Two comments on this.
Your doctor has had years to evaluate other walking assist devices. Which was best?
walking assist (10 posts to May 2016)
Who still uses NDT(Bobath) in stroke rehab when it should have been shitcanned since 2003? Physiotherapy Based on the Bobath Concept for Adults with Post-Stroke Hemiplegia: A Review of Effectiveness Studies 2003
Control Design for a Power-Assisted Mobile Trainer: Applied to Clinical Stroke Rehabilitation
2 and 2

1
Department of Mechanical Engineering, National Taiwan University, Taipei 106, Taiwan
2
Department of Physical Medicine and Rehabilitation, Cheng Hsin General Hospital, Taipei 112, Taiwan
3
Department of Physiology and Biophysics, National Defense Medical Center, Taipei 114, Taiwan
*
Author to whom correspondence should be addressed.
Machines 2024, 12(1), 61; https://doi.org/10.3390/machines12010061
Submission received: 18 December 2023
/
Revised: 10 January 2024
/
Accepted: 11 January 2024
/
Published: 15 January 2024
(This article belongs to the Special Issue Design and Control of Electrical Machines II)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
This paper presents control design and
implementation for a power-assisted mobile trainer that employs
neuro-developmental treatment (NDT) principles. NDT is a gait
rehabilitation technique for stroke patients that provides minimum
intervention at critical gait events. Traditional NDT rehabilitation is
an effective(NO IT'S NOT! DON'T YOU READ RESEARCH?) post-stroke treatment but is also time consuming and labor
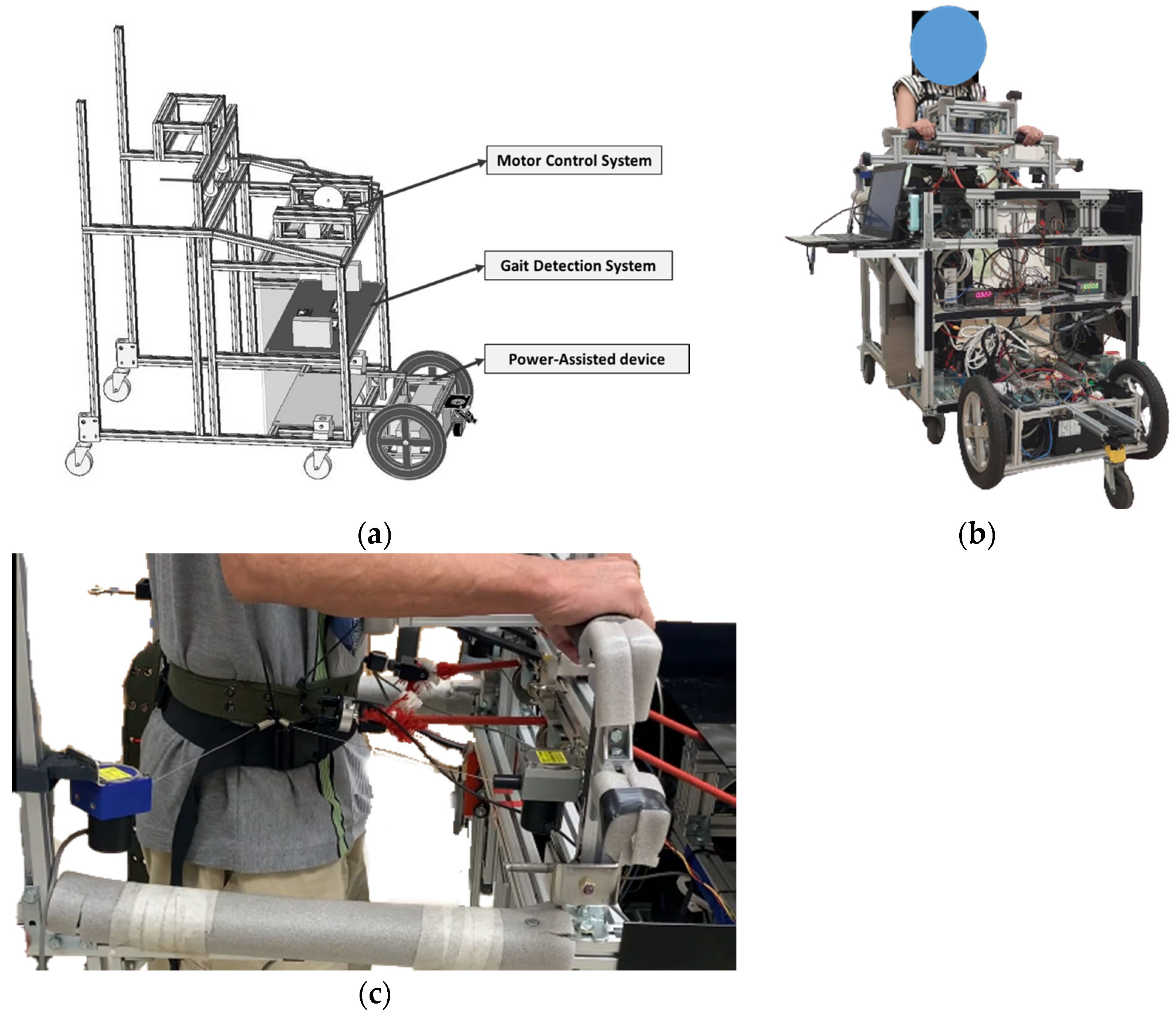
intensive for therapists. Therefore, we designed a mobile NDT trainer to
automatically repeat therapists’ intervention patterns, allowing
patients to receive sufficient training without increasing therapists’
workloads. Because the trainer was self-propelled, it could cause
burdens to stroke patients with limited muscle strength, thereby
potentially degrading the rehabilitation effects. Hence, this paper
proposes a power-assisted device that can let the mobile trainer follow
the user, allowing the subject to focus on the rehabilitation training.
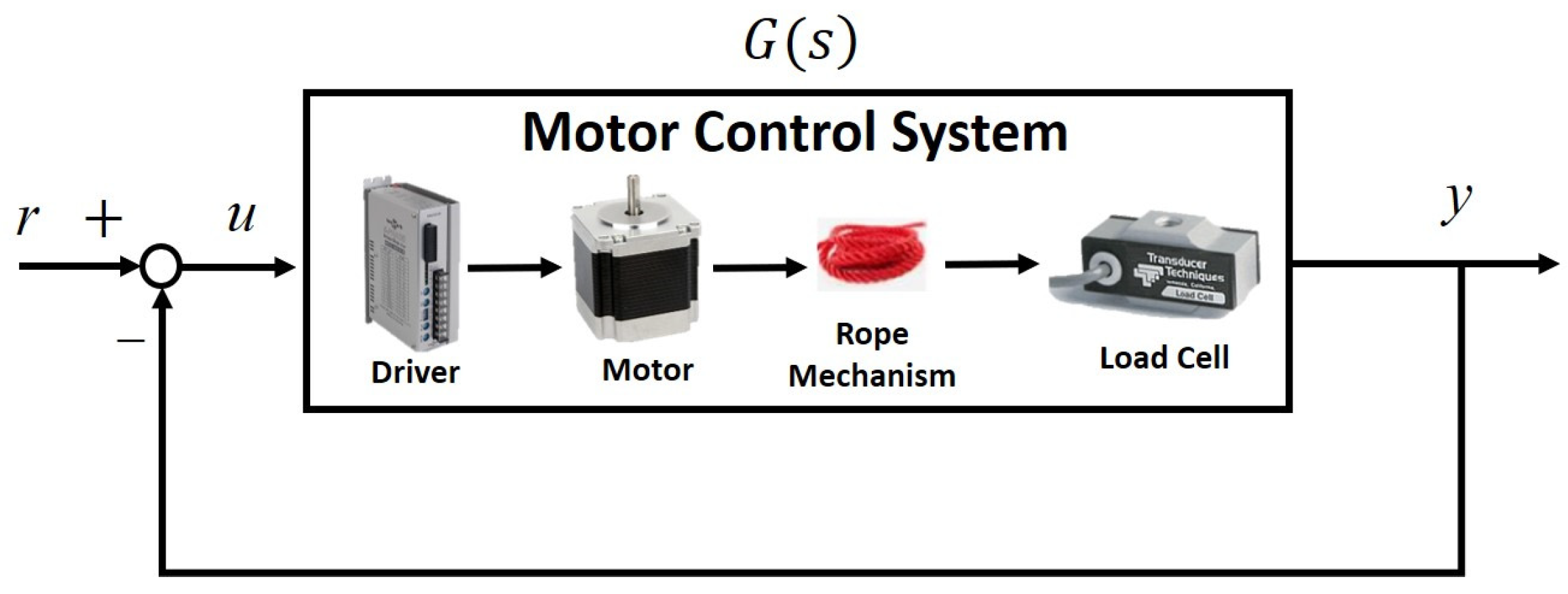
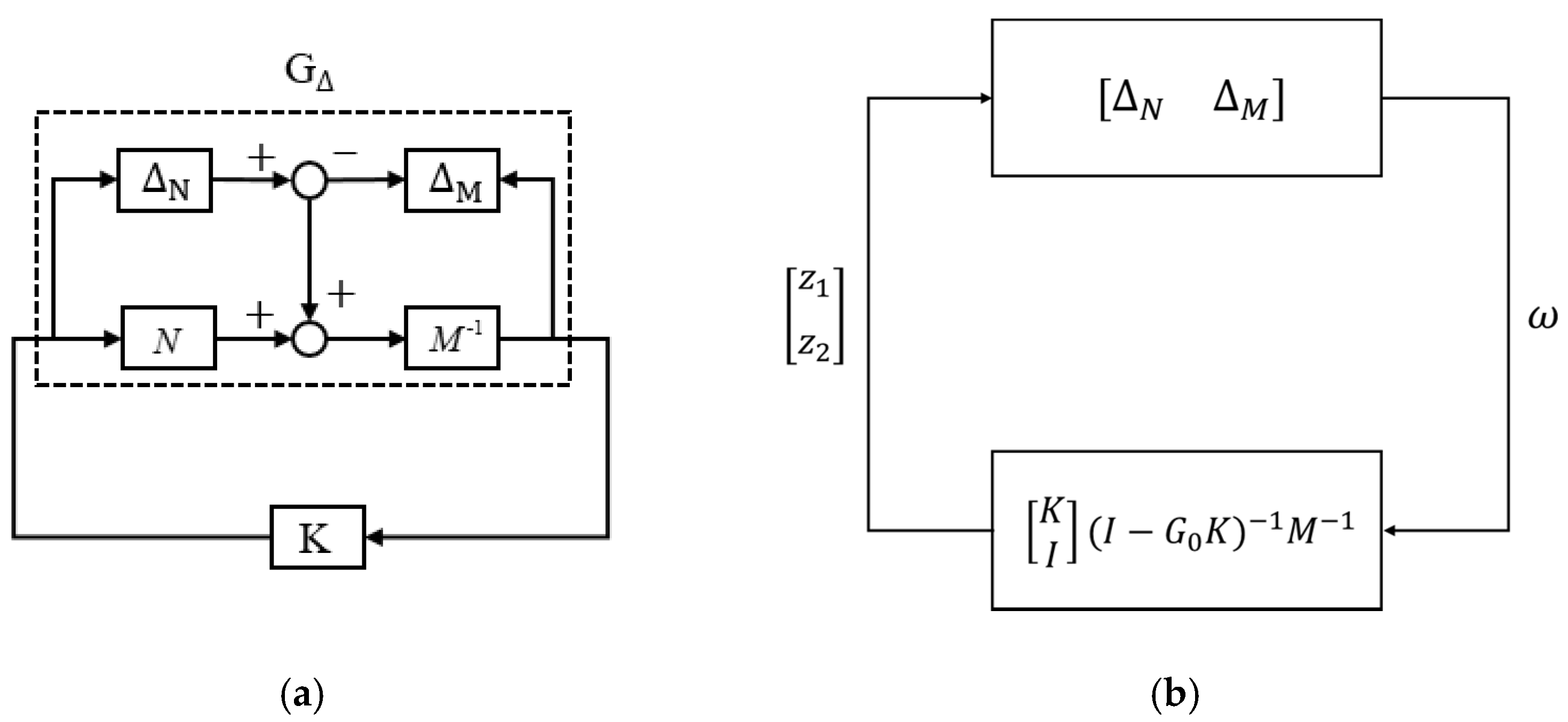
We conducted system identification and control design for the
power-assisted NDT trainer. We then implemented the designed controllers
and tested the trainer. Finally, we invited 10 healthy subjects and 12
stroke patients to conduct clinical experiments. After using the
power-assisted NDT trainer, most participants exhibited improvements in
swing-phase symmetry, pelvic rotation, and walking speed. Based on the
results, the power-assisted device was deemed effective in facilitating
stroke rehabilitation.
1. Introduction
Stroke is the second leading cause of death globally [1].
Even those who survive a stroke can still experience various
after-effects, such as balance issues, difficulties in walking,
cognitive impairments, visual problems, language difficulties, and
fatigue [2]. Because approximately half of post-stroke patients cannot walk [3],
regaining independent walking is the primary goal for post-stroke
rehabilitation as one’s walking ability can significantly affect their
daily activities and life.
Many rehabilitation
devices have been proposed to assist stroke patients in recovering their
walking abilities. For example, Banala et al. [4]
developed lower-limb exoskeletons to improve patients’ gait patterns
and walking speeds for rehabilitation on treadmills. Pietrusinski et al.
[5]
developed a robotic gait rehabilitation trainer that provided practical
guidance on pelvic tilt angles for stroke patients to improve their
walking ability. Werner et al. [6] designed an electromechanical gait trainer to provide non-ambulatory subjects with repetitive practice of gait-like movements.
Another therapeutic approach for treating post-stroke sequelae is neuro-developmental treatment (NDT) [7,8,9],
which is a way to let patients have the feeling of walking with minimal
intervention. The essence of NDT is to rectify sensory perception and
re-educate the processes of posture and motor functions for daily
activities. Patients can intentionally impel their center of gravity
(COG) forward to balance themselves during NDT training [10].
In contrast with other gait-training methods that depend on mechanical
aids, NDT applies facilitated interventions to cultivate the effects of
motor learning. With minimum intervention, NDT applies stimulating
interventions at critical times to correct patients’ inaccurate
movements, thereby enhancing their compensatory movements and daily
activities. Utilizing training techniques based on the NDT theory allows
patients to learn correct movement patterns through motor learning
because of the human brain’s learning capability and high plasticity [11,12,13].
NDT
training has shown positive effects on stroke patients, but it places
heavy demands on participating therapists, and human factors influence
the quality of training. For these reasons, Wang et al. [14]
developed an automatic mobile NDT trainer that repeats therapeutic
interventions that the therapist must typically perform every time.
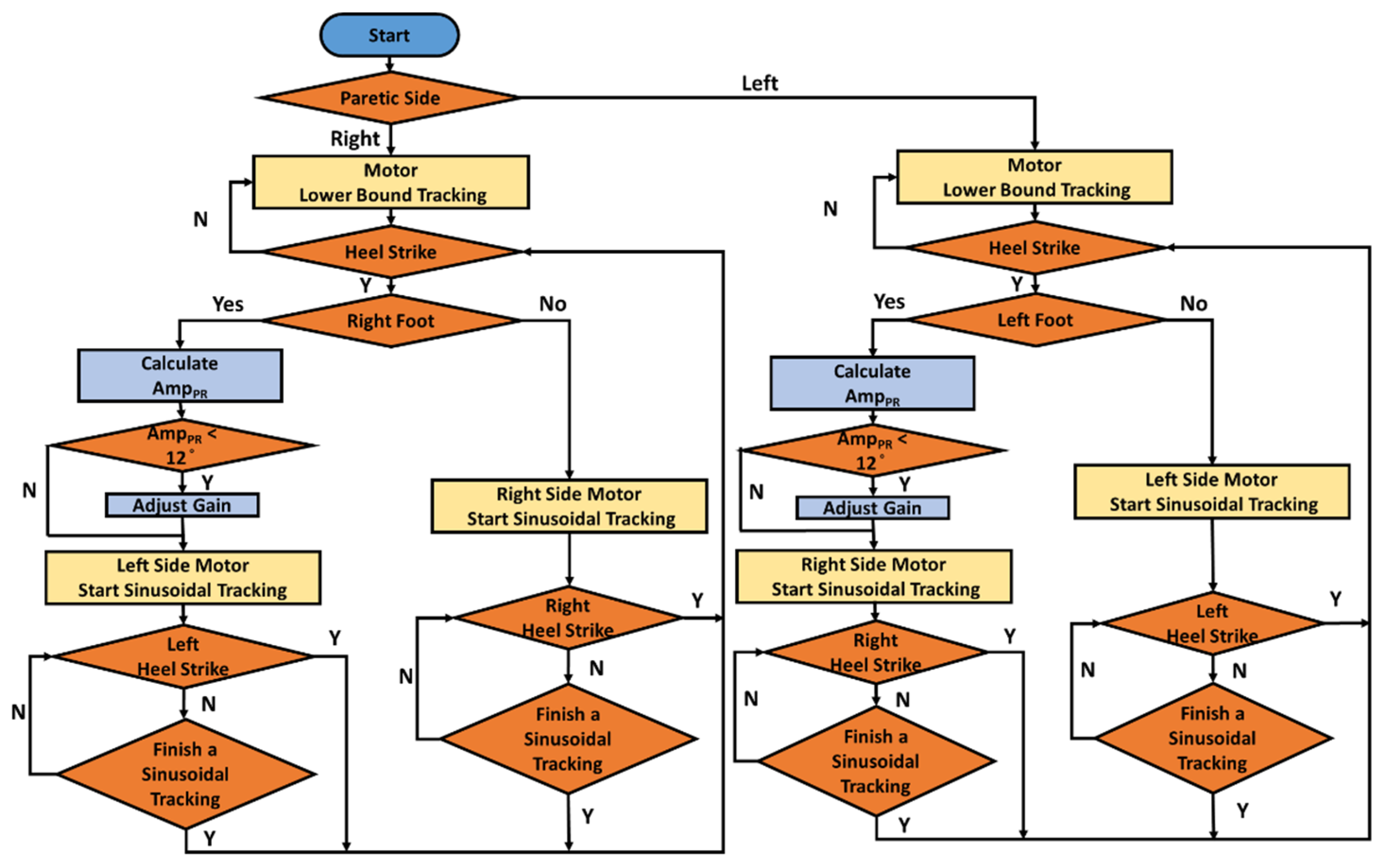
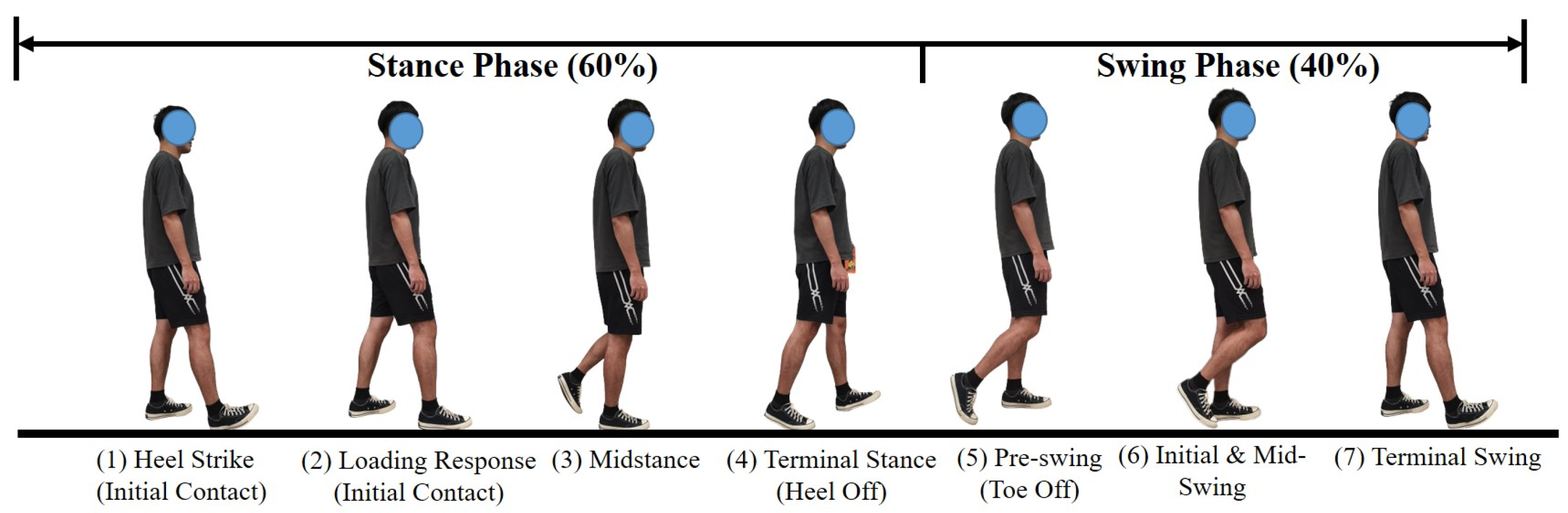
Their analysis of patients’ movements and therapists’ actions revealed
that the therapists conducted NDT intervention primarily at the heel
strike (HS) events. Hence, they applied a motion-capture system to
detect the HS. Wang et al. [15]
later proposed a movable NDT trainer that allowed the users to receive
visual feedback during training. They attached inertial measurement
units (IMUs) to the user’s legs and measured the kinematic data to
identify three essential gait events: the mid-swing (MS), HS, and toe
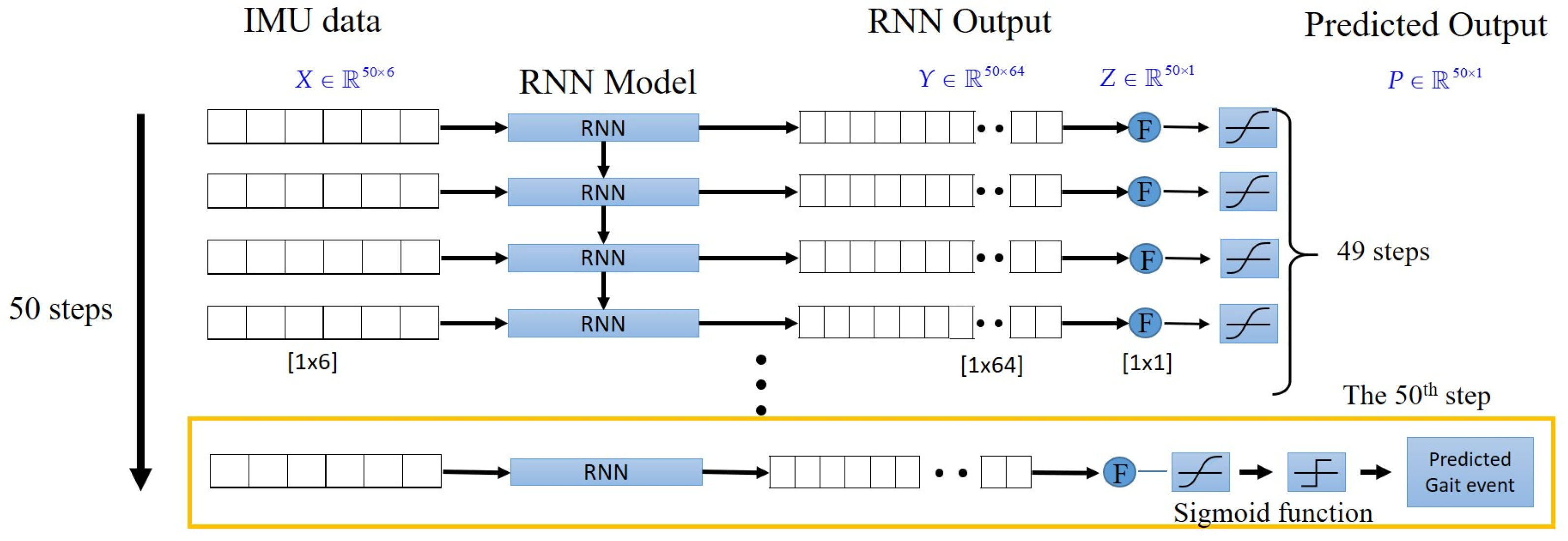
off (TO). Wang et al. [16]
developed a Long Short-Term Memory (LSTM) model, which is an advanced
recurrent neural network to process and predict time-series data to
detect HS events effectively. They applied experimental gait data to
develop a gait-detection model, which sent a triggering signal to motors
to repeat NDT interventions upon detecting an HS. The experimental
results showed that subjects improved their gait performance after the
NDT training. In this paper, we applied the LSTM model to detect HS
events based on IMU data and designed robust control to repeat NDT
interventions by a motor system.
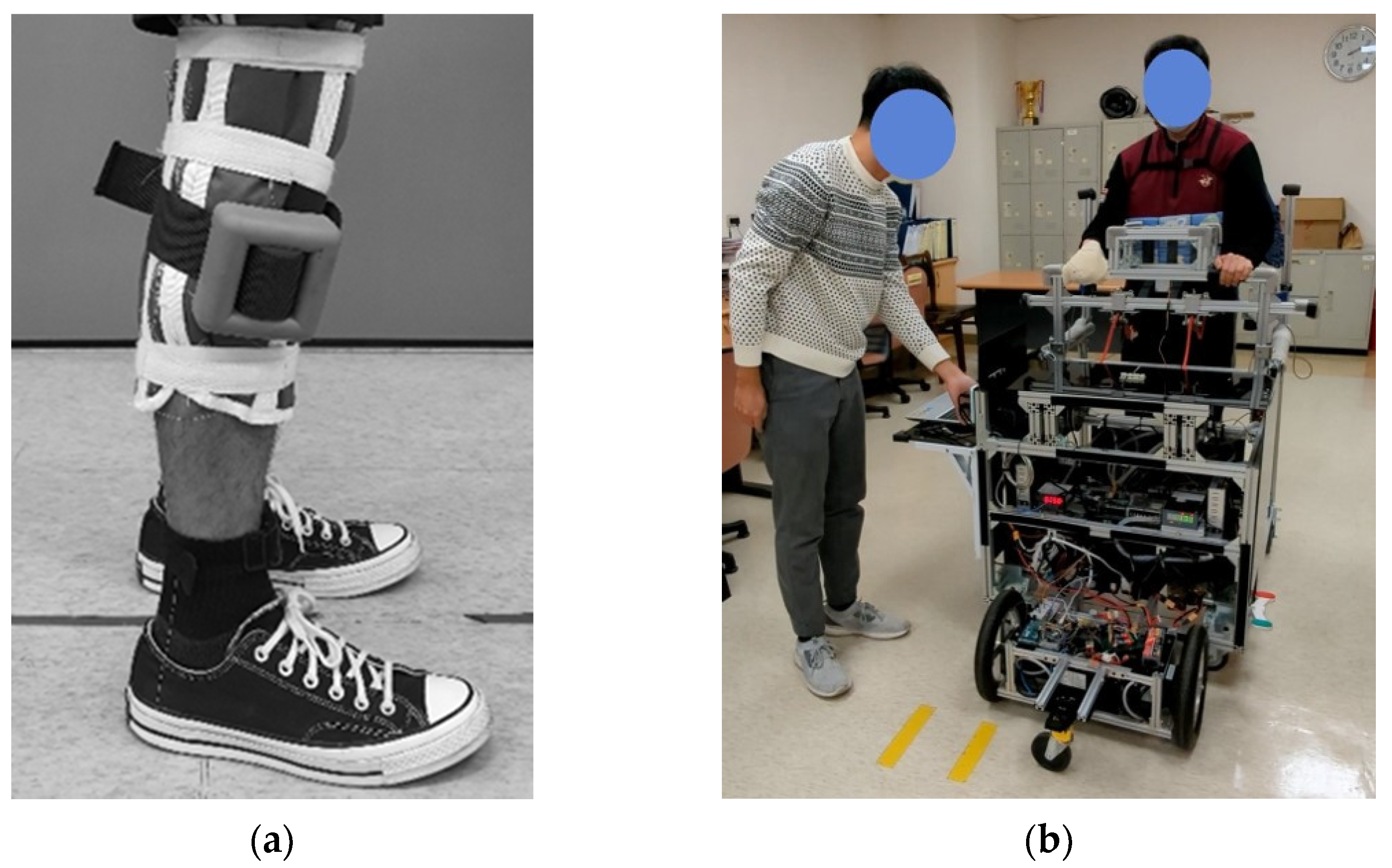
During
clinical experiments, however, we found that operating the
self-propelled mobile trainer could be burdensome for stroke patients,
who usually exhibit a significant reduction in muscle strength in their
legs, especially on the paretic side [17].
Therefore, this paper proposed a power-assisted device to let the
trainer follow the user, thereby allowing stroke patients to focus on
gait training without having to manually propel the trainer. We
conducted system identification and control design for the
power-assisted NDT trainer. We then implemented the designed controller
and recruited ten healthy subjects who wore a joint restrictor to mimic
stroke gaits to test the power-assisted trainer. We then invited 12
stroke patients to participate in clinical experiments. We evaluated the
rehabilitation effects by the swing-phase symmetry, pelvic rotation,
and walking speeds during and after receiving the NDT training with the
power-assisted device.
Gait symmetry is an
essential index for the gait rehabilitation of post-stroke patients and
requires shifting the COG at the right moments to initiate stepping [14]. The rotation of the pelvis reduces the center of mass movement and thereby conserves energy [18]. Increasing walking speed can improve the quality of daily life of stroke patients [19]. Darcy et al. [20]
suggested that improving stroke patients’ walking speed could reduce
energy consumption. Reciprocal and repeated training can help patients
improve their gaits by motor learning and accumulating experience from
comparisons with the sound side. This study showed that the subjects’
gait performance and walking speeds improved after receiving NDT
rehabilitation by using the proposed trainer.
More at link.
No comments:
Post a Comment