Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 33,614 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke. DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
Wednesday, April 10, 2019
Concepts for brain aging: resistance, resilience, reserve, and compensation
You will need this with your likely chance of getting dementia after your stroke. What is your doctor doing to prevent that? I probably used up all my brain reserve just surviving my stroke.
A
primary goal of research in cognitive impairment and dementia is to
understand how some individuals retain sufficient cognitive function for
a fulfilling life while many others are robbed of their independence,
sometimes their essence, in the last years and decades of life. In this
commentary, we propose operational definitions of the types of factors
that may help individuals retain cognitive function with aging. We
propose operational definitions of resistance, resilience, reserve,
with an eye toward how these may be measured and interpreted, and how
they may enable research aimed at prevention. With operational
definitions and quantification of resistance, resilience, and reserve, a
focused analytic search for their determinants and correlates can be
undertaken. This approach, essentially a search to identify protective
risk factors and their mechanisms, represents a relatively unexplored
pathway toward the identification of candidate preventive interventions.
A
primary goal of research in cognitive impairment and dementia is to
understand how some individuals retain sufficient cognitive function for
a fulfilling life while many others are robbed of their independence,
sometimes their essence, in the last years and decades of life. Here, we
propose to define key concepts for which there is not yet a consensus.
At the outset, we recognize that our focus is biological (molecules,
cells, systems, organism), appreciate the major impact of environmental
and social determinants of health and admit our prejudice that
environmental and social factors ultimately impact cognition through
biological processes.
It
seems likely that a host of diverse factors active during fetal
development, childhood, and throughout adult life may initiate,
aggravate, or protect against relevant pathophysiologic processes that
underlie neurodegeneration and its clinical expression. These
factors—some adverse and some protective—may operate independently,
synergistically, antagonistically, sequentially, or even differentially
(Fig. 1).
While some may be examined individually and in exquisite molecular
detail in animal or in vitro models, most will require careful,
longitudinal validation in humans. From this perspective, it is not
surprising that so far we have had only limited success in identifying
risk factors and their underlying mechanisms to guide effective primary
and secondary preventive interventions.
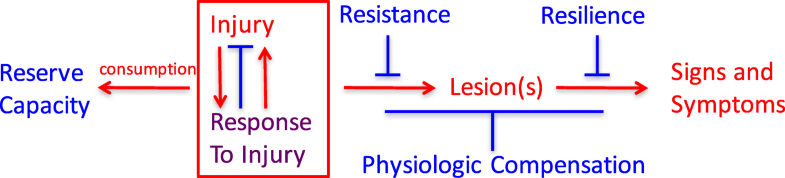
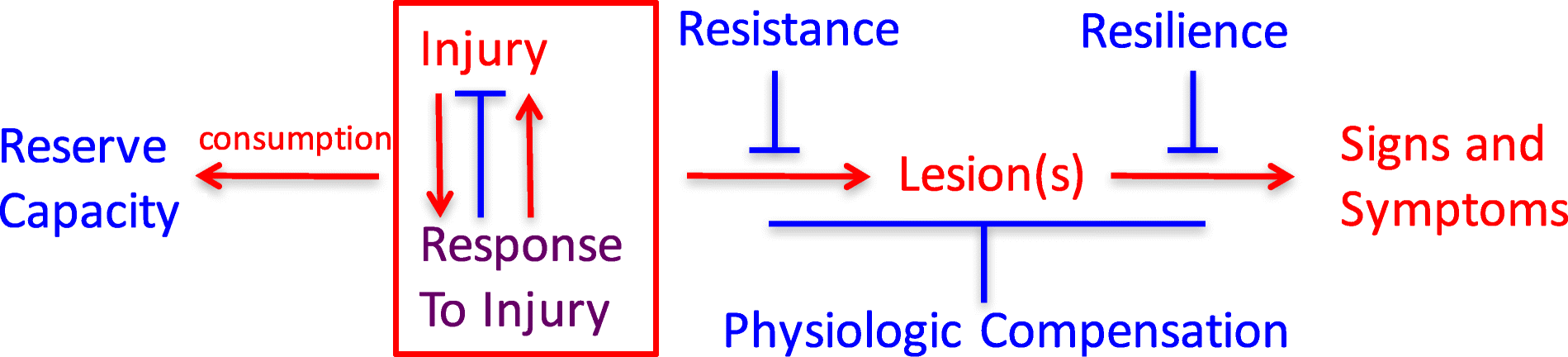
Fig. 1
Relationships among
adverse (red), protective (blue), and mixed (purple) processes that
culminate in signs and symptoms of neurodegenerative diseases
Until
quite recently, “late onset Alzheimer’s disease” was widely viewed as a
specific disease entity responsible for the vast majority of late-life
dementia. However, longitudinal epidemiologic studies of brain aging and
cognitive decline with brain autopsy have consistently demonstrated a
central role for multiple co-morbidities as the dominant determinants of
late-life dementia. It is important to recognize that current intra
vitam measures of these several common diseases of the aging brain are
limited, and consequently, despite limitations, brain histopathologic
evaluation remains the only means to assess comprehensively the impact
of co-morbid diseases on cognitive performance during life.
In
combination with functional assessments obtained during life,
histopathologic features (lesions) determined with brain autopsy define
the presence of specific clinico-pathologic entities, which may or may
not reliably correspond to specific mechanism(s) of disease. As a result
of the highly consistent findings from longitudinal epidemiologic
studies with brain autopsy from across the globe, the view of cognitive
decline and dementia in older adults is shifting from being the result
of a single disease to a conspiracy of multiple, common age-related
disease processes that combine idiosyncratically in each individual. The
most common is Alzheimer’s disease, defined by amyloid beta
accumulation and neurofibrillary degeneration in certain regions of the
brain. Four other commonly recognized pathophysiologic processes that
can contribute to cognitive decline and dementia in late life include
Lewy body disease, vascular brain injury (especially from small vessel
disease), hippocampal sclerosis, and generalized atrophy beyond what can
be explained by these other diseases. While the brain lesions of AD are
more prevalent at autopsy than any of the other lesions, the combined
frequencies of the non-AD abnormalities are usually greater. Indeed, in
both the Nun Study and the Honolulu Asia Aging Study, > 90% of
participants with severe cognitive impairment can be fully attributed to
the collective or individual influences of these five abnormalities [1].
It is critically important, but infrequently appreciated, that the
exponential influence of co-morbid disease is reflected in the
multiplication of individual relative risks (or odds ratios) for each
disease related to cognitive impairment or dementia (Table 1).
Table 1
Point estimates of
odds ratios (OR) from ordinal logistic regression of the impact of the
coprevalence of five brain lesions on cognitive performance within
2 years of death
Lesion co-morbidity index
OR for the Nun Study (n = 334)
OR for the Honolulu Asia Aging Study (n = 774)
0
1.0 (reference)
1.0 (reference)
0.4–0.8
2.8
2.4
1.0–1.8
5.0
4.6
2.0–2.4
23.1
16.3
2.6–4.4
99.1
37.6
Severity of each of
the five brain lesions (Braak stage for neurofibrillary degeneration,
cerebral cortical Lewy body disease, cerebral cortical microinfarcts,
hippocampal sclerosis, low brain weight) was scored as none/mild (0),
moderate (0.4), or severe (1.0) by established criteria, and the lesion
co-morbidity index was calculated as the sum of scores for each of the
five lesions [1]
To
frame a discussion of resistance, resilience, reserve, and
compensation, we conventionally consider the diseases that cause
late-life cognitive impairment and dementia to derive from injury and
response to injury that begin before there are signs or symptoms, but
that the resulting damage, distortion, disruption, and/or degeneration
ultimately becomes overwhelmingly evident as impairments of cognitive
and behavioral function.
The
recognition of risk factors linked to measures of different types and
amount of brain lesions may illuminate fundamental mechanisms and
primary instigating exposures. A systematic search to identify specific
protective factors and the mechanisms that underlie them has been
conducted relatively infrequently. We propose the following operational
definitions as a step toward systematically investigating each of these
processes in individuals:
Resistance
is inferred from an observed absence or lower level of
dementia-associated brain injury, relative to an expected greater
frequency or severity based on age, genetic factors, or other
characteristics of the individual. This state of unexpectedly low or
absent brain injury theoretically may be intrinsic, meaning in someone with greater defenses to forces that usually lead to brain lesions, or environmental,
meaning in someone with usual defenses but who avoided exposure to
these forces. While resistance now can be assessed comprehensively only
with neuropathologic evaluation, specific facets (e.g., beta amyloid,
pathologic tau burden, neuron damage) can be estimated during life with
biomarkers and imaging.
Resilience
is inferred from an observed level of cognitive functioning higher than
expected in the face of demonstrated brain injury. Resilience only can
be recognized or measured when injury exists and can be related to
(near) coincident assessment of function. We prefer to consider two
forms of resilience: apparent and essential. Apparent resilience
refers to a specific lesion type without consideration of common
co-morbidities. Consider two individuals who both are positive by PET
imaging for fibrillar amyloid and pathologic tau; one is cognitively
normal and the other has dementia. The first person has apparent
resilience to AD neuropathologic change. Imagine further a future state
when there also is a PET ligand for pathologic alpha-synuclein. Now, we
learn that the first person lacks Lewy body disease and the second has
co-morbid neocortical Lewy body disease. Is the difference between these
two individuals explained by resilience to AD neuropathologic change or
by resistance to Lewy body in the first person? Once comprehensive
assessment of brain lesions associated with dementia is achieved, then essential resilience
can be evaluated. Currently, this is accomplished best with
neuropathologic assessment, but even this approach is limited. Our brain
autopsy data suggest that much, and perhaps most, of what is referred
to currently as (apparent) resilience actually is resistance to
co-morbid disease.
Consumption or retention of reserve
can be measured or inferred either as brain structural and/or
physiological pre-morbid capacity. Examples might be greater than usual
synaptic density (analogous to computational “hardware”) or enhanced
cognitive effectiveness or redundancy because of learned language,
educational richness, or occupational complexity (analogous to
computational “software”) prior to the onset of disease. The salutary
influence of such resources may be apparent in cognitive test
performance well before the onset of cognitive decline. This definition
requires that measures of reserve capacity must have been estimated or
inferred prior to the development of brain injury. Mechanisms underlying
physiologic compensation
also may be changes in “hardware” or “software,” but in distinction to
pre-existing reserve capacity, physiologic compensation occurs following
injury rather than developing prior to injury/response to injury. An
example of physiologic compensation might be recruitment of additional
regions of the brain to subserve memory function following damage to the
hippocampus or in recovery of language functioning after an infarction
or brain injury.
With
operational definitions of resistance, resilience, and reserve, a
focused analytic search for their predictors and correlates can be
undertaken. This will require distinguishing and measuring each
independently, and then employing those measures as distinct endpoints
to identify their individual determinants. This approach, essentially a
search to identify protective risk factors and their mechanisms,
represents a relatively unexplored pathway toward the identification of
candidate preventive interventions.
No comments:
Post a Comment