If you want this in your hospital YOU will need to initiate. Your hospital has no person assigned to read and implement research. Why should they? The status quo is good enough outcome. If 10% full recovery and 12% tPA full recovery aren't good enough, why aren't stroke survivors complaining and filing lawsuits? Maybe because they have been bamboozled into accepting that fucking tyranny of low expectations provided by your stroke medical professionals.
CODE STROKE ALERT—Concept and Development of a Novel Open-Source Platform to Streamline Acute Stroke Management
- 1Neurointerventional Service – Department of Radiology, Monash Health, Clayton, VIC, Australia
- 2Deloitte, Sydney, NSW, Australia
- 3School of Medicine, Monash University, Clayton, VIC, Australia
- 4Department of Neurology, Monash Health, Clayton, VIC, Australia
- 5Neurointerventional Service – Department of Radiology, Austin Health, Melbourne, VIC, Australia
- 6School of Medicine, Deakin University, Waurn Ponds, VIC, Australia
- 7Alcohol Beverages Australia, Sydney, NSW, Australia
- 8Department of Engineering, Monash University, Clayton, VIC, Australia
- 9South Australian Health and Medical Research Institute, Adelaide, SA, Australia
- 10Department of Radiology, Northern Health, Epping, VIC, Australia
- 11Department of Neurology, Austin Health, Heidelberg, VIC, Australia
- 12School of Medicine, The University of Melbourne, Parkville, VIC, Australia
- 13Stroke Division, The Florey Institute of Neuroscience and Mental Health, University of Melbourne, Parkville, VIC, Australia
Introduction: Effective, time-critical
intervention in acute stroke is crucial to mitigate mortality rate and
morbidity, but delivery of reperfusion treatments is often hampered by
pre-, in-, or inter-hospital system level delays. Disjointed,
repetitive, and inefficient communication is a consistent contributor to
avoidable treatment delay. In the era of rapid reperfusion therapy for
ischemic stroke, there is a need for a communication system to
synchronize the flow of clinical information across the entire stroke
journey.
Material/Methods: A multi-disciplinary
development team designed an electronic communications platform,
integrated between web browsers and a mobile application, to link all
relevant members of the stroke treatment pathway. The platform uses
tiered notifications, geotagging, incorporates multiple clinical score
calculators, and is compliant with security regulations. The system
safely saves relevant information for audit and research.
Results: Code Stroke Alert is a
platform that can be accessed by emergency medical services (EMS) and
hospital staff, coordinating the flow of information during acute stroke
care, reducing duplication, and error in clinical information handover.
Electronic data logs provide an auditable trail of relevant quality
improvement metrics, facilitating quality improvement, and research.
Discussion: Code Stroke Alert will be freely available to health networks globally. The open-source nature of the software offers valuable potential for future development of plug-ins and add-ons, based on individual institutional needs. Prospective, multi-site implementation, and measurement of clinical impact are underway.
Introduction
Gold standard treatment of acute ischemic stroke relies
on timely reperfusion of ischemic cerebral tissue. The two primary
methods of reperfusion are thrombolysis using intravenous tissue
plasminogen activator (IV tPA) and mechanical thrombectomy. These
therapies have been proven to be effective in several randomized
clinical trials and meta-analyses (1–3). With rapid reperfusion therapy, up to 70% of patients may have good neurological recovery (4).
Mechanical thrombectomy is superior to IV tPA for acute
ischaemic stroke due to large vessel occlusion (LVO). In multiple recent
trials, the effect of time to reperfusion with mechanical thrombectomy
was directly proportional to patient outcome (5–7).
It is estimated that every 1-min reduction in the interval between
stroke onset and start of mechanical thrombectomy results in an
additional week of healthy living (8).
A comprehensive stroke service is necessarily complex,
involving medical professionals across multiple disciplines and
departments. Such an intricate system is prone to inefficiencies related
to delayed dissemination of information, communication duplication, and
error as well as the need for consensus decision making among stroke
specialists and neuro-interventionalists (NI). The time critical nature
of cerebral reperfusion is a compelling motivation to optimize
communication systems, allowing for synchronization and improved
coordination of clinical information (9).
To address this need, we aimed to develop a novel,
open-source, multi-platform communication application, named “Code
Stroke Alert,” that facilitates efficient multi-cast, tiered
communication during the hyperacute management stages of an ischaemic
stroke.
Stroke Pathway and Barriers to Timely Reperfusion
The basic pathway of communication in a stroke patient is outlined in Figure 1.
Most strokes occur in the community and rely on initial recognition by
the patient or a family member with subsequent first medical contact
with local emergency medical services (EMS). Pre-hospital triage and
care varies based on locality but generally involves a basic assessment
by trained paramedics and transfer to a local stroke centre. The
emergency department (ED) then alerts the radiology and stroke staff of
the impending stroke (in most hospitals this is achieved through a group
page). Much of the communication to this point is one-way, with limited
ability to provide confirmation by any party, nor detailed clinical
information.
FIGURE 1
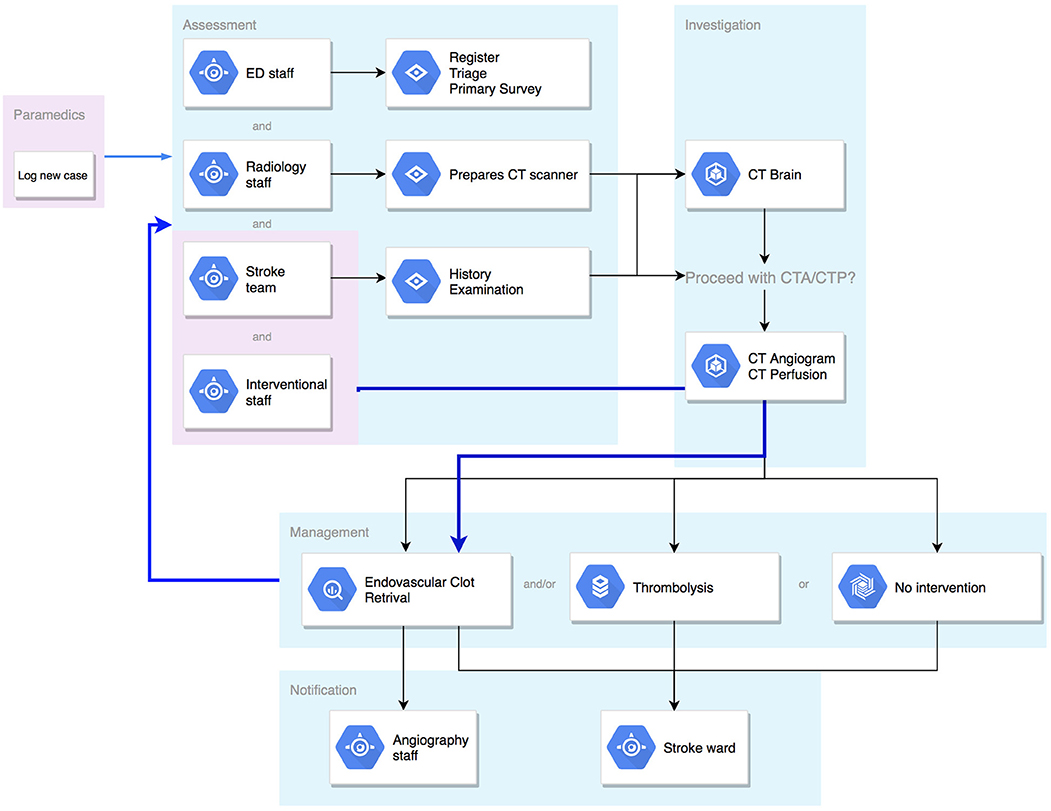 Figure 1. Flowchart of communication pathway in a stroke case.
Figure 1. Flowchart of communication pathway in a stroke case.
On arrival to hospital, multiple
processes happen quickly and simultaneously. The stroke patient will be
reassessed in detail by ED nurses, physicians, and the stroke team,
whilst simultaneous handover is provided by the paramedics. Throughout
this period, there is constant communication between all parties and
senior clinical decision makers within the team. Following clinical
assessment, the patient will proceed to neuroimaging with computed
tomography (CT). Based on imaging findings in correlation with clinical
assessment, a treatment decision will then be made. If the decision is
for mechanical thrombectomy, activation of the angiography lab and
anesthetics team must occur immediately, with broader notification
(stroke unit and admission logistics) shortly after commencement of the
procedure.
There are a number of points in this complex process which are vulnerable to delay (Table 1).
The initial recognition by community members is the first and there are
concerted efforts being made to improve health literacy to address this
issue. Once EMS have been contacted there is a triage and dispatch
process and then time spent in assessment and information gathering. A
decision has to be made regarding destination, followed by transport
time to the target hospital. Within the hospital environment there is a
further complex succession of medical assessment, imaging acquisition,
decision-making and treatment, and in some cases, transfer to a
mechanical thrombectomy-capable service may be required.
TABLE 1
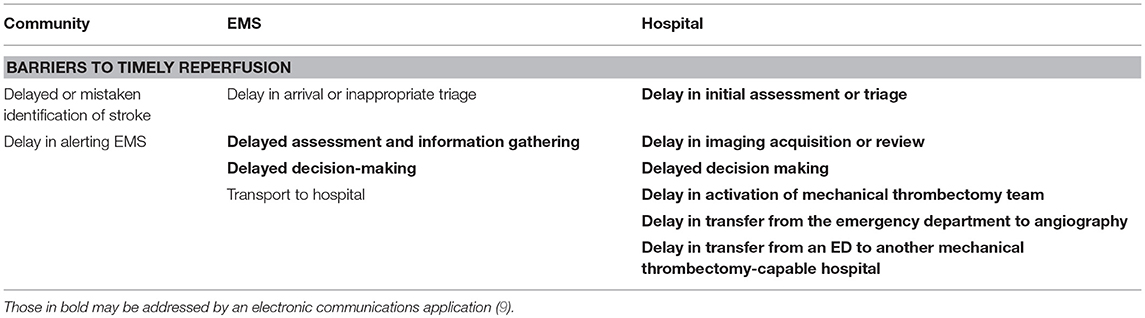 Table 1. Potential systemic barriers to timely reperfusion therapy.
Table 1. Potential systemic barriers to timely reperfusion therapy.
Up to 40 different health care
professionals may be involved in this entire process for an individual
stroke presentation. This includes, but is not limited to, paramedic
staff, ambulance staff, emergency staff, stroke physicians, stroke
nurses, radiologists, radiographers, radiology nurses, NI, anesthetics
staff, orderlies, junior medical staff, and administrative staff.
Reliable and efficient communication is a necessity in
such a scenario, but most hospitals currently rely on paging systems or
paper information sheets with multiple handovers and a sequential
dissemination of information. This can lead to communication
duplication, information loss, security concerns and, ultimately, time
delays. The bold text delays presented in Table 1
highlight points at which we hypothesized that a dedicated, electronic
information gathering and distribution program could accelerate the
pathway of a stroke patient.
More at link.
No comments:
Post a Comment