http://www.nature.com/news/2011/110413/full/472156a.html
Title: Brain Stimulation to Accelerate Learning of Threat Detection, Phase II
Purpose of Study: The research is to investigate how the brain responds to learning tasks to recognize visual targets in synthetic radar imagery. Also, we will be using Transcranial Direct Current Stimulation (TDCS) in attempt to accelerate learning.
Last year a succession of volunteers sat down in a research lab in Albuquerque, New Mexico to play DARWARS Ambush!, a video game designed to train US soldiers bound for Iraq. Each person surveyed virtual landscapes strewn with dilapidated buildings and abandoned cars for signs of trouble — a shadow cast by a rooftop sniper, or an improvised explosive device behind a rubbish bin. With just seconds to react before a blast or shots rang out, most forgot about the wet sponge affixed to their right temple that was delivering a faint electric tickle. The volunteers received a few milliamps of current at most, and the simple gadget used to deliver it was powered by a 9-volt battery.It might sound like some wacky garage experiment, but Vincent Clark, a neuroscientist at the University of New Mexico, says that the technique, called transcranial direct-current stimulation (tDCS), could improve learning. The US Defense Advanced Research Projects Agency funded the research in the hope that it could be used to sharpen soldiers' minds on the battlefield. Yet for all its simplicity, it seems to work.
Volunteers receiving 2 milliamps to the scalp (about one-five-hundredth the amount drawn by a 100-watt light bulb) showed twice as much improvement in the game after a short amount of training as those receiving one-twentieth the amount of current1. "They learn more quickly but they don't have a good intuitive or introspective sense about why," says Clark.
The technique, which has roots in research done more than two centuries ago, is experiencing something of a revival. Clark and others see tDCS as a way to tease apart the mechanisms of learning and cognition. As the technique is refined, researchers could, with the flick of a switch, amplify or mute activity in many areas of the brain and watch what happens behaviourally. The field is "going to explode very soon and give us all sorts of new information and new questions", says Clark. And as with some other interventions for stimulating brain activity, such as high-powered magnets or surgically implanted electrodes, researchers are attempting to use tDCS to treat neurological conditions, including depression and stroke. But given the simplicity of building tDCS devices, one of the most important questions will be whether it is ethical to tinker with healthy minds — to improve learning and cognition, for example. The effects seen in experimental settings "are big enough that they would definitely have real-world consequences", says Martha Farah, a neuroethicist at the University of Pennsylvania in Philadelphia.Getting to this point, however, was hardly straightforward. Direct-current brain stimulation has emerged from a long, touch-and-go history that ranges from the simply bizarre to the simply irreproducible. And for some, it still has much to prove.
The Italian scientist Jean Aldini first tried direct-current stimulation around 1800 — initially to induce movement in the corpses of recently executed felons. Later, he claimed in a paper to cure two acquaintances of the mood disorder then known as 'melancholy'. By the 1940s, many patients with depression were being given electric shocks to the temples that were strong enough to induce seizures — so-called electroconvulsive therapy. But for decades people toyed with the idea of treating mental illness with electric shocks that were much milder — 1,000 times less intense than electroconvulsive therapy.
Weak origins
In 1964, Joe Redfearn, a psychiatrist at Graylingwell Hospital in Chichester, UK, applied some promising results in rats directly to humans, delivering weak currents — of 50–250 microamps — to the scalps of volunteers. He reports that the volunteers became talkative, even giggly, when current was run in one direction, but withdrawn when it ran the other way2. He gave the 'giggly' treatment to 29 patients with depression and claims that half of them improved3. But no one could replicate his results, and the technique was abandoned.
In retrospect, several factors seem to have undermined his work. Among them, Redfearn used currents ten times lower than in modern tDCS — perhaps because he had no way to measure how much electricity was actually reaching his patients' brains. Within a few decades, however, the necessary methods would become available, notably as researchers began to study brain activity induced by transcranial magnetic stimulation (TMS). In TMS, a magnetic coil running at thousands of volts is positioned just outside the head, leading to electrical surges inside the brain that can be precisely measured with external electrodes. Alberto Priori, a neuroscientist now at the University of Milan in Italy, showed in the 1990s that tDCS increased the effectiveness of TMS. He stimulated the motor cortex of volunteers for seven seconds with a direct current of 0.5 milliamps, then started hitting the area with short bursts of TMS.
The assumption was that if tDCS made neurons more responsive, then more of those neurons would respond when TMS was subsequently applied. It turned out to be true — volunteers who got a short pulse of direct current had a larger response to TMS. But when Priori presented his results in 1993, colleagues doubted that the electricity was penetrating the skull. It took him until 1998 to convince reviewers that his results were bona fide4.
Michael Nitsche, a clinical neurologist at the University of Göttingen in Germany, was intrigued by the published findings. He had been experimenting with TMS to treat epilepsy at the time — but the equipment is unwieldy and expensive, and its effects on brain activity were too brief to help patients. Nitsche, a recent graduate at the time, and his supervisor, Walter Paulus, spent a year fiddling with tDCS. Their interest alarmed their colleagues. "It's fucking dangerous," Nitsche recalls being told. "You should stop this immediately." Nitsche managed to get his studies approved by university ethics boards, but a shortage of volunteers willing to have their brains zapped often forced him to experiment on his father, his sister and himself.
In 2000, Nitsche and Paulus published a paper5 showing that up to five minutes of weak current — around 1 milliamp — on the human scalp renders the motor cortex more responsive to signals for several minutes after the electricity is shut off. Like Priori, he used TMS to measure the effects.
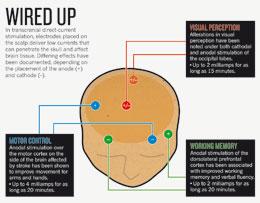
Nitsche and others have begun to clarify how tDCS works. Physiological studies indicate that direct current creates an electric field in brain tissue that changes the voltage across the neuronal membranes. 'Anodal' stimulation, in which electrons flow into the electrode on the head, pulls neurons a few millivolts towards 'depolarization', making them more likely to fire when signals arrive from other cells. 'Cathodal' stimulation, in which electrons flow out of the electrode on the head, has the opposite effect, 'hyperpolarizing' neurons and making them less responsive to signals from other cells.Effects seen after the electricity is shut off can last for an hour or so and seem to arise from a second mechanism. Pharmacological evidence suggests that the current increases the expression of proteins called NMDA receptors at the synapses, the connections between neurons. This heightens the plasticity of brain tissue — leaving it in a temporary state somewhat like wet clay, in which it is more apt to reshape its synaptic connections in response to stimuli, such as when learning a video game.
 Click for larger version.
Click for larger version.
Researchers are exploring the ways in which this wet-clay state can be exploited. In a 2009 study6, Leonardo Cohen at the National Institute of Neurological Disorders and Stroke in Bethesda, Maryland, showed that tDCS improved people's ability to learn a simple coordination exercise — and that the improvement was still apparent three months after the experiment ended. Such results have led to an interest in stroke rehabilitation strategies. Small trials by Cohen, Nitsche, and others have shown improved recovery of hand function when tDCS is used this way (see 'Wired up').
Another group of researchers, led by Felipe Fregni of the Berenson-Allen Center for Noninvasive Brain Stimulation in Boston, Massachusetts, and Paulo Boggio of Mackenzie Presbyterian University in São Paulo, Brazil, is experimenting with tDCS as a way to treat depression. Several small trials done by this group and others suggest that a few sessions of tDCS to a part of the brain called the dorsolateral prefrontal cortex can improve mood for several weeks.Risky approach
In 2007, Boggio and Fregni reported that applying tDCS to the same region can make people less likely to take risks7. They asked healthy university students to play a game in which they press a computer key to pump air into a cartoon balloon. The more they pump, the more virtual money they earn — but if the balloon bursts, they lose all their winnings. People treated with tDCS were less willing to push their luck. The results may be generalizable to addictions, in which people lack "inhibitory control", says Boggio. In 2008, he and Fregni published three studies8–10 showing that stimulation of the dorsolateral prefrontal cortex blunted cravings for alcohol, cigarettes and sweets when people later watched videos in which these were being consumed. They hope, eventually, to test the same technique in a clinical trial for smoking cessation.
“There has been a lot of hokey stuff, and it affects the credibility of the entire field.”
Not everyone is convinced that the disappointments are over, though. Helen Mayberg, a clinical psychiatrist at Emory University in Atlanta, Georgia, has been experimenting with the use of deep-brain stimulation (DBS), in which electrodes are placed deep in the brain, to treat depression. She is excited about the non-invasiveness of tDCS but points out that the trials conducted to date have been short-term. The real questions, she says, will be: "How do you use it chronically, and what kinds of rebounds and relapses are there?" Boggio and others have begun a clinical trial to answer this question, in which patients being treated with tDCS for depression will be observed for up to six months.
Target practice
Still, the stimulation from tDCS is less focused than that from TMS or DBS. Its effects on neurons also drop off rapidly a few centimetres below the scalp, putting some important medical targets out of reach.Bikson has designed a more refined version of tDCS that he hopes will address these shortcomings. Instead of one electrode, he places five on the head in an X configuration. The one in the centre pushes current in the desired direction and the four around it siphon off excess current that would otherwise spread and activate wider brain areas. The configuration could, he says, allow for slightly higher currents that would penetrate deeper into the brain in more focused areas. Such innovations might even help to persuade companies to invest in clinical trials. Currently, Cohen says, no one stands to gain enough return from therapies that can be administered using just US$1,000 worth of off-the-shelf equipment.
Aside from treatment, tDCS is also receiving attention for its potential to enhance the minds of healthy people. In addition to Clark's work showing enhanced ability to see concealed threats, other studies with tDCS have shown improvements in working memory11, word association12 and complex problem-solving13. Most of these studies address scientific questions — but one neuroscientist unabashedly aims to boost the brains of healthy people.
Allan Snyder, director of the Centre for the Mind at the University of Sydney in Australia, hopes to develop "a thinking cap", a tDCS device that corporate executives or advertising copywriters might use to bump up their creativity before walking into a brainstorming meeting. Snyder is cagey about how far he is in product development — but his latest demonstration, published this February14, garnered plenty of attention. Snyder claims to have boosted people's flair for sudden insight by stimulating their anterior temporal lobes. People who received tDCS were two to three times more likely than those receiving sham stimulation to solve a creativity problem in which they raced against the clock to spell out maths equations with matchsticks.
The jury is still out on whether these results will translate into real-world benefits. Nitsche says that it will be harder to improve cognition in young, healthy people — whose minds are theoretically already optimized — than in elderly people or those with addictions, for instance. "I wouldn't say it wouldn't be possible," says Nitsche. "But things might be a little more complicated."“With wires and batteries and home hobbyists trying to run electricity through their heads, somebody could get hurt.”
And wider adoption raises ethical concerns similar to those that surround mind-enhancing drugs such as Adderall and Modafinil, which some students take as study aids. Students might secretly 'electrodope' with tDCS before a university entrance exam to inflate their scores. Ethicists worry that this will give some an unfair advantage or create a culture in which people feel pressured to use such devices. None of the studies published so far have shown a type of mind-sharpening that would help in such exams, says Farah, but that might simply be a matter of targeting the right brain areas. "It would not surprise me" if such effects were possible, she says.
Overall, though, the optimism among tDCS's believers remains high. Although it has generated some disappointments, many are convinced that the present buzz is warranted. "Sometimes in the history of medicine you have to try again after one century or so," says Priori. "You use a novel technical device, and you succeed where somebody else failed."
I wonder if this has any applicability to stroke recovery?
No comments:
Post a Comment