Even with all this previous research NO ONE seems able to write a protocol on this. Incompetency reigns supreme and the result is stroke survivors don't recover. Hope you are ok with that.
- vibrotactile (1)
- vibrotactile feedback (4)
Balance Training With a Vibrotactile Biofeedback System Affects the Dynamical Structure of the Center of Pressure Trajectories in Chronic Stroke Patients
 Kentaro Kodama
Kentaro Kodama Kazuhiro Yasuda
Kazuhiro Yasuda Nikita A. Kuznetsov
Nikita A. Kuznetsov Yuki Hayashi4 and
Yuki Hayashi4 and - 1Department of Economics, Kanagawa University, Yokohama, Japan
- 2Research Institute for Science and Engineering, Waseda University, Tokyo, Japan
- 3School of Kinesiology, Louisiana State University, Baton Rouge, LA, United States
- 4Graduate School of Creative Science and Engineering, Waseda University, Tokyo, Japan
Introduction
Following a stroke, a complex interplay of sensory, motor, and cognitive impairments may interfere with balance (de Haart et al., 2004). Stroke patients commonly show increased postural sway and asymmetric weight distribution while standing (Mansfield et al., 2013; Hendrickson et al., 2014). Impaired balance decreases mobility and increases fall risk in elderly stroke patients (Lamb et al., 2003). Vibrotactile biofeedback (BF) application to the trunk is a promising method for restoring balance ability (e.g., Dozza et al., 2007; Bechly et al., 2013).
However, we previously found that a 4 week vibrotactile BF training did
not induce significant changes on several center of pressure (CoP)
measures (i.e., sway area, path length) in chronic stroke patients (Yasuda et al., 2018).
In this report, we apply detrended fluctuation analysis (DFA; Peng et al., 1994)
to characterize the effects of this BF training in stroke patients. DFA
offers an additional perspective on postural control dynamics in
comparison to traditional CoP metrics because it examines control
processes across multiple time scales (Eke et al., 2002; Seuront, 2009). DFA can evaluate presence of temporal correlations across a range of window sizes (Brown and Liebovitch, 2010). Fractal processes can be categorized in two families: fractional Gaussian noise (fGn) and fractional Brownian motions
(fBm). The scaling exponent, DFA α, is interpreted as an indicator of
temporal correlation pattern: If 0 < α < 1 (fGn) with
anti-persistent (α < 0.5), random (α = 0.5), or persistent dynamics
(α > 0.5). If 1 < α < 2 (fBm) with under-diffusive (a <
1.5), Brownian (α = 1.5), hyper-diffusive dynamics (α > 1.5) (Delignières et al., 2011).
Previous studies have indicated that DFA can identify
differences in postural control strategy between young and elderly
adults (Amoud et al., 2007; Duarte and Sternad, 2008). Roerdink et al. (2006)
applied DFA to CoP data to compare stroke patients with healthy elderly
and showed that the CoP trajectories of both the healthy elderly and
stroke patients exhibited temporally correlated patterns rather than
random noise (Roerdink et al., 2006).
The dynamical structure of CoP during quiet stance is characterized by presence of multiple scaling regions (Minamisawa et al., 2009; Teresa Blázquez et al., 2009; Kuznetsov et al., 2013). Kuznetsov et al. (2013)
reported three scaling regions in a sample of healthy young adults.
Presence of multiple scaling regions may be indicative of intermittent
control strategy (Loram et al., 2011) or continuous open- and closed-loop control strategy (Collins and De Luca, 1995).
The effect of vibrotactile BF on the dynamics across
multiple-scales for postural control remains unknown however. Postural
control strategy used by stroke patients may differ from the strategies
used by younger adults or healthy elderly due to freezing, asymmetrical
weight distribution, and sensory input alterations. We hypothesized that
intensive balance training using vibrotactile BF would affect the
dynamical structure of CoP trajectories in chronic stroke patients.
Materials and Methods
Participants
We recruited 9 participants with chronic hemiparetic
stroke from the Department of Physical Medicine and Rehabilitation,
Tokyo General Hospital (Table 1).
Inclusion criteria were positive history of chronic unilateral ischemic
or hemorrhagic stroke, age 50–80 years, stroke >6 months ago,
completion of conventional therapy, and ability to stand unsupported for
10 min and sense BF system vibrations. Prior to the study, all
participants underwent conventional balance rehabilitation with a
physical therapist twice a week.
TABLE 1
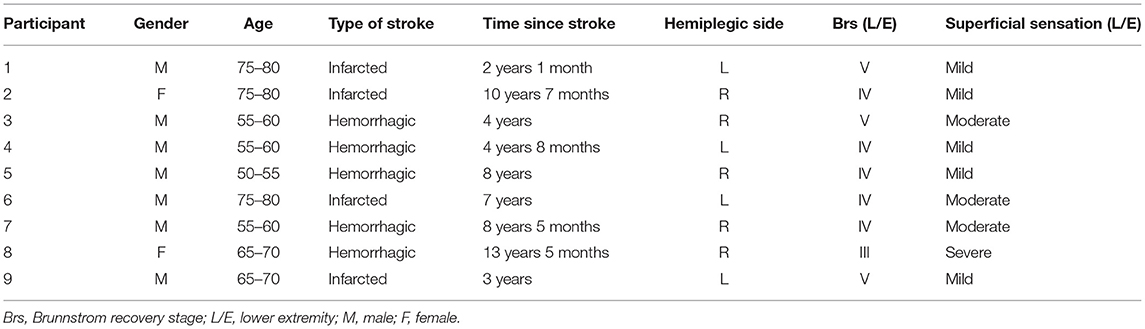 Table 1. Participants' demographic data (n = 9).
Table 1. Participants' demographic data (n = 9).BF System Overview
The vibrotactile BF device consisted of a Nintendo Wii
balance board (Nintendo Co., Ltd., Kyoto, Japan) and a personal computer
with custom software (Visual Studio; Microsoft Corp., Redmond, WA,
USA). CoP position data were measured in both the ML and AP directions
at 50 Hz. The system uses vibration motors attached to the belt at the
level of the pelvic girdle (bilaterally attached at the anterior
superior iliac and posterior superior iliac spine) to convey information
about body sway (Figure 1).
FIGURE 1
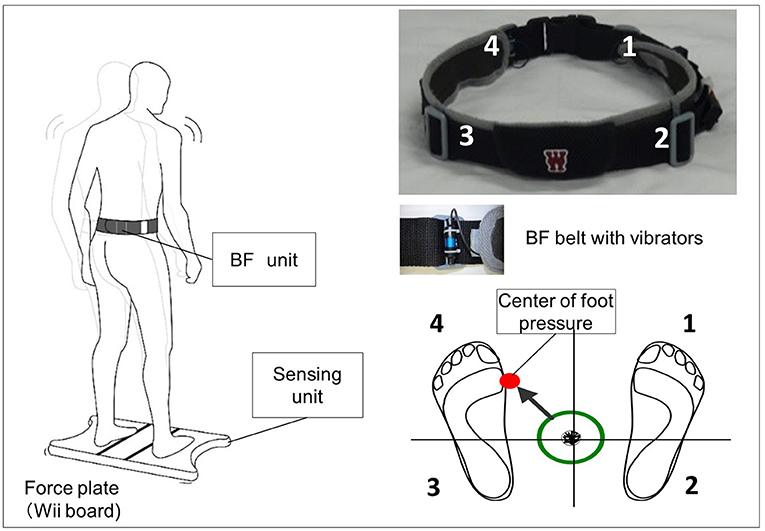 Figure 1. Biofeedback system overview. Vibrators on
the pelvic belts worn by the participants vibrated in the corresponding
direction when the center of pressure (CoP) exceeded the predefined
threshold (e.g., if CoP shifts to the back left, the back left vibrator
is activated).
Figure 1. Biofeedback system overview. Vibrators on
the pelvic belts worn by the participants vibrated in the corresponding
direction when the center of pressure (CoP) exceeded the predefined
threshold (e.g., if CoP shifts to the back left, the back left vibrator
is activated).Protocol and Postural Task
Participants underwent 45 min of BF training 2 times per
week for 2 weeks. The training consisted of two task-oriented balance
training exercises used as part of the conventional rehabilitation (Teasell et al., 2008).
Two balance training exercises were used: (1) standing on
a rubber foam mat (balance mat, Sanwa Kako Co. Ltd, Japan):
participants stood barefoot on the mat with their eyes open and were
instructed to use the BF information to stabilize their postural sway
(i.e., they were instructed to stay within the predefined threshold area
using BF information) and (2) weight-shifting to the paralyzed limb:
participants were instructed to move their paralyzed lower limb forward
and then put their weight on that limb. While doing so, participants
used the BF information to help maintain a stable standing position.
Each training session comprised 10 repetitions of the balance task (1
min per repetition, 10 min total) with a short interval between
repetitions. The BF threshold setting was reset on each day of training
before implementing tasks (1) and (2). We determined the circular
threshold as a 95% confidence circle area (Yasuda et al., 2017)
during the 30 s stance. Target area was defined as 90% of the
pre-measured 95% confidence circle area. The BF vibrators were activated
when the CoP exceeded this threshold (Yasuda et al., 2017).
More at link.
No comments:
Post a Comment