WHAT ABSOLUTE FUCKING BULLSHIT! Survivors don't want spasticity 'managed', they want it cured! Don't you ever listen to survivor goals?
Management of Upper-Limb Spasticity Using Modern Rehabilitation Techniques versus Botulinum Toxin Injections Following Stroke



1
Department of Physical Medicine and
Rehabilitation, University of Medicine and Pharmacy of Craiova, Petru
Rares 2, 200349 Craiova, Romania
2
Department of Pharmacoeconomics, University of Medicine and Pharmacy of Craiova, Petru Rares 2, 200349 Craiova, Romania
3
Department of Anatomy, University of Medicine and Pharmacy of Craiova, Petru Rares 2, 200349 Craiova, Romania
4
Doctoral School, University of Medicine and Pharmacy of Craiova, Petru Rares 2, 200349 Craiova, Romania
5
Department of Neurology, University of Medicine and Pharmacy of Craiova, Petru Rares 2, 200349 Craiova, Romania
6
Department of Internal Medicine, University of Medicine and Pharmacy of Craiova, Petru Rares 2, 200349 Craiova, Romania
7
Medical Rehabilitation Department, Nursing Faculty, University of Medicine and Pharmacy, Petru Rares 2, 200349 Craiova, Romania
*
Authors to whom correspondence should be addressed.
†
These authors contributed equally to this work.
Life 2023, 13(11), 2218; https://doi.org/10.3390/life13112218
Received: 17 October 2023
/
Revised: 4 November 2023
/
Accepted: 8 November 2023
/
Published: 17 November 2023
(This article belongs to the Special Issue Effects of Exercise Training on Muscle Function)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Our purpose is to emphasize the role of botulinum
toxin in spasticity therapy and functional recovery in patients
following strokes. Our retrospective study compared two groups, namely
ischemic and hemorrhagic stroke patients. The study group (BT group)
comprised 80 patients who received focal botulinum toxin as therapy for
an upper limb with spastic muscle three times every three months. The
control group (ES group) comprised 80 patients who received only medical
rehabilitation consisting of electrostimulation and radial shockwave
therapy for the upper limb, which was applied three times every three
months. Both groups received the same stretching program for spastic
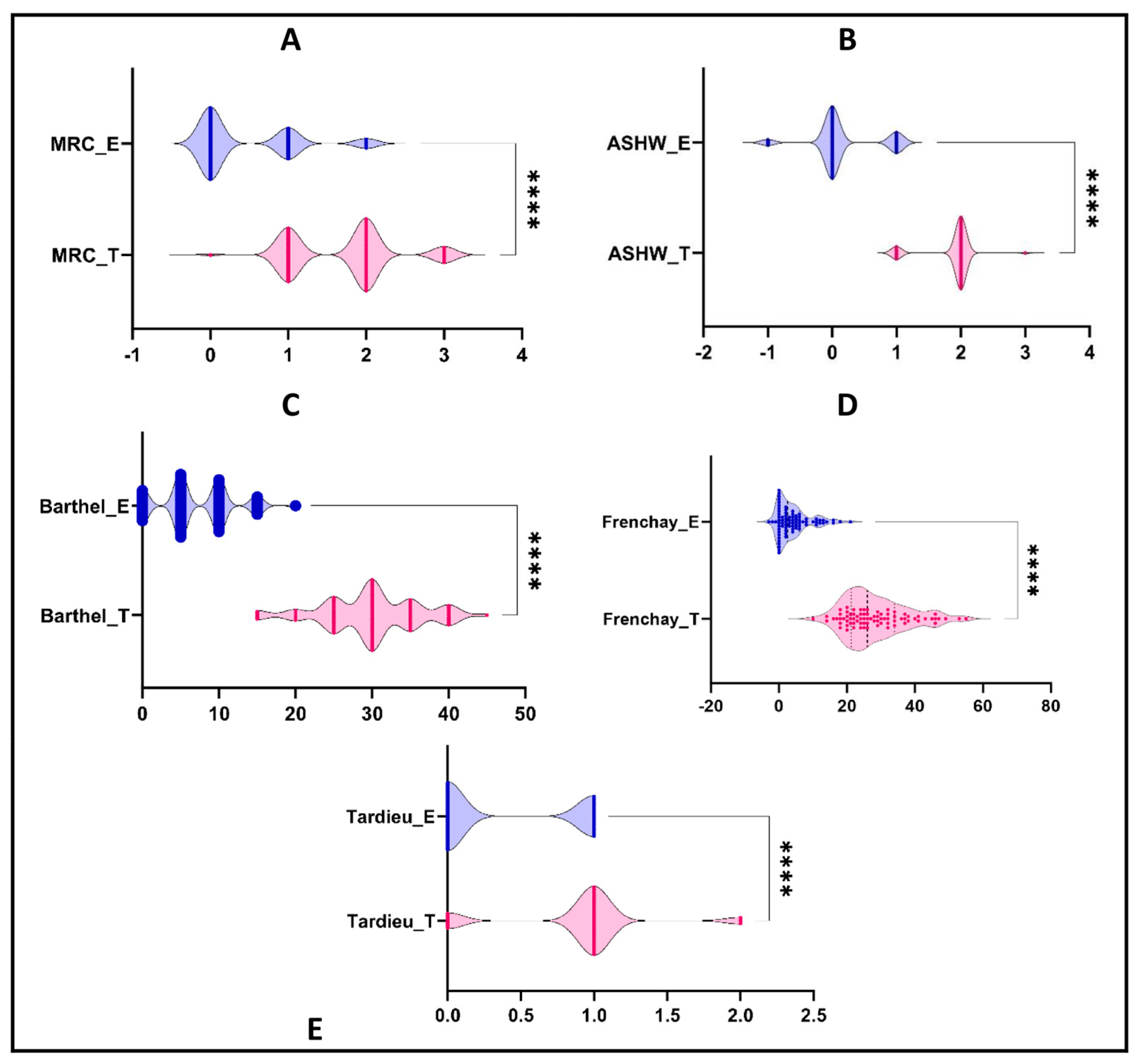
muscles as a home training program. We evaluated the evolution of the
patients using muscle strength, Ashworth, Tardieu, Frenchay, and Barthel
scales. The analysis indicated a statistically significant difference
between the two groups for all scales, with better results(NOT GOOD ENOUGH!) for the BT
group (p < 0.0001 for all scales).
In our study, the age at disease onset was an important prediction
factor for better recovery in both groups but not in all scales. Better
recovery was obtained for younger patients (in the BT group, MRC scale:
rho = −0.609, p-value < 0.0001; Tardieu scale: rho = −0.365, p-value = 0.001; in the ES group, MRC scale: rho = −0.445, p-value < 0.0001; Barthel scale: rho = −0.239, p-value
= 0.033). Our results demonstrated the effectiveness of botulinum toxin
therapy compared with the rehabilitation method, showing a reduction of
the recovery time of the upper limb, as well as an improvement of
functionality and a reduction of disability. Although all patients
followed a specific kinetic program, important improvements were evident
in the botulinum toxin group.
1. Introduction
Stroke
is one of the main causes of mortality and disability in surviving
patients worldwide. More specifically, stroke is the second highest
cause of morbidity and mortality, and motor deficit is the third most
common sequela found in stroke patients [1,2].
Thus,
stroke remains a health problem worldwide. This assertion is supported
by statistical data that are worrying regarding mortality and residual
disability after a stroke. In the European Union in 2017, there were
1.12 million cases of stroke, resulting in 0.46 million deaths and 7.06
million patients with disabilities who required additional medical care,
personal caretakers, and auxiliary medical devices, such as orthoses
and wheelchairs, to improve quality of life. By 2047, it is estimated
that there will be a 3% increase in case incidence, a 27% increase in
prevalence, a 17% decrease in mortality rate, and a 33% decrease in
mortality compared to present figures. The decrease in mortality rate is
estimated to be lower for less-developed countries, such as Romania,
where the estimated mortality rate decrease is only 0.23%. Romania is
one of the top three countries in terms of stroke cases, death, and
disability [3,4].
Stroke
is the second highest cause of death on a world scale, the same as in
Romania, with an increasing trend in incidence and prevalence globally,
so it is estimated that by 2030, it will be the main cause of death
worldwide. Surviving patients, estimated to be an increasing population,
will have a permanent disability, according to the extent of the
stroke, for the rest of their lives. This aspect of permanent
disability, with great effects on the life quality of the patient and
their family, makes this disease a major health problem [5].
In
Romania, stroke prevalence is 252,774 cases per year, with a rate of
8333 cases per 100,000 inhabitants, which represents a very high rate
and explains the interest in finding new therapeutic solutions to
minimize the disability through combined pharmacological and
rehabilitation techniques [6].
The
WHO reports that stroke is the second highest cause of death in
Romania, after heart attack, with a very small difference between the
sexes [7].
Stroke is defined as rapidly developing clinical signs of focal or
global disturbance of cerebral function lasting more than 24 h or
leading to death with no other origin than vascular. In more than 60% of
strokes, there are symptoms related to spasticity. The clinical
characteristics of spasticity are high tone, hyperreflexia, flexor spasm
clasp knife reaction, extensor spasm, and associated reactions [8].
In
stroke patients, there are several stages of evolution. In the early
stage, patients typically exhibit motor deficits, abolished tendon
reflexes, and the appearance of pathological specific reflexes.
Swallowing deficit, sphincter control deficit, impaired speech, and
cognitive disorders may also be observed. The spastic phase begins after
a variable time, usually within a few weeks of the onset of stroke.
Spasticity affects specific muscle groups, such as the flexors of the
upper limbs and the extensors of the lower limbs. The arm tends to
assume a pronated and flexed position, and the leg assumes an adducted
and extended position. These positions indicate that some spinal neurons
are reflexively more active than others. There is no constant
relationship between spasticity and weakness. The pathophysiology of
spasticity is further dependent on two descending tracts: the dorsal
reticulospinal tract and the medial reticulospinal and vestibulospinal
tracts. The dorsal reticulospinal tract has inhibitory effects on
stretch reflexes. Medial reticulospinal and vestibulospinal tracts
facilitate the extensor tone. This is the moment when reflexes
intensify, and it is also the ideal moment to begin rehabilitation. For
adequate rehabilitation, spasticity must be kept at an appropriate level
to initiate and continue rehabilitation [9].
Spasticity is a disorder of the stretch reflex that is clinically manifested by increased muscle tone [10,11]. Also, spasticity is a common condition in post-stroke patients that can be associated with pain and joint contracture [12,13],
which leads to decreased quality of life through vicious limb
positions, deformity, involuntary movement, and medical complications
(skin maceration and pressure sores) when untreated [14].
Spasticity after stroke occurs in approximately one third of patients
and has been shown in many studies to have a negative effect on a
patient’s life and influences upper-limb function negatively [15], which can lead to falls, fractures, and a difficult recovery [16].
The
motor control of the affected limb being deficient causes abnormal
movements, misdirected systematically, which is a primary consequence of
brain injury and a secondary non-use consequence [17].
Reducing
disability and recovery time is an increasingly important aspect
nowadays, given the high costs and socioeconomic implications. Thus,
finding new therapeutic methods to reduce the remaining spasticity
becomes a major objective. Spasticity management is a complex mechanism
that requires a holistic approach which includes pharmacological therapy
associated with adequate and personalized rehabilitation programs. The
objective of spasticity treatment is to reduce the motor hyperactivity
and improve mobility, but without accentuating the motor deficit [18].
The
advantages of local therapy over other spasticity treatments are that
unlike the systemic anti-spasticity drugs which are commonly associated
with generalized weakness and functional loss, botulinum toxin is a
targeted therapy and unlike chemical neurolysis with alcohol or phenol
injection does not causes skin sensory loss or dysesthesia [8].
The
pharmacological treatment for spasticity in stroke patients includes
both focal, localized administration of medication in the spastic muscle
and also conventional oral therapy. Systemic therapy distributes
medication throughout the body, without specifically targeting the
spastic muscle, making it less beneficial for patients. On the other
hand, focal therapy involves injecting botulinum toxin directly into the
spastic muscle, the target zone of treatment, using ultrasound-guided
in situ injection with a precise and personalized dosage, for each
muscle group, every 3 months or more [14,16].
The
objectives of our study were to highlight the differences between
botulinum toxin type A (incobotulinum toxin and abobotulinum toxin) and
recovery therapy, combined with specific kinetic programs, in the
management of spasticity and functionality in stroke patients. We aimed
to emphasize that the association of a kinetic program with focal
therapy with botulinum toxin leads to better results compared to those
of the group that received the same kinetic program but with
electromyostimulation and radial shockwaves. This combination proves
more effective in enhancing muscle force and functionality and reducing
spasticity to a convenient level.(Spasticity is never convenient, you blithering idiots! Survivors want it cured!)
More at link.
No comments:
Post a Comment