Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 33,532 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke. DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
Tuesday, June 30, 2020
Indirect measurement of anterior-posterior ground reaction forces using a minimal set of wearable inertial sensors: from healthy to hemiparetic walking
I got absolutely nothing out of this. NO SOLUTION to the gait problems of stroke survivors, so useless.
The
anterior-posterior a (AP-GRF) and propulsion and
braking point metrics derived from the AP-GRF time series are indicators
of locomotor function across healthy and neurological diagnostic
groups. In this paper, we describe the use of a minimal set of wearable
inertial measurement units (IMUs) to indirectly measure the AP-GRFs
generated during healthy and hemiparetic walking.
Methods
Ten
healthy individuals and five individuals with chronic post-stroke
hemiparesis completed a 6-minute walk test over a walking track
instrumented with six forceplates while wearing three IMUs securely
attached to the pelvis, thigh, and shank. Subject-specific models driven
by IMU-measured thigh and shank angles and an estimate of body
acceleration provided by the pelvis IMU were used to generate indirect
estimates of the AP-GRF time series. Propulsion and braking point
metrics (i.e., peaks, peak timings, and impulses) were extracted from
the IMU-generated time series. Peaks and impulses were expressed as %
bodyweight (%bw) and peak timing was expressed as % stance phase (%sp). A
75%-25% split of 6-minute walk test data was used to train and validate
the models. Indirect estimates of the AP-GRF time series and point
metrics were compared to direct measurements made by the forceplates.
Results
Indirect
measurements of the AP-GRF time series approximated the direct
measurements made by force plates, with low error and high consistency in
both the healthy (RMSE= 4.5%bw; R2= 0.93) and post-stroke (RMSE= 2.64%bw; R2=
0.90) cohorts. In the healthy cohort, the average errors between
indirect and direct measurements of the peak propulsion magnitude, peak
propulsion timing, and propulsion impulse point estimates were 2.37%bw,
0.67%sp, and 0.43%bw. In the post-stroke cohort, the average errors for
these point estimates were 1.07%bw, 1.27%sp, and 0.31%bw. Average errors
for the braking estimates were higher, but comparable.
Conclusions
Accurate
estimates of AP-GRF metrics can be generated using three strategically
mounted IMUs and subject-specific calibrations. This study advances the
development of point-of-care diagnostic systems that can catalyze the
routine assessment and management of propulsion and braking locomotor
deficits during rehabilitation.
The neuromechanical processes underlying healthy bipedal locomotion are multi-factorial [1–3] and converge on locomotor patterns that are characteristically fast, efficient, and stable [1, 4]. An impaired ability to transition from step to step is a locomotor deficit common across diagnostic groups [5–13].
During the step-to-step transition of each gait cycle, a braking force
is generated by the leading limb as it makes contact with the ground in
front of the body. To efficiently accelerate the body into the next
step, coordination of the timing and magnitude of the forward propulsion
force generated by the trailing limb is required [1, 14–16].
Moreover, to walk faster, healthy individuals symmetrically increase
the magnitude of propulsion generated by each limb while maintaining the
relative timing of the propulsion peak [15, 17, 18]. In individuals with impaired propulsion function, walking is often slow, metabolically expensive, and unstable [19–22].
Laboratory
equipment such as instrumented treadmills and forceplates are the gold
standard in characterizing propulsion and braking function during
healthy [23, 24] and impaired [5, 6, 9, 10, 20, 25–27]
walking by way of direct measurements of the anterior-posterior ground
reaction forces (AP-GRFs) generated during walking and point metrics
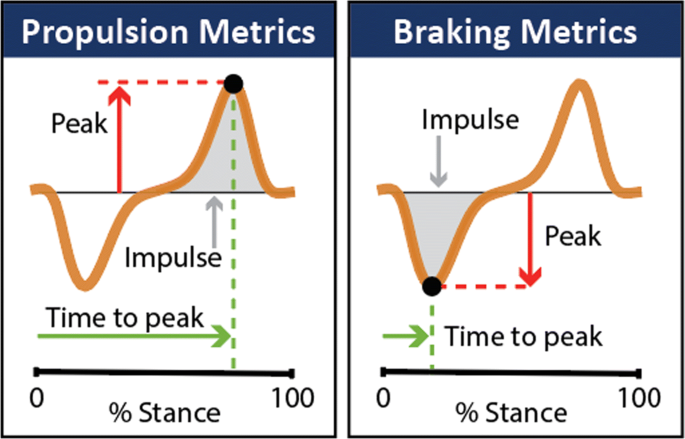
extracted from the AP-GRF time series (Fig. 1).
For example, older adults are reported to generate up to 22% less peak
propulsion (i.e., the peak of the anterior ground reaction force)
compared to young adults [23, 24], and in people post-stroke, the propulsion generated by the paretic limb is up to 68% less than the non-paretic limb [9, 20, 26, 27].
Studies that have combined AP-GRF measurements with clinical
evaluations have shown the clinical consequences of impaired propulsion
function. Indeed, asymmetry in the propulsion impulses generated by the
paretic and non-paretic limbs is correlated with hemiparetic severity [9, 28]. Moreover, deficits in propulsion function are highly related to walking speed [29] and long distance walking [30] after stroke—key determinants of community participation and perceived quality of life [19, 31, 32].
Fig. 1
Anterior-posterior ground reaction force (AP-GRF) time series and salient propulsion and braking metrics
Despite
the importance of propulsion to a functional bipedal gait, conventional
rehabilitation efforts have, by and large, been unable to restore
propulsion function after neurological injury or dysfunction. The
development and study of interventions that target propulsion function
is a highly active area of research [12, 33–41];
however, the clinical translation of these experimental approaches is
hindered by the limited access that rehabilitation clinicians have to
the sophisticated instrumentation (i.e., forceplates and instrumented
treadmills) and personnel with advanced training required to collect,
analyze, and interpret ground reaction force data. Moreover, even in
settings with access to a motion analysis laboratory, locomotor
differences inherent to treadmill walking and the small collection
footprint of most overground forceplate walkways limit ecological
validity. Together, these limitations of the current state-of-the-art
motivate the development of point-of-care propulsion diagnostic systems.
The clinical management of locomotor propulsion deficits will remain
untenable if the measurement instruments used to assess limb propulsion
remain inaccessible.
Wearable
sensors are a promising solution for this measurement gap. Indeed,
wearable sensors have been used to extend gait measurements outside of
the laboratory [42–47]
and a wide range of methods and sensors have proven effective in
providing indirect measurements of the ground reaction forces generated
during walking [48–51].
These methods, however, have largely not been effective for the AP-GRFs
and depend on assumptions of healthy, consistent walking patterns that
may not translate to impaired locomotor patterns [51, 52]. Recent work has shown that inertial measurement units (IMUs) can be used to make measurements during healthy [44] and hemiparetic walking [53]
that are highly correlated to key features of propulsion. The aims of
this study were to extend this work by describing the use of a minimal
set of IMUs to indirectly measure the AP-GRF generated during healthy
and hemiparetic walking and provide estimates of: (i) the AP-GRF time
series and (ii) salient propulsion and braking point metrics (i.e., peak
magnitudes, peak timings, and impulses) extracted from the time series
(see Fig. 1).
No comments:
Post a Comment