Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 33,614 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke. DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
Friday, July 31, 2020
Passive-elastic knee-ankle exoskeleton reduces the metabolic cost of walking
Useless for us, tested in healthy subjects. And since we have NO STROKE LEADERSHIP, we have no one to ask to get this tested in stroke subjects.
Previous
studies have shown that passive-elastic exoskeletons with springs in
parallel with the ankle can reduce the metabolic cost of walking. We
developed and tested the use of an unpowered passive-elastic exoskeleton
for walking that stores elastic energy in a spring from knee extension
at the end of the leg swing phase, and then releases this energy to
assist ankle plantarflexion at the end of the stance phase prior to
toe-off. The exoskeleton uses a system of ratchets and pawls to store
and return elastic energy through compression and release of metal
springs that act in parallel with the knee and ankle, respectively. We
hypothesized that, due to the assistance provided by the exoskeleton,
net metabolic power would be reduced compared to walking without using
an exoskeleton.
Methods
We
compared the net metabolic power required to walk when the exoskeleton
only acts at the knee to resist extension at the end of the leg swing
phase, to that required to walk when the stored elastic energy from knee
extension is released to assist ankle plantarflexion at the end of the
stance phase prior to toe-off. Eight (4 M, 4F) subjects walked at
1.25 m/s on a force-measuring treadmill with and without using the
exoskeleton while we measured their metabolic rates, ground reaction
forces, and center of pressure.
Results
We
found that when subjects used the exoskeleton with energy stored from
knee extension and released for ankle plantarflexion, average net
metabolic power was 11% lower than when subjects walked while wearing
the exoskeleton with the springs disengaged (p = 0.007), but was 23% higher compared to walking without the exoskeleton (p < 0.0001).
Conclusion
The
use of a novel passive-elastic exoskeleton that stores and returns
energy in parallel with the knee and ankle, respectively, has the
potential to improve the metabolic cost of walking. Future studies are
needed to optimize the design and elucidate the underlying biomechanical
and physiological effects of using an exoskeleton that acts in parallel
with the knee and ankle. Moreover, addressing and improving the
exoskeletal design by reducing and closely aligning the mass of the
exoskeleton could further improve the metabolic cost of walking.
Introduction
Reducing
the metabolic cost of walking through use of assistive devices such as
exoskeletons would allow humans to walk further with less effort and
fatigue and could allow those with physical disabilities to be able to
walk. The idea of creating mechanical devices to assist human movement
and reduce metabolic cost has been around since the year 1890 [1].
During the twentieth century, many scientists have focused their
efforts on creating mechanical devices that reduce the metabolic cost of
human movement [2],
and during the last decade, use of an unpowered passive-elastic
exoskeleton has reduced the metabolic cost of walking compared to
walking without an exoskeleton by improving efficiency (quotient of
mechanical and metabolic power) [3, 4].
Distinct
biomechanical tasks needed to walk, such as supporting body weight and
redirecting/accelerating the center of mass, require leg muscle force
and work, and thus incur a metabolic cost. The single limb support phase
of walking has been modelled as an inverted pendulum [5,6,7]. In this model, the body’s mass is represented by a point mass and the stance leg by a rigid massless strut [6, 7].
During the single support phase, mechanical energy is conserved through
the phasic exchange of kinetic and gravitational energy. However, the
muscles of the leg must produce force to support body weight during
single support and thus require metabolic energy [8].
The muscles of the leg must also generate mechanical work to transition
body mass from step to step during the double support phase and this
incurs a greater metabolic cost than body weight support [8,9,10].
Redirecting the center of mass during the step-to-step transition
requires approximately 45% of the overall net metabolic power; whereas
supporting body weight requires approximately 28% of the overall net
metabolic power needed for steady-speed level-ground walking [8].
To facilitate walking, the muscles surrounding the ankle, knee, and hip
joints dissipate and generate mechanical work; these changes in
negative and positive energy could be exploited by a passive-elastic
exoskeleton to reduce metabolic cost.
The muscles surrounding the
ankle joint are primarily responsible for absorbing/producing power to
facilitate the redirection of the center of mass during the step-to-step
transition [11].
Over a stride, the muscles surrounding the knee joint dissipate or
absorb/store net negative mechanical power and work, whereas the muscles
surrounding the ankle and hip joints generate net positive mechanical
power and work [12].
Negative and positive peaks in joint power indicate when mechanical
energy is absorbed and generated, respectively, during a stride (Fig. 1).
Negative peak power indicates eccentric contraction of the ankle
plantar-flexor muscles from heel-strike through tibial progression, knee
extensor muscles during heel-strike, rectus femoris during late stance,
and biceps femoris during late stance (Fig. 1).
Positive power regions primarily correspond to concentric contraction
of the ankle plantar-flexor muscles during late stance, knee extensor
muscles during early stance and hip flexor muscles during early swing
phase. All these muscle contractions incur a metabolic cost. Thus, an
exoskeleton that stores energy corresponding with the eccentric
contraction of the knee extensor muscles and returns this energy during
the concentric contraction of the ankle plantar-flexor muscles could
decrease the metabolic cost of walking.
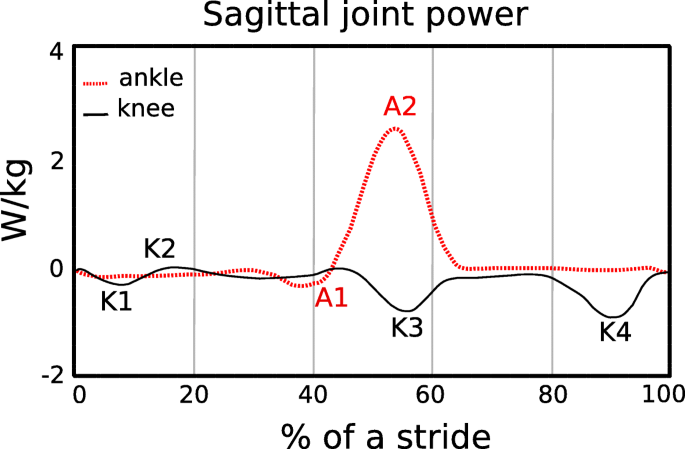
Fig. 1
Average
sagittal plane ankle (A), and knee (K) joint mechanical power during
level ground walking at 1.10 m/s over a stride for one leg, starting at
heel strike. Data are from a previous study [13].
Negative peak power regions for the ankle and knee joints are denoted
as A1 and K1, K3, and K4, respectively. Mechanical power and thus
energy, is dissipated/absorbed during negative ankle (A1) and knee (K4)
joint minimums [11].
At ~ 35–40% of the stride, the ankle plantar-flexors contract
eccentrically to control ankle joint dorsiflexion. During terminal swing
(K4), the hamstrings contract eccentrically to slow the speed of the
swinging leg and avoid knee hyperextension just prior to the subsequent
heel-strike (~ 90% of the stride). Positive mechanical power regions are
labelled as A2 and K2 and correspond to the concentric contraction of
the ankle plantar-flexors during late stance and the knee extensors
during early stance, respectively
In
order to reduce the metabolic cost of walking, use of an exoskeleton
should not alter kinematic gait parameters such as stride length and
step width, or kinetic parameters such as ground reaction forces.
Previous studies have shown that when people walk with stride lengths
and stride frequencies different from preferred, the metabolic cost of
walking increases [14,15,16].
Walking speed is the product of stride length and stride frequency. At a
fixed walking speed, the relationship between stride frequency and
metabolic cost is represented by a U–shaped curve with the minimum
metabolic cost corresponding to the preferred stride frequency [17].
Similarly, previous studies show that when humans walk with wider or
narrower step widths compared to preferred, their metabolic cost
increases [18,19,20]. Step width indicates the lateral distance between the midlines of the feet [21]. At a fixed walking speed, metabolic cost increases with the square of step width [19].
Thus, use of an exoskeleton that results in changes to stride length,
stride frequency and step width compared to preferred could increase the
metabolic cost of walking.
The development of wearable devices
such as exoskeletons has been motivated by the challenge to reduce the
metabolic cost of walking. In 1890, Nicholas Yagn conceptualized and
received a patent for the first exoskeleton for assisting walking,
running, and jumping using pneumatically powered gas bags [1].
Since then, many investigators have developed electrically powered or
battery-powered lower limb exoskeletons for medical applications,
neurorehabilitation therapy, augmentation, and military use [2, 22,23,24,25].
Most of the recent powered exoskeletons use actuators to provide
assistance at the ankle joint during powered plantarflexion at the end
of the stance phase of walking [25,26,27,28,29,30].
Specifically, use of powered exoskeletons has reduced the muscle
activity and lower limb joint work needed by the user during
level-ground walking compared to wearing the exoskeleton with the power
turned off. Together with the timing of the assistance, the weight of
these devices (12 kg to 38 kg [22])
may be one of the reasons why use of a powered exoskeleton does not
decrease metabolic cost compared to normal walking without any wearable
system [24].
With
new methodological innovations, current research shows that
exoskeletons can improve the metabolic cost of walking. Malcolm et al. [30]
used optimal actuation timing predicted by a mathematical model
combined with a tethered electrically-powered exoskeleton that assists
ankle plantarflexion, and found that use of the exoskeleton reduced the
metabolic cost of walking at 1.38 m/s by 6.0 ± 2.0% (mean ± SD) compared
to walking without the exoskeleton. Mooney et al. [25]
developed a battery-powered exoskeleton that utilizes a mathematical
model to control the magnitude of positive mechanical power provided by
the exoskeleton during ankle powered plantarflexion, and reduced
metabolic cost by 8 ± 3% compared to walking without an exoskeleton at
1.5 m/s. Thus, through the optimal timing and magnitude of applied
power, use of a powered exoskeleton can reduce the metabolic cost of
walking.
The way that an exoskeleton is attached to a person can
affect the assistance provided to the person and thus the metabolic cost
of walking. Panizzolo et al. [31]
have investigated the use of an exosuit equipped with compliant
textiles that provide assistance instead of rigid structures, such as
those used in other powered exoskeletons. This approach aimed to improve
the interface between the exoskeleton and the body [32] and reduce the mass on distal body segments to have less of an effect on metabolic cost [33, 34].
In particular, the exosuit was designed to provide assistance during
both ankle joint plantarflexion at the end of the stance phase and hip
joint flexion during the early swing phase. Using this exosuit, net
metabolic power in the powered condition was 14.2 ± 6.1% lower than in
the unpowered condition, but net metabolic power was not reduced with
respect to normal walking at 1.5 m/s.
Use of passive-elastic
exoskeletons has reduced the metabolic cost of walking by enhancing the
mechanism of elastic energy storage and return at the ankle joint, with
springs in parallel to the Achilles tendon [3, 25].
Recent studies demonstrate that storing and returning elastic energy
during the phases of ankle joint negative and positive mechanical power
can significantly reduce metabolic cost [3, 35]. Collins et al. [3]
has shown that use of a passive-elastic exoskeleton in parallel with
the ankle joint that stores and returns energy during the negative and
positive phases of ankle joint power (Fig. 1)
reduced metabolic cost by 7.2 ± 2.6% (mean ± SD) compared to walking
without an exoskeleton at 1.25 m/s. Many others have investigated how
use of a passive-elastic exoskeleton, which does not require an external
power supply and is not equipped with sensors or actuators, affects
walking [3, 36,37,38,39]. Panizzolo et al. [3]
demonstrated that it is possible to reduce the metabolic cost of
walking by more than 3% with a passive device that assists the hip joint
compared to normal walking. Rome et al. [38]
found that use of rubber bands in parallel with the hip joint can
reduce the metabolic costs of carrying loads during walking, whereas
Dean et al. [39]
has shown that the use of a two-joint passive-elastic exoskeleton that
works in parallel with the hip and knee joints can reduce the activity
of lower limb muscles compared to normal walking [39].
We
aimed to determine if a passive-elastic exoskeleton in parallel with
the knee and ankle joints could reduce the metabolic cost of walking. We
built an exoskeleton that stores energy from knee extension during the
late leg swing phase, which corresponds to negative peak knee power
(Fig. 1, K4) since it represents the greatest magnitude of energy absorption/storage during the stride [12].
Then, we designed the exoskeleton to release the energy stored from
knee extension to assist ankle powered plantarflexion, which corresponds
to positive peak ankle power during late stance (Fig. 1,
A2). We designed our experiments to test three hypotheses. First, we
hypothesized that the use of a passive-elastic exoskeleton that resists
knee extension during the late leg swing phase would reduce metabolic
power during level-ground walking compared to walking without an
exoskeleton. Second, we hypothesized that the use of a passive-elastic
exoskeleton that stores energy from knee extension during the late leg
swing phase and returns energy for ankle powered plantarflexion during
late stance would reduce metabolic power during level-ground walking
compared to walking without an exoskeleton. Third, we hypothesized that
the use of a passive-elastic exoskeleton would not change stride length,
ground contact time, peak ground reaction forces, and step width during
level ground walking compared to walking without an exoskeleton.
Material and methods
Participants
Eight
healthy subjects [4 M and 4 F, mean ± SD age: 25 ± 3 years, mass:
73 ± 15 kg, height: 174 ± 10 cm, standing leg length: 83 ± 5 cm]
participated in the study. We measured their leg lengths from the
greater trochanter to the medial malleolus and averaged the right and
left leg lengths. All subjects gave informed written consent before
participating according to the University of Colorado Boulder
Institutional Review Board.
We measured metabolic rates, ground
reaction forces, and center of pressure while subjects walked on a
dual-belt force measuring treadmill with the exoskeleton springs
disengaged (no springs), engaged in parallel with the knee only, engaged
in parallel with the knee and ankle, engaged in parallel with the knee
only but with a longer engagement rope length, and engaged in parallel
with the knee and ankle but with a longer engagement rope length, and
without the exoskeleton.
Description of the exoskeleton
We
custom-made the passive-elastic exoskeleton, which consists of a
lightweight aluminum frame secured to the lower leg with a modified knee
brace (Ottobock HealthCare LP, Austin, US). The exoskeleton is equipped
with a mechanical apparatus comprised of six parts (Fig. 2,
panel e). The primary frame has a central pin that is fixed on the
external side of a modified knee brace, and all the other parts are
attached to this frame. An asymmetric pin holder includes two small pins
and rotates around the central pin, and an upper frame is fixed to the
primary frame and holds the system of springs and a pawl. A block, with
three arms and a ratchet wheel rotates about the central pin and
compresses the system of springs on the upper frame. A case, which
contains a spiral spring is attached distally on the longest arm of the
block. In addition, the exoskeleton includes two inextensible ropes (r1,
r2) that are fixed proximally on the anterior and posterior side of a
belt worn by the subject positioned just above the iliac spines and
glutei (Fig. 2),
and distally to the exoskeletal mechanical apparatus on the pawl (r1)
and the asymmetric pin holder (r2). Specifically, r2 is comprised of two
parts (Fig. 2b).
The superior part consists of a 4 cm wide piece of nylon webbing that
lies posteriorly over the middle of the gluteus, whereas the lower part
is a nylon rope that is attached to the mechanical apparatus. 4 cm wide
pieces of nylon webbing were used to increase the surface area on the
skin and prevent potential discomfort related to the pressure exerted by
the rope on the skin. A third inextensible rope (r3) that originates
from the exoskeletal case, is attached to the ankle frame surrounding
the subject’s heel (Fig. 2a). The total mass of the exoskeleton is ~ 1.4 kg per leg.
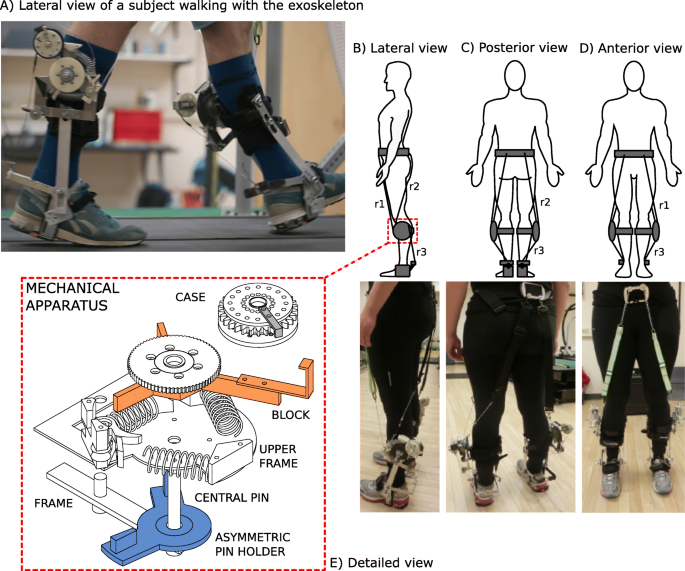
Fig. 2
a
Lateral view of a subject walking on the treadmill while using the
exoskeleton just as the rope (r3) provides plantarflexion assistance to
the trailing leg at the end of the stance phase. b Lateral, c Posterior, and d
Anterior views of the exoskeleton attached to the body and
corresponding pictures of a subject wearing the exoskeleton with ropes
attached from the anterior belt to the apparatus (r1), posterior belt to
the apparatus (r2) and apparatus to the ankle frame (r3). E) An
exploded view of the mechanical apparatus. We designed the upper frame
so that it could engage up to three linear springs. We used two springs
during the experimental sessions in order to attain an angular spring
stiffness of 17.45 Nm/rad. The mechanical apparatus is comprised of a
frame that anchors the upper frame to the braces on the shank. That
frame provides a central pin for the rotation of the asymmetric pin
holder and block. The case rotates around a pin (not shown), fixed on
the longer arm of the block
We
3D printed plastic ratchets and a pawl that were attached to the
lateral portion of the brace and allowed energy from the movement of the
knee to be stored through compression of the metal springs. The
exoskeleton is attached to each leg, but we describe the effects of the
exoskeleton for the right leg (Fig. 3).
At the end of the swing phase, after hip extension is maximal, r2 is
tensioned and rotates the asymmetric pin holder counter-clockwise (Fig. 3a), which pushes the block against the system of springs and compresses them (Fig. 3b).
At the same time, the 3D-printed pawl engages the ratchet wheel to keep
the spring compressed and prevent the clockwise rotation of the block
(Fig. 3b,
c, d). As r2 slackens, the asymmetric pin holder returns to its
original position and the knee can freely flex from the loading response
through mid-stance without any interaction with the engaged mechanical
apparatus. Prior to the beginning of the experimental trial, we set the
length of r2 to ensure it only tensioned in late swing, at maximum hip
flexion. As the shank moves forward, due to its inertia, the tension in
rope r2 provides a force that compresses the springs and allows the
exoskeleton to decelerate the shank prior to heel strike. Also, the
biological ankle’s motion is not affected by the exoskeleton due to a
spiral spring inside the case. This spring allows the case to rotate
from mid-swing through mid-stance (Fig. 3a,
b, c, d), while r3 remains slack and does not interfere with the motion
of the ankle. r3 only undergoes tension during late stance, when the
hip extends, and the case rotation is locked. During this phase, just
prior to powered plantarflexion, r1 is extended along the anterior side
of the upper leg, disengages the pawl, and releases the compressed
springs (Fig. 3e).
The pawl disengagement allows the system of springs to release the
stored energy; the block rotates clockwise lifting the case attached to
its longer arm, which pulls up on r3 and assists the ankle joint during
the push–off phase (Fig. 3f).
The posterior case, attached to the longer arm of the block, rotates
freely during a stride except for at the end of the stance phase, when
the central ratchet is released. Ankle joint plantarflexion is therefore
assisted by the elastic energy return of the exoskeleton. The
exoskeleton does not constrain the biological range of motion of the
ankle joint, and it is positioned at the same height and just lateral to
the ankle, which connects the brace and heel frame of the exoskeleton.
The ankle frame does not include a bearing but is designed to have low
friction and the lever arm of the ankle frame is approximately 0.125 m.
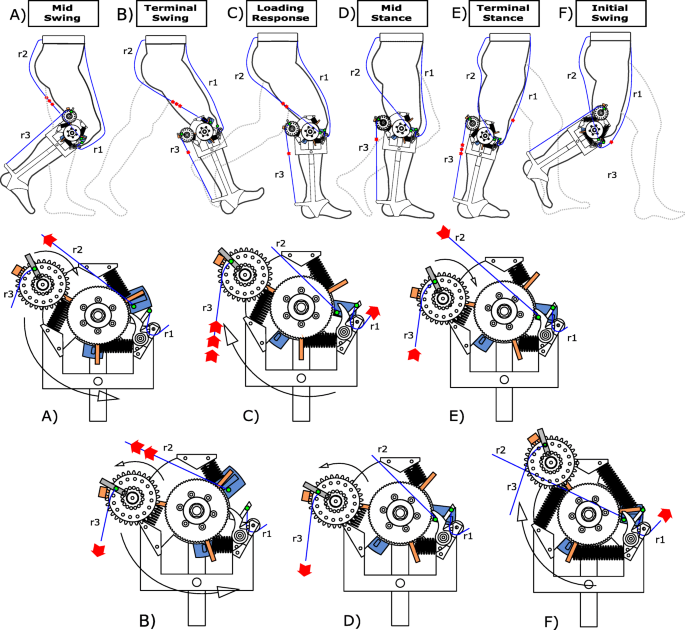
Fig. 3
Engagement
and disengagement of the exoskeleton mechanical apparatus during
different phases of a walking stride. The upper portion of the figure
shows the action of the exoskeleton during a stride and the lower
portion provides a detailed view of the knee mechanism. Red arrows
indicate the direction that ropes r1, r2 and r3 are moving during a
specific phase (in panel E, red arrows are also used to indicate the
extension of the linear springs). a During Mid-Swing, r2 begins
to stretch due to knee extension and pulls the central pin. This knee
extension movement continues until (b) Terminal Swing, and
results in the rotation of the block which, in turn, compresses the
springs. r3 also undergoes tension and causes the counterclockwise
rotation of the case during Terminal Swing (considering the lateral side
of the right leg). c During the Loading Response, both r2 and r3
become slack as the hip extends, which causes clockwise rotation of the
central pin and case, respectively. d During Mid-Stance, r3 is
stretched again as the hip rotates over the ankle and the case is locked
so that there is no additional counterclockwise rotation. e
During Terminal Stance, r1 is stretched due to hip extension, which
pulls the pawl out of the ratchet, and allows the linear springs to
extend and release their stored elastic energy. In this way, the block
rotates clockwise and pulls on r3, which provides assistance during
ankle powered plantarflexion. f At the subsequent Initial Swing only r1 is still stretched, while all of the other components of the device are disengaged
No comments:
Post a Comment