But shouldn't your doctor already be using Candesartan on you? Or are they that incompetent that they don't follow and implement research?
Bacause of this piece of the neuronal cascade of death!
glutamate poisoning
generic drug candesartan (brand name: ATACAND®) Blood Pressure Drug Helps Alzheimer's June 2018
This line from there is instructive:
The scientists found that candesartan prevented glutamate-induced neuronal death.
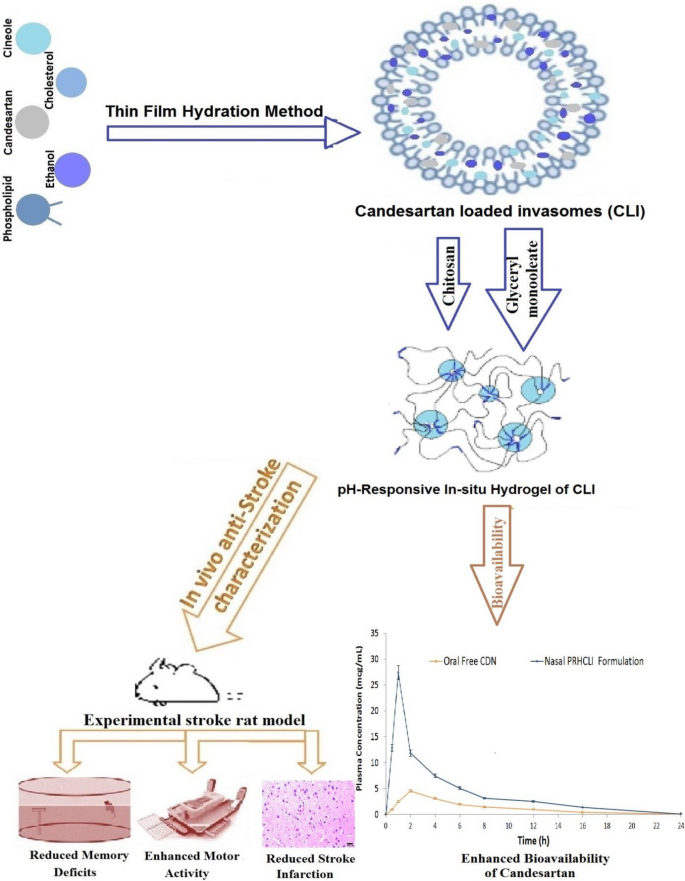
In Vitro and in vivo characterization of nasal pH-Responsive in-situ hydrogel of Candesartan-loaded invasomes as a potential stroke treatment
Abstract
Candesartan (CDN) is a useful anti-stroke medication because it lowers blood pressure, inflammation, oxidative stress, angiogenesis and apoptosis. However, CDN has limited efficacy due to its low solubility and poor bioavailability. This study set out to develop nasal pH-responsive in situ hydrogel of CDN-loaded invasomes a (PRHCLI) for enhancing CDN’s release, penetration, bioavailability, and effectiveness as a possible treatment for stroke. Based on the results of the pre-formulation investigation, the optimum CLI formulation for intravasomal delivery of CDN was determined to be 3% of phospholipid, 0.16% of cholesterol, 3% of ethanol, and 1% of cineole. The optimum formulation significantly enhanced CDN permeation and release by 2.06-fold and 59.06%, respectively. The CLI formulation was added to a mixture of chitosan (0.67%w/v) and glyceryl monooleate (0.27%v/v) to develop PRHCLI. The PRHCLI formulation enhanced the release and permeation of CDN relative to free CDN by 2.15 and 2.76 folds, respectively. An experimental rat stroke model was utilized for in vivo studies to evaluate the bioavailability, effectiveness, and toxicity of the PRHCLI formulation. The nasal PRHCLI drops increased the CDN’s bioavailability by 3.20-fold compared to oral free CDN. Increased grip strength and decreased flexion, spontaneous motor activity, and Morris Water Maze scores in comparison to oral free CDN showed that nasal PRHCLI drops have better anti-stroke activity. The toxicity evaluation revealed the safety of nasal PRHCLI. Hence, nasal PRHCLI drops may represent a promising avenue as a stroke therapy.
Graphical abstract
No comments:
Post a Comment