Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 32,461 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke. DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
In the article they discussed using 5 volunteers(unknown if any were disabled) to test it, so maybe not for us. You'll have to ask your doctor where this P300 wave originates from to see if your area was dead or damaged.
One word, 'care' tells me very explicitly that the WSO isn't even trying to solve stroke and get all survivors 100% recovered. This is an organization that is all about the failed status quo and obviously has NO LEADERSHIP ON STROKE. They need to be destroyed and run by survivors. 57 minute video; TLDL(Too long, didn't listen) and it wouldn't have said anything useful anyway.
People readily adapt established gait patterns to minimize energy use
People converge on new energetic optima within minutes, even for small cost savings
Updated predictions about energetically optimal gaits allow re-convergence within seconds
Energetic cost is not just an outcome of movement, but also continuously shapes it
Summary
People prefer to move in ways that minimize their energetic cost [1, 2, 3, 4, 5, 6,7,8,9]. For example, people tend to walk at a speed that minimizes energy use per unit distance [5,6,7,8] and, for that speed, they select a step frequency that makes walking less costly [3,4,6,10,11,12]. Although aspects of this preference appear to be established over both evolutionary [9,13, 14, 15] and developmental [16]
timescales, it remains unclear whether people can also optimize
energetic cost in real time. Here we show that during walking, people
readily adapt established motor programs to minimize energy use. To
accomplish this, we used robotic exoskeletons to shift people’s
energetically optimal step frequency to frequencies higher and lower
than normally preferred. In response, we found that subjects adapted
their step frequency to converge on the new energetic optima within
minutes and in response to relatively small savings in cost (<5%).
When transiently perturbed from their new optimal gait, subjects relied
on an updated prediction to rapidly re-converge within seconds. Our
collective findings indicate that energetic cost is not just an outcome
of movement, but also plays a central role in continuously shaping it.
Results
That
people prefer to move in energetically optimal ways has been
established for decades and now represents a central principle of
movement science [1, 17, 18].
But the processes by which people discover their optimal patterns are
not clear. Much theorizing has focused on optima being established over
evolutionary timescales, through changes to body shape, muscle action,
and the hardwiring of neural circuitry [9, 13, 14, 15].
Energy optimization may also occur over the course of a lifetime, as
years of experience could allow people to learn the optimal way to move
in familiar situations and allow training to tune physiology to be more
economical [16].
An additional hypothesis—one that underpins many modern theories of
motor control—is that people can adjust their movements to continuously
optimize energetic cost [15, 19, 20, 21, 22, 23].
Only recently has energetic cost been assessed during standard
adaptation paradigms, and it was indeed found that cost was lower after
adaptation than before in both reaching and walking tasks [23,24].
These studies, while tantalizingly suggestive, were not designed to
test whether energetic cost minimization was a control objective of the
central nervous system, leaving the possibility that the measured
reductions in energetic cost were correlated with alternative nervous
system goals, such as stability, accuracy, or force minimization [25, 26, 27, 28].
Here
we directly address the continuous optimization hypothesis using
robotic exoskeletons to create novel energetic landscapes and then test
whether walking subjects adopt the necessary gait adaptions to find new
optima. Of all possible energetic landscapes, we chose to manipulate the
relationship between step frequency and energetic cost because step
frequency is a fundamental characteristic of gait, people have strong
preferences for particular step frequencies, and these preferred
frequencies are energetically optimal [10, 11].
We manipulated the relationship using lightweight robotic exoskeletons
to apply torques that resisted the motion of the knee joints (Figures 1A
and 1B ). To shift the energetic optimum to lower step frequencies, we
had the exoskeleton controller use a “penalize-high” control function
that applied a resistive torque, and therefore an added energetic
penalty, that was minimal at low step frequencies and increased as step
frequency increased (Figures 1C, 1D and S1).
To shift the energetic optimum to higher step frequencies, we used a
“penalize-low” control function, in which the slope of the penalty was
reversed (Figures 1C, 1D and S1).
The control functions were designed to create a clear energetic
gradient for step frequencies in the neighborhood of subjects’ initial
preferred step frequency, yet keep all resistive torques low enough to
allow relatively natural gaits. To distinguish between energetic cost
optimization and simply minimizing the resistive torque applied to the
limb, we also strived to design the control functions such that the
energetic cost optima occurred at step frequencies distinct from those
that minimized exoskeleton resistive torque. It is not possible to
design control functions that specifically rule out all alternative
objectives to energetic cost minimization. But to be indistinguishable
from energy minimization, optimization of these alternative objectives
would need to yield step-frequency adaptations in the same directions,
and by about the same magnitudes, as those predicted by our novel
energetic landscapes.
Natural Gait Variability Does Not Reliably Initiate Optimization
We
first sought to determine whether our subjects would adapt to a new
energetically optimal step frequency given limited experience with the
novel energetic landscape and without being perturbed away from their
natural gait. Subjects were assigned to both the penalize-high and
penalize-low control functions, in random order, on two separate testing
days. On each day, during an initial baseline trial, subjects first
walked for 12 min while wearing the exoskeletons, but with the
controller turned off (Figure 2A,
baseline). This allowed us to determine their “initial preferred step
frequency,” which we defined from the final three minutes of walking.
All walking took place on an instrumented treadmill (FIT, Bertec
Corporation) at 1.25 m/s, and we measured step frequency from treadmill
foot contact events. All subjects appeared to settle into a steady-state
step frequency within 9 min. On average, subjects walked at 1.8 ±
0.1 Hz (mean ± SD), and from step to step subjects’ step frequency
varied about this average by 1.1% ± 0.3% (mean ± SD). We then turned the
controller on, resulting in an applied resistive torque that was
dependent on step frequency, and the subjects walked for an additional
12 min (Figure 2B, first adaptation). During this time, subjects showed no adaptation in step frequency (penalize-high: p = 4.3 × 10−1; penalize-low: p = 4.4 × 10−1; Figure 3A).
They continued to walk at their initial preferred step frequency even
though we designed the controller such that minor adjustments to step
frequency would result in a more economical gait.
Broad Experience with the Energetic Landscape Initiates Optimization
We
next gave our subjects experience with the novel energetic landscape
across a wide range of step frequencies and then once again looked for
adaptations toward the novel energetic minima. This was accomplished by
instructing subjects to self-explore walking with high and low step
frequencies, as well as to match their steps to different steady-state
and sinusoidally varying metronome tempos (Figure 2C, exploration). After this 15 min exploration period, subjects were again allowed to self-select their step frequency (Figure 2D,
second adaptation), and we found that subjects immediately made large
adaptations in step frequency toward the energetic minima (Figure 3A).
To robustly determine whether this was a new preferred step frequency,
we had subjects match a metronome tempo for 6 min that perturbed them
toward both higher resistive torques (penalize-high: +10%; penalize-low:
−10%) and lower resistive torques (penalize-high: −10%;
penalize-low: +10%) (Figure 2D,
second adaptation). After each perturbation, subjects were allowed to
self-select their step frequency for another 12 min, and we found that
they returned to a step frequency that was shifted toward the energetic
optima (Figure 3).
We defined the average of the final 3 min of self-selected step
frequency after the last perturbation as the “final preferred step
frequency.” On average, when given the penalize-high control function,
subjects decreased their step frequency by 5.7% ± 3.9% (mean ± SD),
whereas for the penalize-low control function, subjects’ step frequency
increased by 6.9% ± 4.3%. These final preferred step frequencies were
distinct from what subjects initially preferred (penalize-high: p =
1.3 × 10−3; penalize-low: p = 6.2 × 10−4), and
they were distinct from those that would minimize the resistive torque
being applied to the limb (penalize-high: p = 5.2 × 10−5; penalize-low: p = 2.4 × 10−4).
We
next sought to determine how our subjects’ final preferred step
frequency compared to the energetically optimal step frequency by
mapping their energetic landscape. We again turned the controller on and
had subjects walk to steady-state metronome tempos for 6 min each (Figure 2E,
cost mapping), including tempos about the initial preferred step
frequency (+5%, 0%, −5%) and about the final preferred step frequency
(+5%, 0%, −5%). We measured metabolic energetic cost using respiratory
gas analysis equipment (VMax Encore Metabolic Cart, ViaSys). As
hypothesized, our subjects had indeed increased or decreased their
self-selected step frequency, whichever was required by the new
landscape, to converge on the new energetic optima (Figure 4).
These adaptations were to achieve relatively small cost savings. The
energetic cost at the final preferred step frequency was 8.1% ± 7.0%
lower than the energetic cost at the initial preferred step frequency
for the penalize-high control function (p = 4.1 × 10−3) and 4.0% ± 3.8% lower for the penalize-low control function (p = 9.7 × 10−3).
Subjects achieved most of the costs savings immediately after the
exploration period, yet they continued to fine-tune their step frequency
for vanishingly small energetic savings (Figure 3).
Evaluation of the energetic cost at the final preferred step
frequencies, and at step frequencies on either side of the final values,
suggested that subjects converged to, or at least near, their minimum
costs; no further cost savings appear to be gained by additional
adjustments to preferred step frequency (Figures 4B and 4F).
Gait Adaptations Use Updated Predictions of Energetically Optimal Gaits
After
perturbations using the metronome tempos, our subjects converged toward
their new preferred step frequency within seconds (Figures 3B
and 3C). In cases where subjects were held at metronome tempos that
resulted in high resistive torques (penalize-high: +10%; penalize-low:
−10%) and then released, they immediately bypassed their initial
preferred step frequency, which was now energetically suboptimal, to
quickly converge on the new preferred and energetically optimal step
frequency. All subjects bypassed the initial preferred step frequency in
less than 10 s. When held at metronome tempos that resulted in low
resistive torques (penalize-high: −10%; penalize-low: +10%) and then
released, subjects actually elected to increase the resistance on their
limb, again within seconds, in order to reach the energetic optima. We
have previously argued that the timescale of such rapid adaptations to
energetically optimal gaits requires the prediction of energetic cost,
rather than its direct optimization [
].
That subjects rapidly converged on new energetic minima indicates that
subjects had updated their prediction of the optimal gait for each
control function. This was also observable when the high or low penalty
was removed for a final 12 min (Figure 2D,
second adaptation); subjects’ step frequency remained shifted toward
the control function optima for minutes despite a return to the natural
energetic landscape and its former energetically minimal gait (Figure 3).
Discussion
Motor
variability has traditionally been thought of as an inevitable, if not
potentially burdensome, consequence of imperfect neural control.
However, recent findings have reframed motor variability as an asset—one
that can facilitate and enhance motor learning. For example, songbirds
are able to leverage small variations in their pitch to continuously
optimize their song performance [30], and humans actively reshape the structure of their motor output variability to elicit faster learning of reaching tasks [31].
We found that natural gait variability did not initiate the
optimization process in our particular experiment. Instead, subjects
persevered at their initial preferred step frequency after the
controller was turned on, even though minor adjustments to step
frequency would have resulted in a more economical gait. Only after the
exploration period, which enforced large variations in step frequency,
did subjects demonstrate large adaptations toward the new energetic
optima (Figure 3A).
One possible explanation for this need for exploration is that people’s
natural variability in step frequency is not expansive enough to
elucidate a clear energetic gradient. Alternatively, people may not
initiate optimization based on energetic gradients, but may instead
require that exploration provide explicit experience with the new
optimum in order for people to adapt to it. In either case, these may be
smaller issues when walking in a real-world setting because natural
changes in speed and terrain may generate the variability in gait
required to either initiate optimization or provide experience with new
optimal movement patterns.
Our
findings suggest that new optima are encoded in an updated prediction of
the energetically optimal gait and leveraged to rapidly select
preferred step frequency [29, 32].
When subjects were held away from their preferred step frequency using a
metronome and then released, they returned to their new preferred step
frequency within seconds (Figures 3B
and 3C). These adjustments are likely too fast to be governed by blood
gas sensors, muscle metaboreceptors, and other known direct sensors of
energetic cost, which are known to be relatively slow [33, 34].
Furthermore, optimization itself tends to be slow if its algorithm
requires the time consuming steps of averaging and iterative convergence
[29].
That the subjects made an updated prediction of the optimal gait is
also observable at the end of the experiment, when subjects’ preferred
step frequency remained shifted toward the control function optima for
minutes despite a return to the natural energetic landscape (Figure 3B). This aftereffect differs from the aftereffects seen in force-field reaching or split-belt walking paradigms [35, 36],
where the resulting trajectories are mirror images of those observed
when initially exposed to the novel environment. When our controller was
turned off, rather than displaying this overshoot and rapid correction,
we instead found that subjects adjusted to the rapid reduction in
exoskeleton torque and persevered at the optimum for the previous
adaptation. These aftereffects appeared to last an order of magnitude
longer than those typically reported in other walking paradigms [36, 37, 38, 39].
This implies that sensorimotor predictions about energetically optimal
movements are particularity resilient, at least without an exploratory
phase to initiate re-optimization. The slow step-frequency adjustments
during re-adaptation are not in conflict with the fast adjustments
observed when subjects are released from a metronome after exploring
their new energetic landscape. During the latter, subjects are able to
quickly predict their optimal gait within a now-familiar energetic
landscape. But the former requires optimization within a new energetic
landscape, or at least recognition that this new landscape is familiar.
Despite
a lifetime of experience walking under natural conditions, people
readily adapted established motor programs to minimize energy
expenditure, and they did so for quite small energetic gains. It is
sensible that motor programs remain malleable because people’s bodies,
and the tasks they are presented with, can change. Continuous energetic
optimization benefits motor adaptation by keeping movements close to
energetically optimal, helping people to efficiently adapt to changing
terrains, compensate for injury or motor deficits, and learn new tasks.
What a fucking waste. There should never be a need for these simple review articles.
An absolute waste of time because our fucking failures of stroke associationshave not set up a database of all stroke research with instructions to update as new info comes in.
In
the United States, strokes are known to kill over 140,000 people every
year and effect mobility in more than 50 percent of stroke survivors
(Centers for Disease Control and Prevention, 2020). It is a debilitating
disease that befalls when blood vessels transporting nutrients to the
brain are disrupted by a blood-clot or rupture of a vessel. While many
rehabilitative therapies are available to those who have suffered from a
stroke, there is one therapy that may benefit stroke survivors more
than just conventional therapies. Mirror therapy (MT), a therapy that
utilizes a mirror box to create an optical illusion, may be one way to
help survivors to recover their lost motor functions. MT can aid
rehabilitation by using a mirror to produce a reflection of a person’s
unaffected limb in place of the affected limb when performing tasks.
When the unaffected extremity is shifted, the mirror image allows the
brain to believe that the affected limb is moving. These optical
illusions allow the patients to feel as if their two extremities are
moving symmetrically. This literature review focuses on how mirror
therapy is utilized in practice today and if it should be incorporated
as a conventional therapy for stroke rehabilitation. Peer reviewed
journal articles have been dissected from the databases CINAHL Complete
and MEDLINE. Through the review process, it was revealed that while
mirror therapy on its own did not show any significant changes in
overall motor functionality, mirror therapy in combination with
conventional therapy has the potential to have statistically significant
results.
Obviously it is your responsibility to be able to do this while in a locked-in state otherwise you may be cut off from rehab. Not your doctor's responsibility, YOURS. You do know that this will never get to your hospital.
Does your hospital have an
employee whose only function is to scan for stroke related research and
information and create rehab protocols and distribute them to the staff?
If not, YOU HAVE A FUCKING INCOMPETENT HOSPITAL.
A
simple "sniff test", trialled by researchers at the University of
Cambridge, could help doctors diagnose and determine treatment for
patients who are in a vegetative state or have minimal consciousness
following brain injuries.
Patients
in a vegetative state can open their eyes, wake up and fall asleep
regularly and have basic reflexes but don't show signs of awareness.
Minimally conscious patients can have periods where they can show signs of awareness or respond to commands.
'Sniff test'
"The
accuracy of the sniff test is remarkable - I hope it will help in the
treatment of severely brain injured patients around the world," said Dr
Anat Arzi, a researcher in the University of Cambridge's Department of
Psychology and the Weizmann Institute of Science Israel, who led the
study.
Results published in the journal Nature
revealed 100 per cent of patients who reacted to the sniff test went on
to regain consciousness and more than 91 per cent of these patients
were still alive three and a half years after injury.
Doctors
often find it difficult to determine a patient's state of consciousness
after a severe brain injury but accurate diagnosis is critical for
treatment strategies, such as pain management, and for end-of-life
decisions.
Sense of smell relies on structures deep within the brain and works whether we are awake or asleep.
Accurate diagnosis
The
brain automatically changes the way we sniff in response to different
smells, with shorter and shallower breaths for unpleasant smells.
Scientists
carried out the ‘sniff test’ on 43 patients with severe brain injury,
presenting them different jars of smell for five seconds.
One jar contained a pleasant smell of shampoo, one an unpleasant smell of rotten fish, and one had no smell at all.
Each
jar was presented ten times in a random order and the volume of air
sniffed by the patient was measured using a nasal cannula.
Jars of smell
Trials were carried out on patients with minimal consciousness and in a vegetative state (Photo: Getty)
Researchers
found minimally conscious patients inhaled significantly less in
response to smells but did not discriminate between nice and nasty.
These
patients also modified their nasal airflow in response to the jar with
no smell, suggesting they were aware of the jar or anticipated a smell.
Vegetative
state patients had a more varied response, some did not change their
breathing in response to the smells but others did.
A
follow-up investigation three and a half years later found more than
91% of the patients who had a sniff response shortly after injury were
still alive, but 63% of those who had showed no response had died.
Sniff response
"We
found that if patients in a vegetative state had a sniff response, they
later transitioned to at least a minimally conscious state”, said Dr
Arzi, “In some cases, this was the only sign that their brain was going
to recover - and we saw it days, weeks and even months before any other
signs.”
Dr Tristan
Bekinschtein, from the University of Cambridge's Department of
Psychology who was also involved in the study, said:"This new and simple
method to assess the likelihood of recovery should be immediately
incorporated in the diagnostic tools for patients with disorders of
consciousness."
This biomarker research is status quo defeatism. LEADERS CHANGE THE STATUS QUO, ARE YOU A LEADER OR A MOUSE?
Nothing here will get any survivor closer to recovery. Useless.
Oops, I'm not playing by the polite rules of Dale Carnegie, 'How to Win Friends and Influence People'.
Politeness
will never solve anything in stroke. Yes, I'm a bomb thrower and proud
of it. Someday a stroke "leader" will ream me out for being negative, I
look forward to that day.
Stroke — Cassidy JM, Wodeyar A, Wu J, et al. | April 29, 2020
This study was intended to explore hypotheses relating
electroencephalography measures, including low-frequency oscillations,
to injury and motor recovery post stroke. Researchers examined the
association that electroencephalography measures (power and coherence
with leads overlying ipsilesional primary motor cortex [iM1]) had with
injury and motor status, targeting on delta (1–3 Hz) and high-beta
(20–30 Hz) bands. The results of this study exhibit that delta band
coherence with iM1 related to greater injury and poorer motor status
subacutely, while delta band power related to greater injury and better
motor status chronically. The data showed that after stroke,
low-frequency oscillations reflect both injury and recovery and may be
beneficial biomarkers in stroke recovery and rehabilitation.
I SEE ABSOLUTELY NO PROGRESS IN STROKE. NONE. ZIP. NADA. Enlighten me how the fuck this meme came to represent World Stroke Day a few years ago. And May is Stroke Awareness month. You are all aware that everything in stroke is a complete failure and you are shouting that to the rooftops? For those not enlightened these two links prove how fucking bad stroke is;All the problems in stroke, or this nihilism list.
You need this progress in Parkinsons because of this:
We knew this Parkinson’s Awareness Month would be unlike
any other. Pivoting to support the worldwide Parkinson’s community
through this challenging time, The Michael J. Fox Foundation continued
to work with urgency and determination, albeit remotely, to move our
programs forward.
We sourced expert voices from neurology, epidemiology, public policy and
infectious disease to provide practical, Parkinson’s-specific advice
and you logged on, signed up and tuned in. We shared ways to participate
in research from home through our online clinical study Fox Insight, and over 2,000 new participants enrolled in April alone.
Ultimately, our obligation is to keep Parkinson’s research moving forward with as little disruption as possible.
Not only is mobilizing our engaged patient community critical, so is
maintaining the flow of vital support for ongoing research, and
grantmaking for projects that can progress remotely, such as data
analysis. Just this week, we announced $10.4 million in funding for 72 new research projects.
Parkinson’s Awareness Month ends today but the supply of timely information and updates will not. Progress in Parkinson’s research is continuing,
and we pledge to uphold our commitment to transparency and
accountability as we respond to patients’ and scientists’ needs during
this time.
We felt your presence this month — even from afar — and remain hopeful knowing that you’re here with us until Parkinson’s isn’t.
But you never say how fast you are. Can you even compete with these other fast diagnosis tools? It still seems to require a neurologist which I think needs to be removed from the equation. But since I'm not medically trained I will just shut up and be quiet, your stroke medical professionals will explain how fast you need to be treated to get 100% recovery and EXACTLY how this technology will do that.
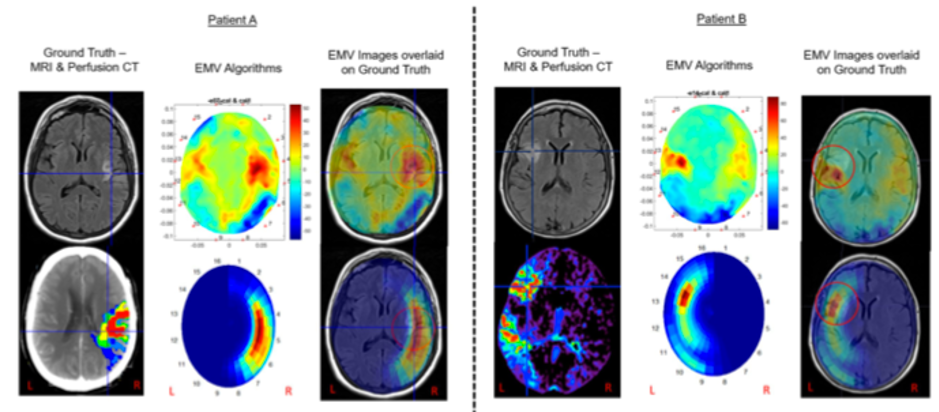
EMVision Medical Devices Ltd (EMV), a company that
took part in Switzer’s Small and Micro Cap Investor Day on 3 March 2020,
has released new information on the ASX, releasing the preliminary
images from their clinical trial.
READ MORE: https://switzer.com.au/the-experts/sophia-katsinas/a-taste-of-switzers-small-and-micro-cap-investor-day-event/
EMVision aims
to revolutionise the imaging of strokes and traumatic brain injuries through
the development and commercialisation of portable medical imaging technology.
Its first brain scanner is a commercial product at a manageable price
that allows for quick, efficient and scalable brain scanning.
EMVision’s scanners display strong correlation with CT and MRI scanners.
The clinical assessment results show these similarities that produce
the detection and localisation of abnormal brain tissue. The advantage
of the EMV images, as shown in the images below, is that the EMV images
distinguish abnormal brain tissue from healthy brain tissue, which
apparently is often less clear in CT scans.
The technology is currently in the clinical trial stage, and the
company has its hat in the ring for a share in a $50 million+ Medical
Research Future Fund Grant pledged with the Australian Stroke Alliance.
Co-chairs of the
Australian Stroke Alliance and past presidents of the World Stroke
Organization, Professors Stephen Davis AM and Geoffrey Donnan AO said the
results of the trial were “promising”. Professor Davis commented “These early
images are clinically promising, clearly showing the effects of ischemic stroke
in the same region as the gold standard imaging methods”. While Professor
Donnan said “the lightweight portability of the device makes it a potential
candidate for emergency stroke imaging in the prehospital setting.”
The machine
will be accessible in the prehospital triage stage, meaning parademics and
on-the-scene medical professionals will be able to identify the issue earlier,
allowing for more targeted treatment options.
EMVision CEO,
Dr Ron Weinberger was pleased with the result, saying “We are confident that as
we continue to process further stroke patient data, we will demonstrate our
unique value proposition to meet a major unmet clinical need in rapid and
portable stroke diagnosis and monitoring.”
GripAble was out there way back in October 2016, HOW FUCKING INCOMPETENT DOES YOUR HOSPITAL HAVE TO BE TO NOT DO ANYTHING WITH HAND RECOVERY IN 3.5 YEARS?
S/he has had three years to come up with prevention protocols. Why the hell aren't there any?
Laziness? Incompetence? Or just don't care?
No leadership? No strategy? Not my job? The board of directors didn't
tell them that totally solving stroke was their job, not just lazily
relying on the status quo?
Researchers
at Karolinska Institutet and the University of North Carolina have
mapped out the cell types behind various brain disorders. The findings
are published in Nature Genetics and offer a roadmap for the
development of new therapies to target neurological and psychiatric
disorders. One interesting finding was that cells from the gut's nervous
system are involved in Parkinson disease, indicating that the disease
may start there.
The
nervous system is composed of hundreds of different cell types with very
different functions. It is vital to understand which cell types are
affected in each disorder so as to understand the causes of the
disorders and, ultimately, develop new treatments.
Researchers
have now combined mice gene expression studies with human genetics to
systematically map cell types underlying various brain disorders,
including Parkinson disease, a neurodegenerative disorder with cognitive
and motor symptoms resulting from the loss of dopamine-producing cells
in a specific region of the brain.
Several unexpected findings
“As
expected, we found that dopaminergic neurons were associated with
Parkinson disease. More surprisingly, we found that enteric neurons also
seem to play an important role in the disorder, supporting the
hypothesis that Parkinson disease starts in the gut,” says one of the
study’s main authors Patrick Sullivan, Professor at the Department of
Medical Epidemiology and Biostatistics at Karolinska Institutet and
Yeargan Distinguished Professor at the University of North Carolina.
When
the researchers analysed differences in brain tissue from healthy
individuals and people with Parkinson disease at different stages of the
disease, they made another unexpected discovery. A type of support cell
in the brain called oligodendrocytes were found to be affected early
on, suggesting that they play a key role in the early stages of the
disease.
Attractive target for new therapies
“The fact that the animal studies pointed us to oligodendrocytes and
that we were then able to show that these cells were also affected in
patients suggests that the results may have clinical implications,” says
Jens Hjerling-Leffler, research group leader at the Department of Medical Biochemistry and Biophysics at Karolinska Institutet and the other main author of the study.
The oligodendrocytes appear to be affected even before the loss of dopaminergic neurons.
Advertisement
“This makes them an attractive target for therapeutic interventions in Parkinson disease,” says Julien Bryois,
researcher at the Department of Medical Epidemiology and
Biostatistics at Karolinska Institutet and one of the first authors of
the study.
The study was financed by the Swedish Research Council, StratNeuro,
the Wellcome Trust, the Swedish Brain Foundation, the Swiss National
Science Foundation, the US National Institute of Mental Health, and the
Psychiatric Genomics Consortium.
Patrick Sullivan reports that he is currently a member of the
pharmaceutical company Lundbeck’s advisory committee and that he has
received grants from them. For the past three years he has been a member
of Pfizer’s scientific advisory board and received fees from Element
Genomics and Roche. Co-author Cynthia Bulik has received grants from
Shire and is a member of their scientific advisory board. She is also an
author and recipient of royalties from both Pearson and Walker.
Well the only animals I meet are deer in the woods I do my daily walk in and they are usually 50 yards away and running besides, 9 today. Turkeys are rarely seen and the squirrels run to the back side of the tree. Tomorrow will be morel hunting after today's rain and the warm weather, they may be popping soon.
The Centers For Disease Control and Prevention is now recommending
that cats, dogs and other animals keep the same social distancing as
recommended for humans.
The recommendation was made after a small
number of animals -- including dogs and cats -- were reported to test
positive for COVID-19 after they had had close contact with a person who
had the disease.
While the first coronavirus infections were
thought to be linked to a live animal market, the virus is now
"primarily spreading from person to person," the CDC said in a statement
on its website. "At this time, there is no evidence that animals play a
significant role in spreading the virus that causes COVID-19."
However,
it now appears that the virus can spread from people to animals.
Earlier this month, a Malayan tiger in the Bronx Zoo tested positive for
the virus. Last week, at least two cats in New York tested postive. Now
the CDC is reporting "a small number of pets, including cats and dogs
... to be infected with the virus that causes COVID-19."
It
advises pet owners to avoid letting their pets interact with people or
animals outside your household. Cats should be kept indoors if possible.
Dogs should be walked on a leash and kept at least 6 feet away from
other animals or people. It's best to avoid dog parks and other public
places where lots of people and dogs gather.
And if someone in your house becomes sick, they should isolate themselves from everyone in the house, including any pets.
(c)2020 Star Tribune (Minneapolis)
So you obviously missed the point that you learn faster by having errors and correcting them. Good thing you aren't training toddlers to walk, they would never get to perfection and actually walk.
Compensations
are commonly observed in patients with stroke when they engage in
reaching without supervision; these behaviors may be detrimental to
long-term functional improvement. Automatic detection and reduction of
compensation cab help patients perform tasks correctly and promote
better upper extremity recovery.
Objective
Our
first objective is to verify the feasibility of detecting compensation
online using machine learning methods and pressure distribution data.
Second objective was to investigate whether compensations of stroke
survivors can be reduced by audiovisual or force feedback. The third
objective was to compare the effectiveness of audiovisual and force
feedback in reducing compensation.
Methods
Eight
patients with stroke performed reaching tasks while pressure
distribution data were recorded. Both the offline and online recognition
accuracy were investigated to assess the feasibility of applying a
support vector machine (SVM) based compensation detection system. During
reduction of compensation, audiovisual feedback was delivered using
virtual reality technology, and force feedback was delivered through a
rehabilitation robot.
Results
Good
classification performance was obtained in online compensation
recognition, with an average F1-score of over 0.95. Based on accurate
online detection, real-time feedback significantly decreased
compensations of patients with stroke in comparison with no-feedback
condition (p < 0.001). Meanwhile, the difference between audiovisual and force feedback was also significant (p < 0.001) and force feedback was more effective in reducing compensation in patients with stroke.
Conclusions
Accurate
online recognition validated the feasibility of monitoring
compensations using machine learning algorithms and pressure
distribution data. Reliable online detection also paved the way for
reducing compensations by providing feedback to patients with stroke.
Our findings suggested that real-time feedback could be an effective
approach to reducing compensatory patterns and force feedback
demonstrated a more enviable potential compared with audiovisual
feedback.
Background
Stroke is the leading cause of long-term disability in adults worldwide [1], and many post stroke patients suffer from varying degrees of upper extremity motor dysfunction [2]. Skilled reaching is an important aspect of upper limb motor ability but is impaired after stroke [3, 4].
Patients with stroke usually develop adaptive compensatory patterns,
particularly by recruiting excessive trunk or shoulder movements during
reaching [5, 6].
The use of compensatory motions could be beneficial for an immediate
improvement in function; however, such a functional improvement occurs
because of a reinforcement of compensation instead of true motor
recovery [7].
Patients with stroke who commonly use compensatory strategies may form
nonoptimal motion patterns, hindering long-term recovery of their
impaired arms [8, 9].
Previous studies have demonstrated that reducing compensatory patterns
has the potential to improve the final functional outcome. Improvements
were accompanied by lager active joint range [8], higher FMA-UE score [10] and recovery of lost motor patterns [7].
Therefore, therapists correct undesired compensatory motions when they
supervise therapeutic exercises. However, stroke patients perform many
exercises without supervision, such as home therapy, which highlights
the need to detect and reduce compensation in unsupervised rehabilitation
[10].
Automatic
detection of compensation can ensure subsequent intervention to prompt
the patient into the correct pose. Previous studies have evaluated the
feasibility of sensor-based and camera-based systems to detect
compensation without the supervision of a therapist [11,12,13,14,15].
However, camera systems are not appropriate for application in clinical
or home settings, which face challenges such as object obstruction,
complex setups and privacy [13, 16].
Sensor-based systems suffer from inducing unnatural motions due to the
attachment of sensors. Moreover, the reliability of the outcome
estimates from these sensors is still a challenge for researchers [14, 16].
While the detection of compensatory patterns still lacks a simple,
unobtrusive and practical method, we have proposed a pressure
distribution-based compensation detection system [17, 18].
With a pressure mattress mounted on the chair, participants performed
seated reaching tasks, and the pressure distribution data were recorded.
Several features were extracted from the pressure distribution data
that reflected the information for different kinds of compensatory
motions. Different models were applied to recognize compensatory
patterns and achieved excellent offline recognition accuracy. Our
previous studies pave the path toward detecting compensation based on
pressure distribution data and machine learning methods. However, there
is still a gap between online and offline detection performance, and few
studies on the real-time detection of compensation have been reported.
To our knowledge, no previous study has evaluated the feasibility and
validity of detecting compensatory motions based on pressure
distribution data and machine learning methods in real time. Therefore,
the purpose of this study is to investigate whetherthe pressure
distribution-based method can be implemented in the real-time monitoring
of compensatory motions in patients with stroke.
Based on the real-time detection of compensation, various feedback strategies, in the form of visual [19, 20], auditory [21, 22], or force feedback [23],
were provided to patients with stroke to modify their motion patterns.
However, there is still no consensus on the kind of feedback modalities
that would be effective in reducing compensation. In this study, virtual
reality (VR) technology was employed to provide audiovisual feedback,
while a rehabilitation robot was employed to provide force feedback.
This pilot study aimed to investigate whether the compensation of stroke
survivors during reaching can be reduced by audiovisual and force
feedback and to examine whether one feedback method is superior to the
other.
Therefore,the main contributions of this paper are as follows:
1)The
implementation and validation of the presented compensation-detecting
method using pressure distribution data and machine learning algorithms
in real time;
2)The
use of virtual reality and a rehabilitation robot to reduce
compensatory motions in patients with stroke during reaching tasks; and
3)The comparison of audiovisual and force feedback for reducing compensation.
Methods
Participants
Eight
poststroke subjects were recruited from the Third Affiliated Hospital,
SUN Yat-sen University. A summary of the participants’ demographics was
provided in Table 1.
Ethical approval was obtained from the Guangzhou First People’s
Hospital Department of Ethics Committee. All participants reviewed and
signed an informed consent form prior to entering the study.
Table 1 Demographic and clinical data for participants with stroke
Participants
were included if they had experienced their first-ever stroke, if they
were either in the subacute (between 1 to 6 months poststroke) or
chronic (over 6 months poststroke) stage of recovery, if they were able
to remain in a sitting posture (without back or arm rests) for at least
10 min and if they were able to perform the required motions.
Participants were excluded from the study if they had the following:
upper limb pain > 4/10 on a visual analogue scale (VAS) [24]; upper limb spasticity > 2 on the Modified Ashworth Scale (MAS) [25]; Mini-Mental State Examination (MMSE) score ≤ 23 [26]; or visual spatial neglect based on clinical judgment.












00958-6&id=gr1.jpg){kind=link}
00958-6&id=gr2.jpg){kind=link}
00958-6&id=gr3.jpg){kind=link}
00958-6&id=gr4.jpg){kind=link}