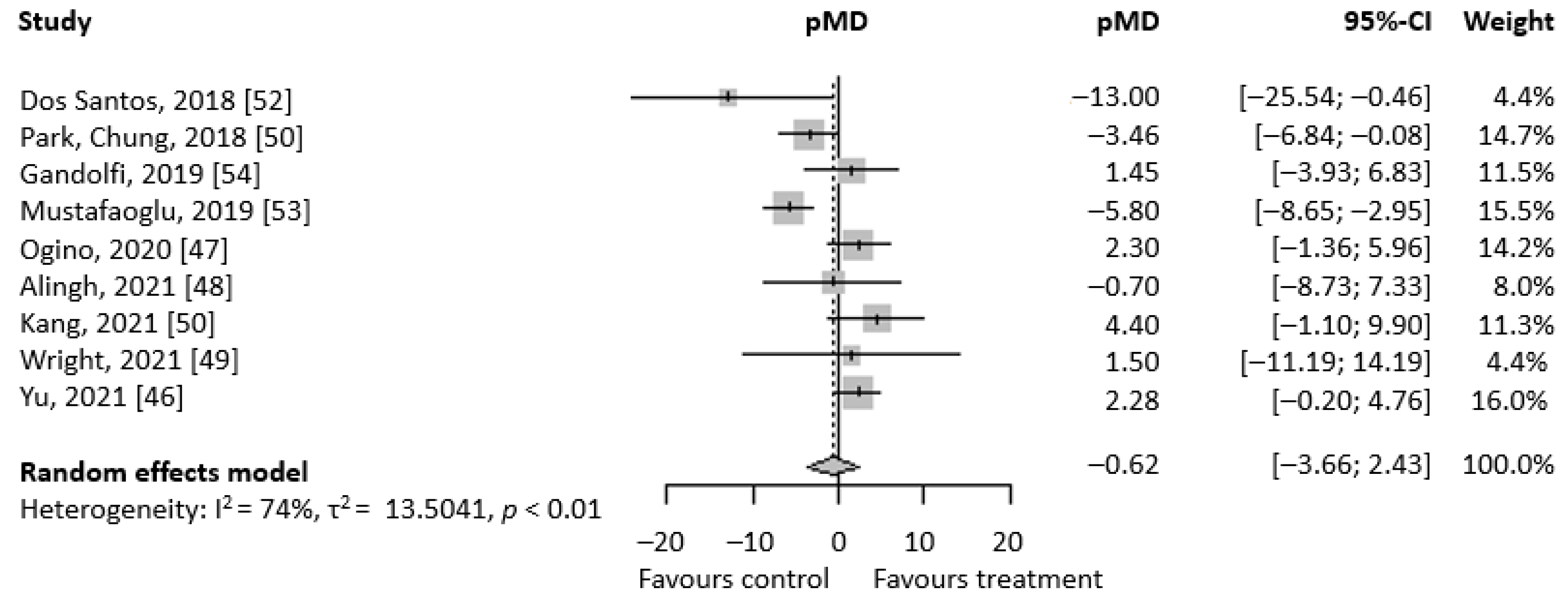
CI 0.79; 3.55). TUG pre-post mean difference is in favor of RAGT, but
not statistically, with a pMD of −0.62 (95%CI − 3.66; 2.43).
Meta-regression analyses showed no relevant association, except for TUG
and treatment duration (β = −1.019, 95% CI − 1.827; −0.210, p-value
= 0.0135).
Conclusions:
RAGT efficacy is equal to traditional therapy,
while the combination of the two seems to lead to better outcomes than
each individually performed. Robot-assisted balance training should be
the focus of experimentation in the following years, given the great
results in the first available trials. Given the massive heterogeneity
of included patients, trials with more strict inclusion criteria
(especially time from stroke) must be performed to finally define if and
when RAGT is superior to traditional therapy.
1. Introduction
Stroke
is the second leading cause of death and the first cause of disability
in the world. Given the rising mean age of the world’s population, the
incidence of stroke is also steadily increasing, leading to higher
economic burden through the years [1,2,3,4].
Aphasia
and depression are often the causes of disability in post-stroke
patients, but the most common disability tract is a reduced mobility due
to hemiparesis [1,5].
This impairment is strictly connected to two main factors: a rapid
change in muscle thickness and composition (visible within 1 month from
the onset) and reduced central motor control [6,7].
All these impairments also lead to a reduced balance function: the
patient is unable to maintain his center of gravity within his support
base with or without the action of external forces [8].
After the clinical stabilization of the acute stroke, the
rehabilitation program is usually focused on upper limb and gait
rehabilitation, while balance is often a secondary or ignored outcome.
This is a problematic point of rehabilitation programs because balance
is a skill deeply involved in patients’ autonomy and independence. As a
matter of fact, balance is not only fundamental in walking but also in
many activities of daily life (ADL). It is also the main deficit
involved in fall risk evaluation [9].
Nowadays,
it is well known that an early and intensive mobilization protocol
improves functional recovery after stroke, especially in young patients [10].
Along with the development of acute stroke management (early
rehabilitation in stroke units, facilitation of brain repair mechanisms
and experimental approaches, such as neuronal transplantation) [11],
the management and rehabilitation of chronic stroke patients have
recently seen great improvement. The greatest effort in stroke
rehabilitation can be identified in four main outcome domains: physical
fitness, ADL, arm-hand dexterity and function, and gait and
mobility-related functions and activities [12].
Regardless of the main outcome pursued, many different
neurorehabilitation techniques have been developed over the years for
both sub-acute and chronic stroke survivors. Functional electrical
stimulation (FES) has been largely used to contract muscles that are
non-activable by the patient, improving complex motor function, such as
gait. Along with peripheral stimulation, brain stimulation has been
developed over the years. Transcranial direct current stimulation (tDCS)
can be integrated during the rehabilitation program to improve limb
movement and pain [13].
Manual therapy for strength and mobility recovery is the most used
approach worldwide but is difficult to standardize, and it is heavily
related to therapist dexterity and experience [14].
That is why, in the last 20 years, many technological devices have been developed, for both upper [15,16,17,18,19,20] and lower limb rehabilitation [21,22,23,24,25,26,27,28].
In this scenario, we can find many levels of assistance, with different
ideas of rehabilitation beneath. First of all, there is the body
weight-supported treadmill, in which the patients can practice a
supervised and repetitive walk. Then, we can find overground
exoskeleton, which provide patients with either full or partial guidance
of the lower limbs during the whole gait cycle [13].
Lastly, there are also end-effectors, which are smaller devices that
permit the patient to perform a specific joint movement during specific
gait phases [29].
The development of these devices has improved the quality of
post-stroke rehabilitation, guaranteeing patients early verticalization,
gait training, and dismission [30,31,32].
The
use of robotics for lower limb rehabilitation is currently starting to
spread widely, but given the various protocols available worldwide,
there is no consensus on which approach is the most effective [10].
Moreover, there is a lack of knowledge about the superiority of robotic
treatment over standard treatment and which of the patients’
characteristics are to be considered when deciding whether or not to
treat them with robotic devices. Furthermore, while there is some
evidence on the efficacy of these devices for gait rehabilitation [33,34,35],
more evidence on the balance outcomes is needed. More precisely, very
few trials on robotic rehabilitation consider balance as an outcome and
all the previous meta-analyses performed were not able to gather enough
data to provide a sufficient statistical relevance. In addition,
considering the high cost of these robotic devices, there is no certain
evidence on their efficacy that completely justifies this kind of
expenditure. The aim of this study is to sum up all the evidence about
robotic-assisted gait training (RAGT) on balance rehabilitation. In
particular, the study focuses on covering the lack of statistical
relevance present in the actual literature, due to a small number of
trials included, and tries to assess as many sub-group evaluations as
possible.
More at link.
No comments:
Post a Comment