Among
Chinese patients with minor nondisabling stroke who presented within 4.5
hours of symptom onset, dual antiplatelet treatment was noninferior to
thrombolysis with intravenous alteplase with regard to functional outcome at 90 days in the ARAMIS trial.
The
trial was presented by Thanh Nguyen, MD, Boston Medical Center, on
February 10 at the International Stroke Conference (ISC) 2023 in Dallas,
Texas.
"Given the ease of administration, less intensive
monitoring, low cost, and safety profile of dual antiplatelet therapy,
the current findings support the use of dual antiplatelet in this
population," Nguyen concluded.
Commenting on the ARAMIS trial for theheart.org | Medscape Cardiology,
Pooja Khatri, MD, professor of neurology at the University of
Cincinnati, Ohio, and lead investigator of the previous PRISMS study of
tissue plasminogen
activator (tPA) or alteplase in mild stroke, said the results
reinforced the current recommendations of giving dual antiplatelet
therapy but not alteplase to these patients.
Noting that the standard of care is now to give dual
antiplatelet therapy to these patients, Khatri said: "These data
reassure that this remains the right way to go."
She added that her take-home message from the study would
be: "Keep giving dual antiplatelet therapy, and we may be doing more
harm than good with alteplase in this patient population."
Introducing her presentation, Nguyen explained that mild ischemic stroke,
defined as having a National Institutes of Health Stroke Scale (NIHSS)
score of 5 or less, comprises half of ischemic stroke patients in the
US. But the benefit of thrombolysis in patients with minor ischemic
stroke that is not disabling is unknown.
A subgroup analysis
of one of the major thrombolysis trials (IST-3) found that a higher
proportion of patients with mild ischemic stroke that was treated within
3 hours of symptom onset were alive and independent at 6 months if they
had been given thrombolysis (84%), compared to 65% in the control group
who received standard medical treatment.
This led to the first randomized trial (PRISMS)
dedicated to patients with mild nondisabling stroke, which found that
alteplase given within 3 hours of symptom onset did not increase the
likelihood of a good functional outcome at 90 days in comparison with
single-agent aspirin.
The study was unfortunately terminated early for administrative
reasons, and no definitive conclusions could be drawn on the basis of
these results, Nguyen reported.
In 2018, the American Heart Association/American Stroke Association
guidelines indicated that for patients who present within 3 hours of
symptom onset with mild ischemic stroke that was judged to be
nondisabling, thrombolysis with intravenous alteplase could be
considered, she noted.
In the meantime, dual antiplatelet therapy was shown to be safe and effective in the POINT and CHANCE
trials in patients presenting with minor stroke within 12 or 24 hours,
and the CHANCE trial also found a benefit in reducing recurrent stroke
that was most effective in the first 2 weeks.
The current ARAMIS
trial was therefore conducted to evaluate dual antiplatelet therapy in
comparison with thrombolysis for patients with acute minor stroke (NIHSS
5 or less) who presented within 4.5 hours of symptom onset and were
without clearly disabling deficit.
The trial was conducted in 38 hospitals in China and
included 760 patients (median NIHSS score of 2) who were randomly
assigned to receive intravenous alteplase at the standard dose of 0.9
mg/kg, followed by guideline-based antiplatelet treatment, or dual
antiplatelet therapy (clopidogrel 300 mg plus 100 mg aspirin loading
dose followed by 10 to 14 days of aspirin 100 mg and clopidogrel 75 mg).
The trial was designed to assess noninferiority of dual antiplatelet therapy to alteplase with noninferiority margin of -4.5%.
In
the modified intention-to-treat analysis, which included 722 patients,
the primary outcome (excellent functional outcome, defined as a Modified Rankin Scale
score of 0 or 1 at 90 days) occurred in 93.8% of patients in the dual
antiplatelet therapy group and in 91.4% of the alteplase group. This
gave a difference of 2.4%, which fell within the limits for
noninferiority (P = .0002 for noninferiority test).
"Therefore, this was a positive trial," Nguyen stated.
About
20% of patients crossed over from the dual antiplatelet group to the
thrombolysis group, and about 16% of patients crossed over from the
thrombolysis group to the dual antiplatelet group. But a per-protocol
and an "as treated" analysis showed similar results to the main
intention-to-treat analysis.
Secondary
outcomes were largely similar between the two groups other than early
neurologic deterioration, which was less common in the dual antiplatelet
therapy group.
In terms of safety, symptomatic intracranial hemorrhage
occurred in 0.3% (1/369) in the dual antiplatelet group and in 0.9%
(3/350) in the alteplase group, a nonsignificant difference.
Events
of "any bleeding" occurred in more patients in the thrombolysis group
(5.4%) than in the dual antiplatelet therapy group (1.6%), and this
difference was significant (P = .01).
Subgroup
analysis showed a trend toward benefit of alteplase for patients with
higher NIHSS score at baseline (NIHSS >3). Otherwise, the other
subgroups looked similar to the main results.
Dual Antiplatelet Therapy Now Standard of Care
Nguyen
pointed out one limitation of the study ― that dual antiplatelet
therapy was updated to standard treatment in this target population in
the 2019 AHA/ASA guidelines.
In her discussion of the study, Khatri suggested that the ARAMIS results were what might have been expected.
"Dual
antiplatelet therapy is designed to prevent stroke. Even in the POINT
trial, dual antiplatelet therapy showed no effect on 90-day functional
outcome. It was really about prevention. The PRISMS trial suggested that
alteplase was also unlikely to improve 90-day functional outcome in
this population of patients with mild and not clearly disabling stroke.
So, it is not surprising that dual antiplatelet therapy was noninferior
to alteplase for 90-day functional outcome for both those reasons," she
explained.
"That being said, while
designed as a noninferiority study, it is interesting to note that
alteplase again showed no evidence of treatment effect compared to
antiplatelet therapy, affirming what was observed in the prematurely
terminated PRISMS trial," Khatri added.
In
a discussion of the study at an ISC 2023 highlights session, ISC
program chair Tudor Jovin, MD, Cooper Neurological Institute, Cherry
Hill, New Jersey, said: "This is very important data and it's actually
the first completed trial that examines this question."
But,
he added, "I think we need to refine our knowledge about what a
nondisabling stroke actually is. You could argue that every stroke is
disabling. I think we need more clarity on this definition, as in
practice, many clinicians still give tPA on account of these mild
strokes still being disabling."
The
ARAMIS trial was funded by the National Key R&D Program of China
and the Science and Technology Project Plan of Liao Ning Province.
Nguyen reports research support from Medtronic that was not related to
the current study.
International Stroke Conference (ISC) 2023: Abstract LB23. Presented February 10, 2023.
For more from the heart.org | Medscape Cardiology, follow us on Twitter and Facebook.

 Giovanni Merlino
Giovanni Merlino Lorenzo Nesi2†,
Lorenzo Nesi2†,  Sara Pez
Sara Pez Yan Tereshko
Yan Tereshko Giuseppe Sportelli
Giuseppe Sportelli Julia Ferrari
Julia Ferrari Audrey Reynolds
Audrey Reynolds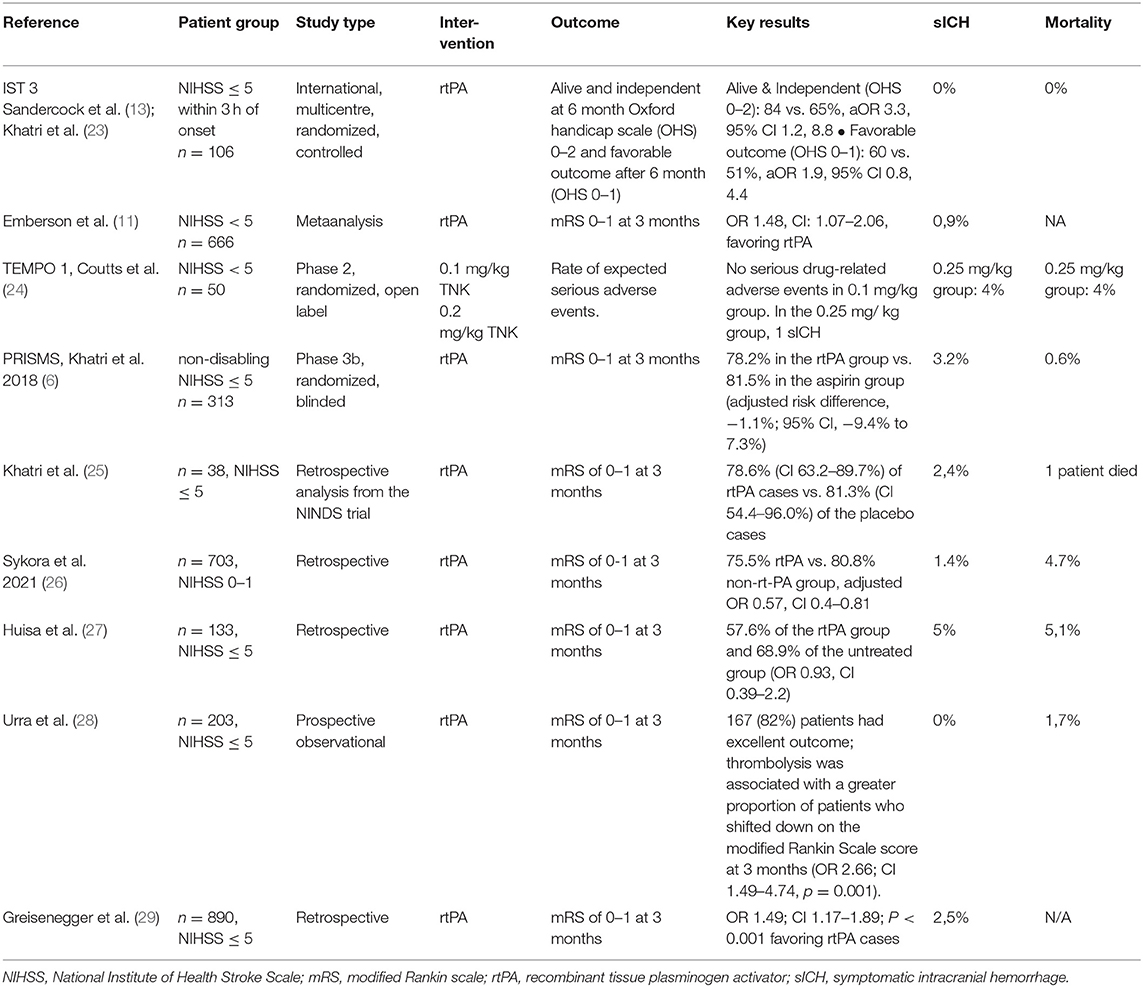

 Aleksandra Yakhkind
Aleksandra Yakhkind Ryan A. McTaggart2,
Ryan A. McTaggart2,
 Brian Silver
Brian Silver Shadi Yaghi
Shadi Yaghi{kind=link}