You better hope as a young adult stroke person you even get to this stage. You better have classic stroke symptoms, drooping mouth, slurred speech, one side useless.
WRONG: PA Told MD It Was a 'Wine Headache' -- She Almost Died
Factors Associated With Misdiagnosis of Acute Stroke in Young Adults
Pediatric Stroke Often Misdiagnosed, Treatment Delayed
Doctors tell boy, 15, he had a migraine after rugby tackle - but he was actually suffering a paralyzing stroke which nearly killed him
The latest here:
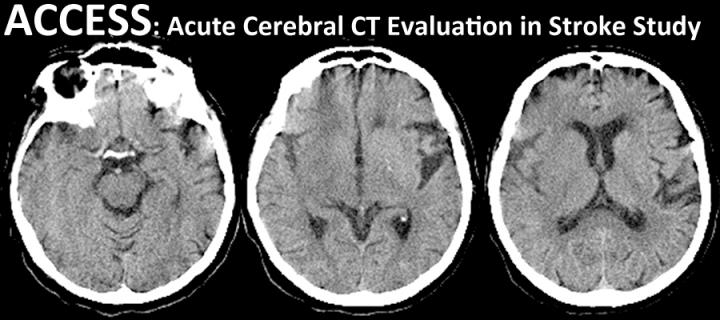
Acute Cerebral CT Evaluation of Stroke Study (ACCESS)
ACCESS helps you to learn about how to read acute stroke
CT scans. Participation also helps to increase the amount of data
available on observer reliability.
REGISTER FOR ACCESS
- We will send you a password with which to login to the ECCITING online teaching platform
LOGIN TO ACCESS
- ACCESS was launched originally in 2004
Quick links
-
ACCESS quick notes for participants
- Take the BASP CT Training Lecture beforehand here
- Integrate imaging training with STARS Thrombolysis Masterclass
Background
ACCESS has been running continuously since 2004. Over 1,000 people have participated.ACCESS is therefore one of the largest studies of observer reliability. It is definitely the largest study of observer reliability in stroke.
We describe results from the initial study in two papers:
- Wardlaw JM, Farrall AJ, Perry D, von Kummer R, Mielke O, Moulin T, Ciccone A, Hill M, for the Acute Cerebral CT Evaluation of Stroke Study (ACCESS) Study Group. Factors influencing the detection of early computed tomography signs of cerebral ischemia. An internet-based, international multiobserver study. Stroke. 2007;38:1250-6. http://dx.doi.org/10.1161/01.STR.0000259715.53166.25
- Wardlaw JM, von Kummer R, Farrall AJ, Chappell FM, Hill M, Perry D. A Large web-based observer reliability study of early ischaemic signs on computed tomography. The Acute Cerebral CT Evaluation Of Stroke Study(ACCESS). PLoS ONE. 2010;5:e15757. http://dx.doi.org/10.1371/journal.pone.0015757
Participation
ACCESS helps you to learn about how to read acute stroke CT scans. It has been used for training:- Third International Stroke Trial (IST-3) centres
- IST-3 expert scan reading panel members
- British Society of Neuroradiologists (BSNR) doctors in training
- British Association of Stroke Physicians (BASP) doctors in training
Participation is eligible for CPD / CME.
If you are introducing a new thrombolysis service or are likely to be working in a unit where you will see many acute stroke patients, & you feel that your scan reading skills are either rusty or have never been developed in the first place, then completing ACCESS is a quick way of helping to bring yourself up to speed.
Key findings
Data from ACCESS have been used to understand ways of improving observer confidence in interpreting hyperacute stroke CT scans. For example:- observers rarely see early infarcts signs that are not present (i.e. the false positive rate is low)
- the most reliably recognised sign is the hyperattenuated artery
- more experienced observers read scans more slowly
- taking longer to read scans improves observer performance
- old lesions are distracting because they draw your attention away from acute lesions
- use of any visual rating scale helps improve observer performance
Thanks
We'd like to thank everybody who has contributed to this work so far. Hopefully you have found it to be beneficial to your practice.Please recommend ACCESS to your friends and colleagues.
Links & other information
- Register for ACCESS here
- Login to ACCESS here
- Notes about ACCESS for participants
- Take the BASP CT Training Lecture beforehand here
- Integrate imaging training with STARS Thrombolysis Masterclass
- ECCITING - Edinburgh Criteria for CAA-associated ICH Training
- Please link to the short url for the Acute Cerebral CT Evaluation of Stroke Study (ACCESS) webpage:
No comments:
Post a Comment