http://journal.frontiersin.org/article/10.3389/fpsyg.2015.00768/full?utm_source=newsletter&utm_medium=email&utm_campaign=Psychology-w28-2015
Ken Rosslau1,2*,
 Daniel Steinwede2, C. Schröder2,3,
Daniel Steinwede2, C. Schröder2,3,  Sibylle C. Herholz4, Claudia Lappe5, Christian Dobel5 and
Sibylle C. Herholz4, Claudia Lappe5, Christian Dobel5 and  Eckart Altenmüller2
Eckart Altenmüller2
- 1Clinic of Phoniatrics and Pedaudiology, Muenster University Hospital, Muenster, Germany
- 2Institute of Music Physiology and Musicians‘ Medicine, Hannover University of Music, Drama and Media, Hannover, Germany
- 3Clinic for Neurology, Hannover Medical School, Hannover, Germany
- 4German Center for Neurodegenerative Diseases (DZNE), Bonn, Germany
- 5Institute for Biomagnetism and Biosignalanalysis, University of Muenster, Muenster, Germany
Introduction
Although the amusia field is presently dominated by research into congenital cases (e.g., Ayotte et al., 2002),
there has been a long tradition of investigations into acquired amusia
after stroke or brain damage. We have observed, based on our clinical
experience on a stroke unit, that some patients feel that music sounds
different to how it did before the stroke. For such cases, we were
interested in detecting the characteristics of those deficits as they
relate to perceptual and productive musical functions.
Cortical and subcortical brain lesions may cause impairments to such musical functions (Peretz, 1990; Liegeois-Chauvel et al., 1998; Schuppert et al., 2000). These impairments, which manifest themselves clinically in various patterns of deficits in music processing and production (Kohlmetz et al., 2003; DiPietro et al., 2004),
are collectively referred to as receptive or expressive amusia. The
terms “receptive” and “expressive” are used to represent perceptive and
productive musical ability, respectively.
The cognitive processing of music involves high-order
neural processing, and it has been claimed that an accurate perception
of the melodic and temporal aspects of music requires both “local” and
“global” auditory information processing. The terminology of “local” and
“global” processing was introduced in the seminal paper by Peretz (1990):
In melody perception, the particular interval between two successive
notes is assumed to be processed by local, more analytical strategies,
whereas the perception of the entire melodic contour requires a more
global sense of information processing. The temporal dimension comprises
rhythm perception through local strategies and discrimination of meter
via global processing mechanisms (Peretz, 1990; see also Liegeois-Chauvel et al., 1998). Those findings were confirmed by our own observations (Schuppert et al., 2000);
we detected a more pronounced deficit in local pitch- and rhythm-
related ability following left-sided stroke. Conversely, after a
right-sided stroke, greater deficits were revealed in global melody
contour (use of melodic contextual cues in pitch judgments) and meter
processing. Consequently, for this study we retain the systematic view
of a differentiation between local and global aspects of melodic and
rhythmic processing.
Another key theoretical concept is that of hemispheric
specialization for music processing and expression. Previous studies
have confirmed the idea of a relative specialization of left and right
auditory areas by showing that the left temporal lobe is more involved
in the processing of rhythmic, temporal, and sequential features of
music than right temporal regions. The latter are more engaged in
melodic (pitch and contour) and timbre perception and the perception of
spectral features (Samson and Zatorre, 1994; Zatorre and Belin, 2001; Schonwiesner et al., 2005; Lappe et al., 2013).
The tendency of melodic and rhythmic processing to lateralize to the
left hemisphere in professional musicians has also been demonstrated (Altenmüller, 2001; Russeler et al., 2001; Vuust et al., 2005). Based on the idea of both hemispheres functioning as an intertwined music perception network (Altenmüller, 1989; Schon et al., 2010),
an additional bilateral sensitivity to timing information has also been
suggested, as well as a higher order system in the superior temporal
sulcus, with the processing of slowly modulated signals in the right
hemisphere (Boemio et al., 2005).
In the case of expressive functions, evidence exists for a
differentiation of hemispheric involvement: namely, an asymmetry
favoring right temporal regions in the maintenance of pitch while
singing (Perry et al., 1999) and in the imagery of tunes (Halpern and Zatorre, 1999; Herholz et al., 2008).
In our view, a lesion study provides an excellent
opportunity to clearly associate such receptive and expressive musical
functions. The Montreal Battery of Evaluation of Amusia (MBEA; Peretz et al., 2003)
is a well-established tool to document incidences of amusia. It
contains detailed receptive melodic and metric subtests subdivided into
global and local aspects of music processing. However, when we started
data collection, the first version of the MBEA seemed to be too complex
for use in the clinical routine of a stroke unit. Additionally, the MBEA
does not contain any expressive tests, which we considered valuable in
addressing the lack of information about expressive musical abilities
after a stroke.
In line with the MBEA, one element of the bedside test
battery used in this study was a group of five receptive subtests (Pitch
Test, Melody Interval Test, Melody Contour Test, Rhythm Test, Meter
Test), presented in a previous design to assess melodic and metric music
perception by means of discrimination tasks (Schuppert et al., 2000). Additionally, we generated new versions of expressive rhythmic and melodic tests.
Our study comprises two experiments with separate groups
of subjects. After evaluation of the first experiment, we reorganized
the receptive and expressive tests for a second experimental setting
with some adjustments to better capture the underlying receptive or
expressive mechanisms. For the original Meter Test 1, melody sequences
had to be identified as a “waltz” or a “marching” meter. The idea was to
make it easy to decide whether there was a metric violation or not.
However, after evaluation of the first experiment we changed the test to
a discrimination task requiring “same”/“different” judgments in line
with the other receptive subtests (Figure 1),
because some subjects were unfamiliar with the musical terms of “waltz”
or “marching” meter. The second adjustment concerned the instrument
used for the expressive melody test. For the first version of expressive
melody testing, we used a xylophone because this instrument is used in
early music education at German schools, and it seemed to be appropriate
for the simple reproduction of short melody lines. But again after the
evaluation of the first experiment, we recognized that the use of a
xylophone was much more complex than had been assumed, based on the
statements of our subjects complaining about too complex motoric
interaction. Due to the fact that Germans also receive a vocal education
in school and that good vocal imitation via singing had already been
shown for congenital amusics (Tremblay-Champoux et al., 2010), we decided to change this test to one of vocal reproduction.
FIGURE 1
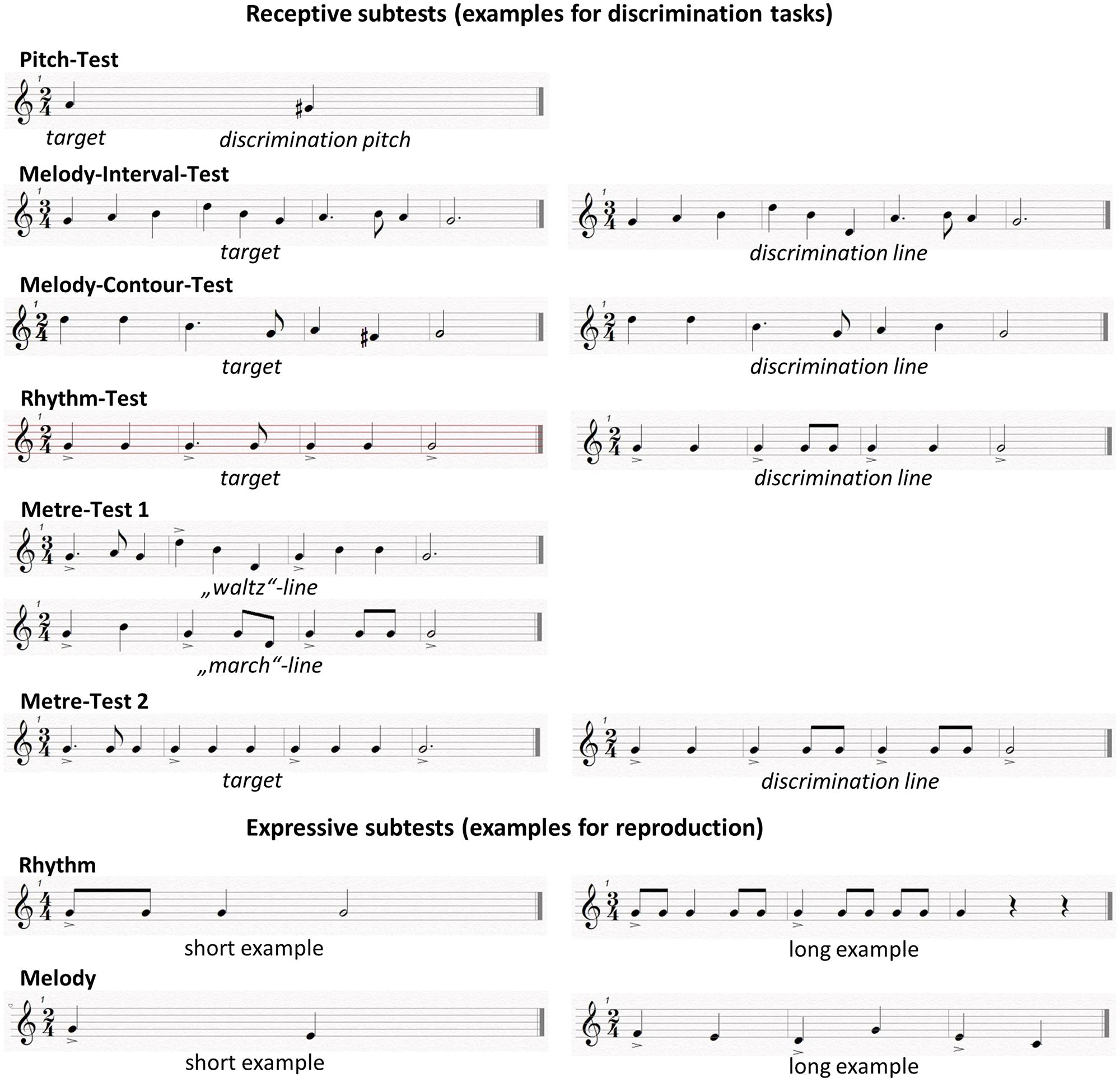 FIGURE 1. Examples of receptive and expressive subtests.
FIGURE 1. Examples of receptive and expressive subtests.
Creating a direct interaction
between the subjects and the investigator was important for the
expressive testing of our study. Recent literature has shown that the
brain’s mirror neuron system is strongly involved in motoric imitation
as well as in vocal imitation, a phenomenon first investigated in song
birds (Prather, 2013)
that learn their melody lines by imitation. On the basis of various
neuroimaging studies, the claim could be made that the intertwined
involvement of receptive and expressive functions, especially during
vocal production, is a sign of a refined learning system of human social
communication (Brown et al., 2004; Ramachandra et al., 2009; Leveque et al., 2013). Recent findings discussed the underlying pathways for vocal and non-vocal perception and production (Loui et al., 2009)
which could be interpreted as a reason for a potentially different
outcome for instrumental versus vocal imitation. Nevertheless, good
results of live vocal interaction during stroke rehabilitation have been
obtained with Melodic Intonation Therapy in which patients actively
reproduce vocally adapted intonation lines to improve language recovery (Norton et al., 2009).
This study was designed as a straightforward assessment
of receptive and especially expressive musical functions that could
feasibly be applied in clinical practice. Our main focus was to compare
the music perception and production abilities of patients directly after
stroke, separately by side of lesion, with those of healthy subjects.
Our tests covered the spectral and temporal domains; some focused on a
more detailed analysis of musical patterns (Pitch Test, Melody Interval
Test, Rhythm Test) and others on a more global music perception ability
(Melody Contour Test, Meter Test), on the basis of previous literature
on acquired amusia.
In line with previous research, we expected stroke
patients to perform significantly worse on receptive and expressive
musical tasks than the controls. Furthermore, we expected that on
comparing the outcome of the different receptive subtests, local versus
global processing would be differentially affected by the side on which
the stroke had been experienced. We anticipated greater reduction in
local musical function in the Melody Interval Test and the Rhythm Test
following a left-sided stroke and a more strongly impaired global
musical function in the Melody Contour Test and the Meter Test following
a right-sided stroke. For both receptive and expressive musical
functions, we hypothesized that musical impairment would depend on the
level of musical education that was gained prior to the stroke.
No comments:
Post a Comment