If your therapists don't understand that the way to get to this is 100% recovery protocols; then you don't have a functioning therapist!
Improving Strength and Mobility with Healthy Stability: A Case Report
Written By: Lori Duncan, DPT, MTC, CPT
 As
therapists, we are always trying to optimize our patient’s function and
independence. This requires a combination of strength, mobility, and
stability. So where do we start?
As
therapists, we are always trying to optimize our patient’s function and
independence. This requires a combination of strength, mobility, and
stability. So where do we start?
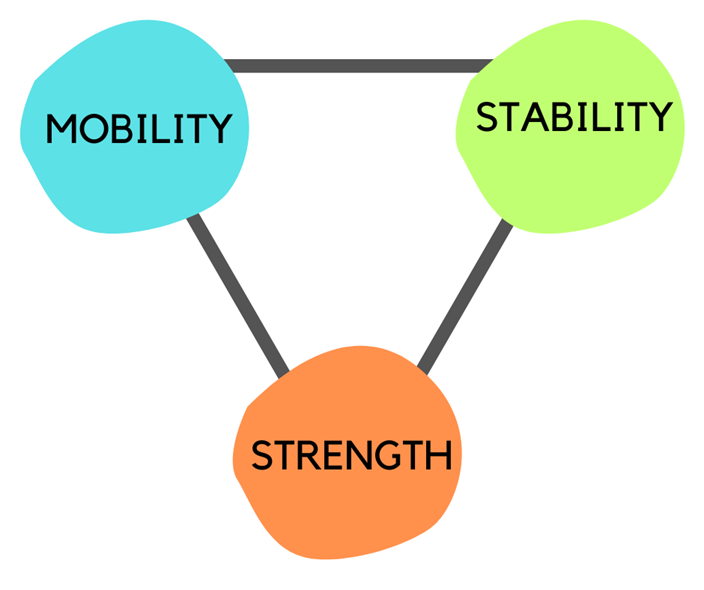
Over the years, I have found that stability is often missed, skipped, or devalued in a patient’s rehabilitation program; however, the first 6-8 weeks of muscle gain is a chit-chat between the muscle and brain. This is neuromuscular recruitment (i.e. stability or motor control) not a change in muscle fiber size. In general, poor stability results in poor symptom resolution, and decreased strength and function. This is a schematic I use (I draw this for my patients) to show them the relationship of mobility, stability, and strength. Notice that strength is below, or after, mobility and stability. Yet so many rehabilitation programs begin with strength.
Here is a case report of a patient I am currently treating to illustrate the importance of the stability link to optimize our patient outcomes.
Clinical Notes:
September 2023: A 47-year-old man presented with significant right quadriceps atrophy after experiencing rhabdomyolysis from a compression injury in July 2023. He had been in rehab for 4+ weeks prior to our meeting but was still experiencing significant knee pain, functional weakness with stairs, and right quad a trophy.
For review, rhabdomyolysis is when damaged muscle releases muscle cell contents (i.e. Myoglobin, creatine kinase, etc.) into the blood. This release of cell contents can then cause a host of different organ damage. Luckily, this patient was treated quickly enough and only had resultant muscle atrophy.
His program from August-September 2023 (prior to coming to my clinic):
- Lunges, squats, bridging, and walking on the treadmill
Lunges, squats, and bridging are FABULOUS exercises, but they are
very strength-based. For a patient dealing with such significant quad
atrophy, this was simply too much on the system and he was loading his
knee joint. Watch
the progression we used to resolve his knee pain and develop his
quadriceps muscle. It’s not strength-based movements at first.
September 2023 (initial program at my clinic):
- Stability/Mobility: Pilates-based movements for the VMO, glutes and quads
- Stability/Mobility: Physioball supine walkouts and HS curls
October 2023 (after 1 month he reported his symptoms were improving and was able to negotiate stairs with more confidence):
- Stability/Mobility: Continued Pilates-based movements
- Stability/Mobility: BOSU kneeling and bird dog
- Strength: SL squat assisted and only to mid-range
- Carioca for coordination and improved confidence with RLE
November 2023 (after 2 months he reported he was able to get up and down from the floor without pain):
- Stability/Mobility: Pilates side-series for glutes, VMO and RLE endurance
- Stability/Mobility: Physioball forearm planks, lateral lunge supported
- Stability/Mobility: BOSU SL kneeling, bird dog knee to nose and standing SL balance
- Strength: SL squat + hover over the chair, squat to toes reach
- Mobility isolated: prone quad stretch to tolerance, dynamic not static
This is only one example of how the emphasis on early stability and mobility will optimize patient symptoms and outcomes; the possibilities are endless for how to incorporate this principle into treatment. In the end, our role as clinicians is to meet each patient where they are at and progress them appropriately so they can have a healthy return to their life and independent function outside of rehab.
Interested in learning more? Attend any or all of my 4 Live Streams on Improving Strength and Mobility taking place January 26th & 27th. Hope to see you there!
Explore online continuing education courses from Lori below:
No comments:
Post a Comment