But why are you doing such a slow method for diagnosing stroke? Or don't you follow stroke research at all?
Hats off to Helmet of Hope - stroke diagnosis in 30 seconds; February 2017
New Device Quickly Assesses Brain Bleeding in Head Injuries - 5-10 minutes April 2017
Smart Brain-Wave Cap Recognises Stroke Before the Patient Reaches the Hospital
October 2023
Put this all together in a protocol and you could save billions of neurons and maybe get stroke patients to walk out of the hospital immediately.
The latest here:
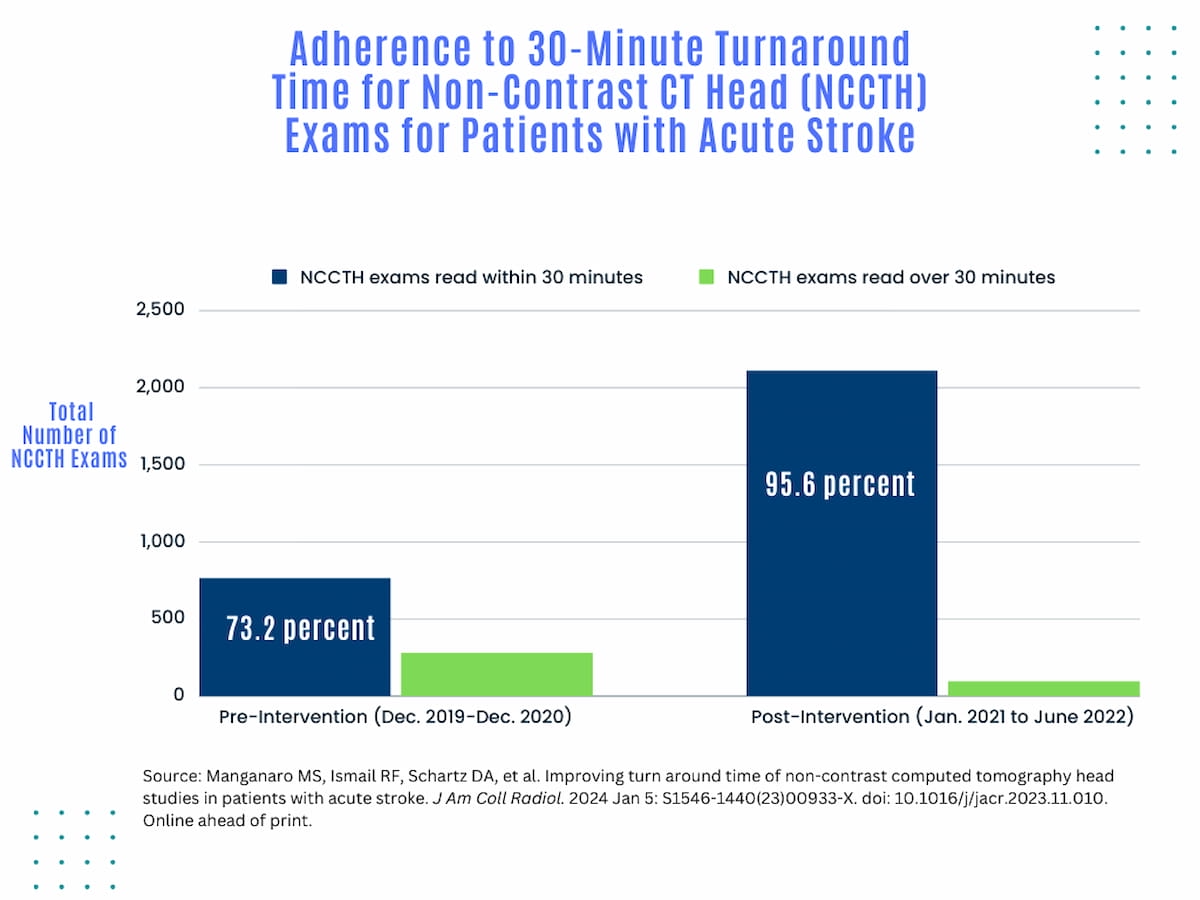
Head CT for Acute Stroke Patients: Study Shows 22 Percent Improvement for 30-Minute Turnaround Times
Modifications to the radiology workflow, including the use of a structured report template, improved adherence for 30-minute turnaround times for acute stroke head CT results from 73.2 percent to 95.6 percent, accordingly to new research.
Emerging research suggests significant improvements to turnaround times for head computed tomography (CT) exams in acute stroke cases can be achieved with simple modifications to radiology workflow, including the use of a structured report template.
For the retrospective study, recently published in the Journal of the American College of Radiology, researchers reviewed 1,046 cases involving head CT turnaround times (TATs) and noted potential factors contributing to TATs of more than 30 minutes. The study authors noted that possible etiologies of prolonged TATs may include increasing imaging volume, inconsistent worklist prioritization for acute stroke triage, lack of a separate picklist for acute stroke exams and lack of a standardized template for assessing patients with acute stroke.
Accordingly, the study authors instituted a standardized preliminary structured template for head CT exams, utilized a “super stat” purple color code designation on PACS worklists for all exams with concern for stroke and emphasized reminders of TAT benchmark expectations at monthly departmental quality conferences for radiologists.


In an 18-month period after implementing radiology workflow changes, including use of a standardized structured template for head CT exams, the researchers found that 95.6 percent of 2,112 CT head exams had turnaround times (TATs) within 30 minutes in comparison to 73.2 percent of CT head exams prior to implementation of the workflow changes.
In a 18-month period after implementing these workflow changes, the researchers found that 95.6 percent of 2,112 CT head exams had TATs within 30 minutes in comparison to 73.2 percent of CT head exams prior to implementation of the workflow changes.
“The series of interventions performed to reduce the TAT of (non-contrast computed tomography head) examination completion to a preliminary digital read for acute stroke CT interpretation effectively improved the ability of our academic radiology department to meet state and national certification requirements for timely stroke care,” wrote lead study author Mark S. Manganaro, D.O., who is affiliated with the Department of Imaging Sciences at the University of Rochester Medical Center in Rochester, N.Y., and colleagues.
The study authors conceded that staggered implementation of the aforementioned workflow modifications made it difficult to determine which one had the most impact. However, they noted that the standardized template appeared to facilitate sustained improvement with 30-minute TAT adherence and emphasized that all of the workflow changes are easy to implement.
“These interventions are relatively simple and can be utilized and replicated at other radiology departments facing a similar challenge across the United States,” added Manganaro and colleagues.
No comments:
Post a Comment