https://www.medscimonit.com/abstract/index/idArt/907372/act/2
huai Zhang, Min Chen, Lei Gao, Ying Liu
(Department of Radiology, Beijing Hospital, National Center of Gerontology, Beijing, China (mainland))
Med Sci Monit 2018; 24:2841-2848
DOI: 10.12659/MSM.907372
Published: 2018-05-06
BACKGROUND:
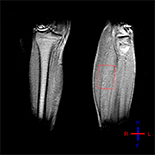
New evidence reveals significant metabolic changes in skeletal muscle after stroke. However, it is unknown if 31P magnetic resonance spectroscopy (31P-MRS) can evaluate these metabolic changes. Our objective here was to investigate: (a) if muscle energy metabolism changes in the affected side; (b) if muscle energy metabolism changes after rehabilitation; and (c) if energy metabolism measured by 31P-MRS can reflect changes in the Modified Modified Ashworth Scale (MMAS) and Fugl-Meyer assessment-lower extremity (FMA-LE) scores after rehabilitation.
MATERIAL AND METHODS:
We enrolled 13 patients with stroke symptoms and hemiplegia. Lower-limb motor status on the affected side was evaluated by FMA-LE and MMAS. The 31P-MRS measures included phosphocreatine (PCr), inorganic phosphate (Pi), PCr/Pi, and pH. We statistically compared these measures in the affected and unaffected lower leg muscles before rehabilitation and after rehabilitation on the affected side. Spearman correlational analyses was performed to determine correlations between change in energy metabolism and change in FMA-LE score and MMAS score after rehabilitation.
RESULTS:
PCr and PCr/Pi were significantly lower in the affected muscle compared to the unaffected muscle; however, there were no significant differences in Pi or pH. After rehabilitation, PCr, Pi, PCr/Pi, and pH did not significantly change. However, FMA-LE and MMAS score improved significantly after rehabilitation. Changes in energy metabolism measured by 31P-MRS had no correlation with FMA-LE change after rehabilitation. However, changes in PCr and PCr/Pi were correlated with change in MMAS score after rehabilitation.
CONCLUSIONS:
31P-MRS can evaluate changes in muscle energy metabolism in patients with stroke. PCr measured by 31P-MRS can reflect changes in MMAS after rehabilitation.
No comments:
Post a Comment