But is it better than these other walking assist robots/exoskeletons?
But if you are not walking without the robotic help then you didn't get a successful outcome.
Ask your doctor how this compares to all the other walking assist devices out there.
walking (567)
walking aids (1)
walking assist (6)
walking bike (1)
walking capacity (1)
walking endurance (1)
walking frame (1)
Walking o’Clock (1)
walking pace (3)
walking pattern (1)
walking resistance (1)
walking speed (7)
EksoGT exoskeleton (1 post to September 2017)
Gravity Balancing Exoskeleton (1 post to May 2020)
hip exoskeleton/ (5 posts to May 2020)
kickstart (6 posts to April 2015)
LOPES Exoskeleton (2 posts to October 2020)
HAL (5 posts to April 2019) Hybrid Assistive Limb
The latest here:
Mobile Robotic Balance Assistant (MRBA): a gait assistive and fall intervention robot for daily living
Journal of NeuroEngineering and Rehabilitation volume 20, Article number: 29 (2023)
Abstract
Background
Aging degrades the balance and locomotion ability due to frailty and pathological conditions. This demands balance rehabilitation and assistive technologies that help the affected population to regain mobility, independence, and improve their quality of life. While many overground gait rehabilitation and assistive robots exist in the market, none are designed to be used at home or in community settings.
Methods
A device named Mobile Robotic Balance Assistant (MRBA) is developed to address this problem. MRBA is a hybrid of a gait assistive robot and a powered wheelchair. When the user is walking around performing activities of daily living, the robot follows the person and provides support at the pelvic area in case of loss of balance. It can also be transformed into a wheelchair if the user wants to sit down or commute. To achieve instability detection, sensory data from the robot are compared with a predefined threshold; a fall is identified if the value exceeds the threshold. The experiments involve both healthy young subjects and an individual with spinal cord injury (SCI). Spatial Parametric Mapping is used to assess the effect of the robot on lower limb joint kinematics during walking. The instability detection algorithm is evaluated by calculating the sensitivity and specificity in identifying normal walking and simulated falls.
Results
When walking with MRBA, the healthy subjects have a lower speed, smaller step length and longer step time. The SCI subject experiences similar changes as well as a decrease in step width that indicates better stability. Both groups of subjects have reduced joint range of motion. By comparing the force sensor measurement with a calibrated threshold, the instability detection algorithm can identify more than 93% of self-induced falls with a false alarm rate of 0%.
Conclusions
While there is still room for improvement in the robot compliance and the instability identification, the study demonstrates the first step in bringing gait assistive technologies into homes. We hope that the robot can encourage the balance-impaired population to engage in more activities of daily living to improve their quality of life. Future research includes recruiting more subjects with balance difficulty to further refine the device functionalities.
Background
Physiologic aging processes, musculoskeletal limitations and neuropathology are common causes of impaired balance. Balance control probably has the greatest impact on activities of daily living (ADLs) independence and gait, because it is a fundamental motor skill and prerequisite to the maintenance of a myriad of postures and mobility [1,2,3]. A consequence of weakened balance control is fall. Patient falls have been a major issue of concern in geriatric care and rehabilitation worldwide as it is the single most crucial factor in patient injuries [4]. Falls also have psychological impacts in which they cause fear, anxiety, and loss of confidence, resulting in activity avoidance, social isolation and increasing frailty [5]. The occurrence rate of falls among older patients is high in both healthcare facilities and at home.
The idea of an overground gait or balance trainer has been explored by the rehabilitation and assistive robotics community in the past decade, most notably is the KineAssist [6] developed at Northwestern University and commercialized by Kinea Design LLC. A similar technology focusing on Parkinson’s Disease patients, the Robotic Walker for Gait Rehabilitation, has been reported by Mun et al. [7] from National University of Singapore (NUS). Because of the inertia of the robots, the users of both systems experience an alteration in gait strategies, especially in the stages of transiting between standing and walking (i.e. starting and stopping). On the other hand, some products were developed based on a suspended harness system to provide body weight support for overground mobility training [8]. Most devices currently available were designed to be used in healthcare institutions, rather than home- or community-based, thus having a large footprint and low maneuverability.
A device named Mobile Robotic Balance Assistant (MRBA) was thus developed to address this problem (Fig. 1). The robot provides body weight and balance support to the user during level ground ambulation through its pelvic interface that allows MRBA to track its user autonomously. MRBA follows the user closely while holding onto their pelvis, mimicking the helping hands of a parent when a toddler learns to walk. In case the user loses balance, the robot can intervene the fall by securing the user in place so that they can regain balance. When the user wants to sit down or commute, the robot can be transformed into a powered wheelchair. The motion between sitting and standing are physically supported by the robot. The hybrid design of a gait assistive technology and a wheelchair potentially allows the user to perform a wide variety of ADLs at home and in the community with only one piece of mobility aid.
While the robot is designed for home use, it can also be used in clinical settings to relieve the burden of physiotherapists. It may also help in rehabilitation as it encourages the user to engage in walking and ADLs by providing added safety features. Such home- and community-based rehabilitation is a complement to hospital-based rehabilitation and may promote better recovery in motor capability as it increases the training dose by allowing patient to practice more walking and balancing tasks. Nevertheless, as patients’ mobility and independence are encouraged in the paradigm, the risk of falls is further increased [9,10,11,12]. Notwithstanding, having a device like MRBA ensuring the safety of the user allows the user to participate in a more active lifestyle.
Fig. 1 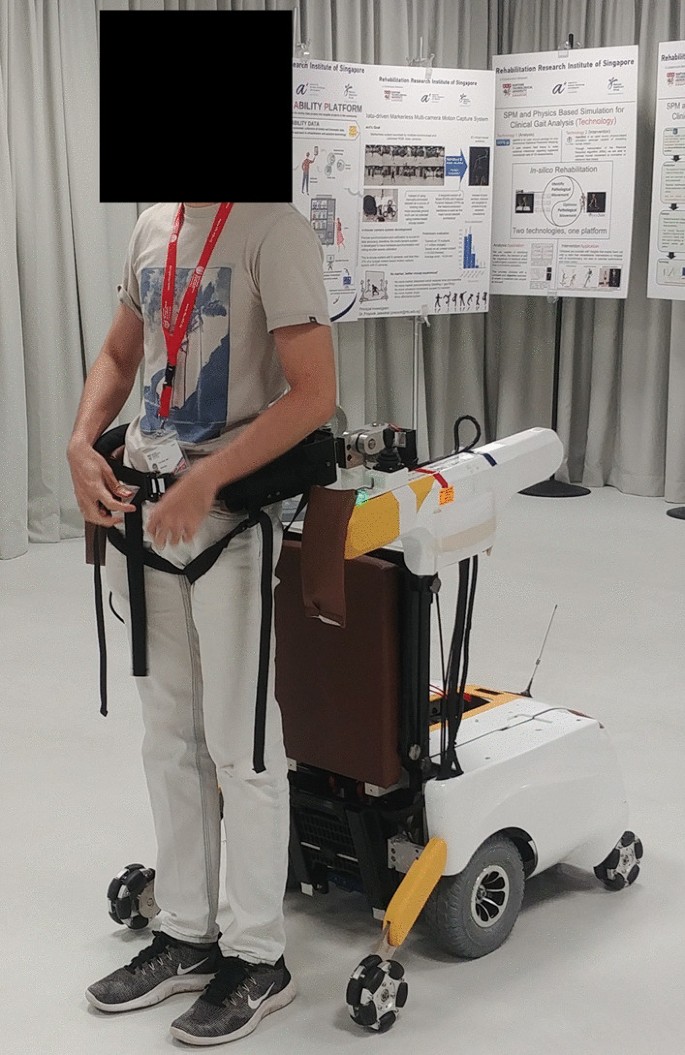
Mobile Robotic Balance Assistant (MRBA) with a user attached to it
Methods
No comments:
Post a Comment