Hell, wearables have been out there for years, your doctor should have been doing movement assessment for years. But because the board of directors has set incorrect goals for the stroke department, survivors suffer the consequences.
wearable (15 posts to April 2012)
wearable arms (1 post to May 2013)
wearable computing (3 posts to August 2013)
wearable devices (31 posts to October 2015)
Wearable inertial measurement units (1 post to June 2019)
wearable sensors (14 posts to January 2018)
wearable shoe (1 post to December 2019)
sweat-reading hydration wearable (1 post to March 2018)
Automated Movement Assessment in Stroke Rehabilitation
 Tamim Ahmed1*,
Tamim Ahmed1*,  Kowshik Thopalli2*,
Kowshik Thopalli2*,  Thanassis Rikakis1,
Thanassis Rikakis1,  Pavan Turaga2,
Pavan Turaga2,  Aisling Kelliher3,
Aisling Kelliher3,  Jia-Bin Huang4 and
Jia-Bin Huang4 and  Steven L. Wolf5
Steven L. Wolf5- 1Department of Biomedical Engineering, Virginia Tech, Blacksburg, VA, United States
- 2Geometric Media Lab, School of Arts, Media and Engineering, Arizona State University, Tempe, AZ, United States
- 3Department of Computer Science, Virginia Tech, Blacksburg, VA, United States
- 4Department of Electrical and Communication Engineering, Virginia Tech, Blacksburg, VA, United States
- 5Department of Rehabilitation Medicine, Emory University, Atlanta, GA, United States
We are developing a system for long term Semi-Automated Rehabilitation At the Home (SARAH) that relies on low-cost and unobtrusive video-based sensing. We present a cyber-human methodology used by the SARAH system for automated assessment of upper extremity stroke rehabilitation at the home. We propose a hierarchical model for automatically segmenting stroke survivor's movements and generating training task performance assessment scores during rehabilitation. The hierarchical model fuses expert therapist knowledge-based approaches with data-driven techniques. The expert knowledge is more observable in the higher layers of the hierarchy (task and segment) and therefore more accessible to algorithms incorporating high level constraints relating to activity structure (i.e., type and order of segments per task). We utilize an HMM and a Decision Tree model to connect these high level priors to data driven analysis. The lower layers (RGB images and raw kinematics) need to be addressed primarily through data driven techniques. We use a transformer based architecture operating on low-level action features (tracking of individual body joints and objects) and a Multi-Stage Temporal Convolutional Network(MS-TCN) operating on raw RGB images. We develop a sequence combining these complimentary algorithms effectively, thus encoding the information from different layers of the movement hierarchy. Through this combination, we produce a robust segmentation and task assessment results on noisy, variable and limited data, which is characteristic of low cost video capture of rehabilitation at the home. Our proposed approach achieves 85% accuracy in per-frame labeling, 99% accuracy in segment classification and 93% accuracy in task completion assessment. Although the methodology proposed in this paper applies to upper extremity rehabilitation using the SARAH system, it can potentially be used, with minor alterations, to assist automation in many other movement rehabilitation contexts (i.e., lower extremity training for neurological accidents).
1. Introduction
As the US and global populations age, we observe an increasing need for effective and accessible rehabilitation services for survivable debilitating illnesses and injuries, such as stroke and degenerative arthritis (1, 2). Effective rehabilitation requires intensive training and the ability to adapt the training program based on patient progress and therapeutic judgment (3). Intensive and adaptive rehabilitation is challenging to administer in an accessible and affordable way; high intensity therapy necessitates frequent trips to the clinic (usually supported by a caregiver), and significant one-on-one time with rehabilitation experts (4). Adaptation requires a standardized, evidence-based approach, coordinated amongst many specialists (5–7). Active participation by the patient is also critical for improving self-efficacy and program adherence (8), although, without significant dedicated effort from a caregiver, in many cases, active participation and adherence are difficult to achieve (9).
Telemedicine and telehealth are gaining significance as viable approaches for delivering health and wellness at the home and in the community at scale (10). Applying existing telemedicine approaches to physical rehabilitation in the home is not yet possible, owing to the challenges of automating the observation, assessment, and therapy adaptation process used by expert therapists. For upper extremity rehabilitation for stroke survivors, which is the focus of this paper, more than 30 low-level movement features need to be tracked as the patient performs functional tasks in order to precisely and quantitatively characterize movement impairment (5). High precision sensing and tracking systems can work well in spacious and supervised clinical environments, but are currently not yet appropriate for a typical home setting. The use of marker-based tracking systems or complex exoskeletons are simply too expensive, challenging to use, and obtrusive in the home (11–13).
Banks of video camera arrays can seem intrusive in the home and lead patients and/or their families to feel as if they are under surveillance (6). More promisingly, networks of wearable technologies (e.g., IMUs, smart skins, pressure sensors) can provide useful tracking data for overall movement and detailed features, but they can also be hard to put on correctly, irritating to wear for long periods of time, and sometimes require a perceived excessive number of wearables to capture all movement features correctly (14). A final concern with respect to the patient's home environment concerns the physical footprint of any technology introduced into their home. Disturbing the home setting can be understood negatively, which has the knock-on effect of reducing adoption by stroke survivors and/or other family members in the home (15).
That said, accurate, low-cost capture of movement data is only part of the challenge. Automation of assessment is also difficult because the processes used by therapists are largely tacit and not well standardized (16). Clinicians are trained to use validated clinical measures (e.g., Fugl-Meyer, ARAT, and WMFT), utilizing a small range of quantitative scales (0–2, 0–3, and 0–5, respectively) for assessing performance of functional tasks that map to activities of daily life (17, 18). These scales provide standardized rubrics for realizing this assessment and use a uniform activity space with exact measurements for each subcomponent of the space to assist the standardized performance of the tasks. The high-level rating of task performance provided by experts through these measures is difficult to map directly to specific aspects of movement and related detailed kinematics extracted through computational means. Even expert clinicians cannot simultaneously observe all aspects of upper extremity pathological movement or compare such observations to a standardized value. There is considerable evidence showing that individual therapists direct their attention toward different elements and assess them differently when evaluating performance in situ and real-time, or when later rating videos of performance (19–22). The relation of movement quality to function is therefore difficult to ascertain in a standardized quantitative manner (5, 16). This results in approaches for structuring and customizing therapy that are partly based on subjective experience rather than a standardized quantifiable framework (16, 20). In turn, this results in a lack of large-scale data on the structuring and customization of adaptive therapy, and on the effects of customization and adaptation choices on functionality in everyday life (23). Therefore, full scale automation of the real-time functions of the therapist at the home is not yet feasible.
In light of these limitations, we are developing the novel Semi-Automated Rehabilitation At the Home (SARAH) system. The SARAH system comprises two video cameras, a tablet computer, a flexible activity mat, and eight custom-designed 3D printed objects, as shown in Figure 1 below. The objects are designed to support a broad range of perceived affordances (24), meaning they can be gripped, moved, and manipulated in a wide variety of ways (25). Each object is unique in terms of size and color to assist identification of objects by patients, and to enable easier identification and tracking using computer vision methods. The flexible activity mat is screen-printed with high-contrast guidance lines indicating to the patient the four primary activity spaces (near and distal ipsilateral and contralateral) through increasingly colored lines. In addition, four rows of circles on the mat assist the computer vision system with boundary detection between activity space for consistently analyzing patient activities.
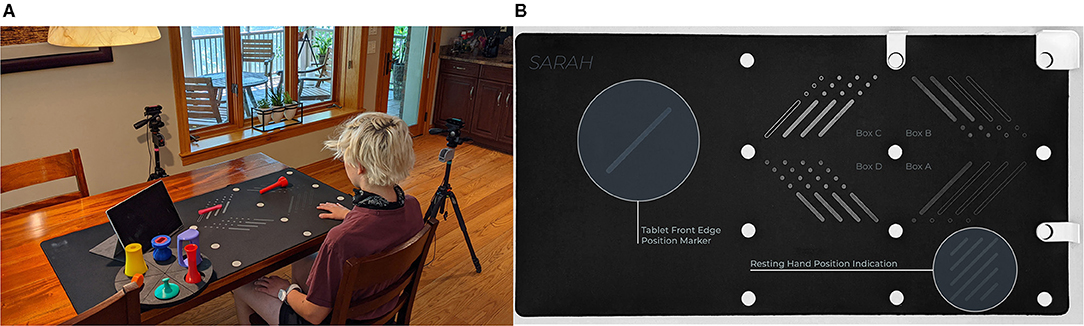
Figure 1. (A) SARAH system and objects setup. (B) SARAH activity mat.
The system can be easily installed on a regular kitchen or living room table. The two cameras initiate and record only during training, and they are activated and controlled by the patient using a custom-designed application on the tablet computer. The system aims to integrate expert knowledge with data driven algorithms to realize coarse real-time automated assessment of movement of stroke survivors during therapy at the home (26). This assessment can drive high-level feedback on results and performance after execution of each training task, to assist patients with self assessment, and to help them plan their next attempt(s) of the training task. Daily summaries of the interactive training will be transmitted to remote therapists to assess overall progress (within and across sessions), adjust the therapy structure, and provide text or audio based feedback and directions to the patient via the tablet. Continuous and effective training monitoring accompanied by feedback on the patient's immediate performance, combined with expert customization of therapy to their needs and learning styles, increases the likelihood of patients adopting home-based rehabilitation systems (8).
The SARAH system is optimized for daily at home therapy of stroke survivors with moderate and moderate-to-mild impairment. Stroke survivors who score above 30 on the Fugl Meyer test and can initiate even minimal movement into extension of the elbow, wrist and digits when discharged from the clinic post stroke, can show significant improvement in function through repetitive training lasting 2 weeks to 6 months (27–29). Currently, third party insurance in the US provides financial support for up to 6 months of outpatient and/or in home therapy after release from the clinic. Patients with moderate impairment and a Mini Mental score >25 can follow instructions given by the SARAH system, use their unimpaired limb to control the SARAH system and can engage (at least partially) all SARAH objects (25). The SARAH system promotes active learning by the patient who is expected to interpret the coarse feedback provided by the system and to plan the next action so as to improve her performance. Furthermore, the generalizable design of the objects and tasks of SARAH encourages the patient to actively map the task to multiple ADLs. These active learning characteristics of the SARAH system, combined with the variety of included tasks in the system makes the system feasible for in-home rehabilitation lasting 2–8 weeks (25, 26).
This paper focuses on our hybrid knowledge-based data-driven approach to automated assessment of human movement in the home. Our approach leverages expert rubrics for standardized rating of overall task performance to inform automated rating of movement performance based on low cost, limited, noisy, and variable kinematic data. The assessment process and outcomes need to be compatible with therapist assessment approaches so as to assist remote therapists in using summaries of the computational assessment when remotely monitoring progress and structuring therapy at the home. Our approach has two components: (i) making the expert raters process as observable as possible; and (ii) leveraging the expert rating process to inform the structuring and improved performance of computational algorithms. In previous publications, we have presented in detail our research and development activities for the first component (26, 30, 31). Inspired by clinical measures for rating rehabilitation movement, we developed the SARAH system to utilize a standardized activity space with eight well defined sub-spaces that are drawn as bounding boxes on the video capture of therapy (see Figure 2). We designed the SARAH training objects to facilitate generalized mapping of training tasks to ADLs for the patients, while also facilitating tracking through low-cost video cameras (25). We used participatory design processes and custom-designed interactive video rating tools to help expert therapists reveal and reflect on their rating process and internalized (tacit) rating schemas (26).
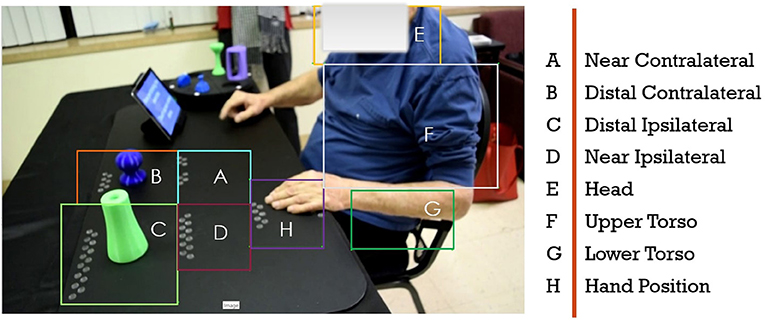
Figure 2. Drawn bounding boxes on the activity space and patients upper body; there are five bounding boxes on the mat and three on the patients body.
In order to manage the complexity of real-time movement observation and to make generalizable observations across different therapy tasks, therapists tend to segment tasks into a few segments that can be combined in different sequences to generate targeted therapy tasks. Even though most therapists use intuitive segmentation of movement for observation and assessment, the segment vocabulary is not standardized. We worked with expert therapists to standardize the segment vocabulary into a state machine that can produce all 15 tasks of the SARAH system (26). The segments are: Initiation + Progression + Termination (IPT), Manipulate and Transport (MTR), Complex Manipulation and Transport (CMTR), and Release and Return (RR). As an example, a drinking related task can be described by the following codification: subject reaches out and grasps a cone object (IPT) and brings it to their mouth (MTR), then returns the object to the original position (MTR), and releases the object and returns the hand to the rest position (RR).
To make the assessment of segments in real-time manageable, the therapist significantly limits the features observed per segment. This limitation is achieved by using their own experience to develop a probabilistic filtering of irrelevant low-level features for a segment (i.e., digit positioning is likely not that relevant to movement initiation), and probabilistic composite observation of relevant features (i.e., a strategy for quick impressions of shoulder and torso compensation during movement initiation). This process is not well standardized as the filtering and compositing activities are based on individual experience and training. We further worked with expert therapists to define a consensus-limited set of composite movement features that are important when assessing the performance of each segment in our model (26). For example, the resulting rubric identifies four key features to assess during the Complex Manipulation and Transport stage: (i) appropriate initial finger positioning, (ii) appropriate finger motion after positioning, (iii) appropriate limb motion following finger positioning, and (iv) limb trajectory with appropriate accuracy. The rubric also establishes operational definitions of terms used to evaluate movement quality and inform rating. For example, the word “appropriate” used in the above instructions is defined as “the range, direction, and timing of the movement component for the task compared to that expected for the less impaired upper extremity.” Although therapists do not explicitly track and assess raw kinematic features, in previous work we proposed computational approaches connecting therapist's assessment of composite features to computationally tracked raw kinematics (5, 32).
No comments:
Post a Comment