It can't be state of the art, nothing is mentioned on how they are dealing with spasticity. Unless they deal with it by cherry picking patients that don't have spasticity.
State of the art in parallel ankle rehabilitation robot: a systematic review
Journal of NeuroEngineering and Rehabilitation volume 18, Article number: 52 (2021)
Abstract
Background
The ankle joint complex (AJC) is of fundamental importance for balance, support, and propulsion. However, it is particularly susceptible to musculoskeletal and neurological injuries, especially neurological injuries such as drop foot following stroke. An important factor in ankle dysfunction is damage to the central nervous system (CNS). Correspondingly, the fundamental goal of rehabilitation training is to stimulate the reorganization and compensation of the CNS, and to promote the recovery of the motor system’s motor perception function. Therefore, an increasing number of ankle rehabilitation robots have been developed to provide long-term accurate and uniform rehabilitation training of the AJC, among which the parallel ankle rehabilitation robot (PARR) is the most studied. The aim of this study is to provide a systematic review of the state of the art in PARR technology, with consideration of the mechanism configurations, actuator types with different trajectory tracking control techniques, and rehabilitation training methods, thus facilitating the development of new and improved PARRs as a next step towards obtaining clinical proof of their rehabilitation benefits.
Methods
A literature search was conducted on PubMed, Scopus, IEEE Xplore, and Web of Science for articles related to the design and improvement of PARRs for ankle rehabilitation from each site’s respective inception from January 1999 to September 2020 using the keywords “ parallel”, “ ankle”, and “ robot”. Appropriate syntax using Boolean operators and wildcard symbols was utilized for each database to include a wider range of articles that may have used alternate spellings or synonyms, and the references listed in relevant publications were further screened according to the inclusion criteria and exclusion criteria.
Results and discussion
Ultimately, 65 articles representing 16 unique PARRs were selected for review, all of which have developed the prototypes with experiments designed to verify their usability and feasibility. From the comparison among these PARRs, we found that there are three main considerations for the mechanical design and mechanism optimization of PARRs, the choice of two actuator types including pneumatic and electrically driven control, the covering of the AJC’s motion space, and the optimization of the kinematic design, actuation design and structural design. The trajectory tracking accuracy and interactive control performance also need to be guaranteed to improve the effect of rehabilitation training and stimulate a patient’s active participation. In addition, the parameters of the reviewed 16 PARRs are summarized in detail with their differences compared by using figures and tables in the order they appeared, showing their differences in the two main actuator types, four exercise modes, fifteen control strategies, etc., which revealed the future research trends related to the improvement of the PARRs.
Conclusion
The selected studies showed the rapid development of PARRs in terms of their mechanical designs, control strategies, and rehabilitation training methods over the last two decades. However, the existing PARRs all have their own pros and cons, and few of the developed devices have been subjected to clinical trials. Designing a PARR with three degrees of freedom (DOFs) and whereby the mechanism’s rotation center coincides with the AJC rotation center is of vital importance in the mechanism design and optimization of PARRs. In addition, the design of actuators combining the advantages of the pneumatic-driven and electrically driven ones, as well as some new other actuators, will be a research hotspot for the development of PARRs. For the control strategy, compliance control with variable parameters should be further studied, with sEMG signal included to improve the real-time performance. Multimode rehabilitation training methods with multimodal motion intention recognition, real-time online detection and evaluation system should also be further developed to meet the needs of different ankle disability and rehabilitation stages. In addition, the clinical trials are in urgent need to help the PARRs be implementable as an intervention in clinical practice.
Background
The ankle joint complex (AJC) mainly consists of the tibia, fibula, talus and calcaneus, as shown in Fig. 1 [1]. The tibia and fibula are considered one unit to simplify the motions of the AJC, and the ankle joint involves the articulation between the tibia-fibula unit and the talus [1]. The AJC is of fundamental importance for balance, support, and propulsion. However, it is particularly susceptible to musculoskeletal and neurological injuries, especially neurological injuries such as the drop foot following stroke. Based on a report from the American Heart Association, approximately 795,000 people experience stroke in the United States each year [2]; stroke has poor prognosis and is associated with a high proportion of patients with drop foot, becoming the leading cause of permanent disabilities worldwide, with over 15 million new cases each year and 50 million stroke survivors [3]. An important factor in ankle dysfunction is damage to the central nervous system (CNS), which needs to be stimulated for reorganization and compensation and to promote the recovery of the motor system’s motor perception function [4]. Therefore, physiotherapy becomes essential for patients under this circumstance [5, 6]. During treatment, patients can regain their limited range of motion (ROM), restrengthen weak muscles, recover dynamic balance, and thus gradually restore motion functions [7]. However, this necessitates a long, repetitive, and intensive rehabilitation process, leading to a large burden and workload on the traditional ankle rehabilitation training, which is performed by therapists on a one-on-one hands-on basis to gradually stimulate and repair the damaged CNS [8]. In addition, traditional ankle rehabilitation training cannot provide sufficient training frequency and intensity due to limited time and resources [6]. Moreover, the rehabilitation training plans are developed based on therapists’ subjective clinical experience, which leads to the problem where therapists cannot accurately control the changes in complex forces, rehabilitation training forms and training parameters; hence, it is difficult to ensure accurate training of the affected limbs.
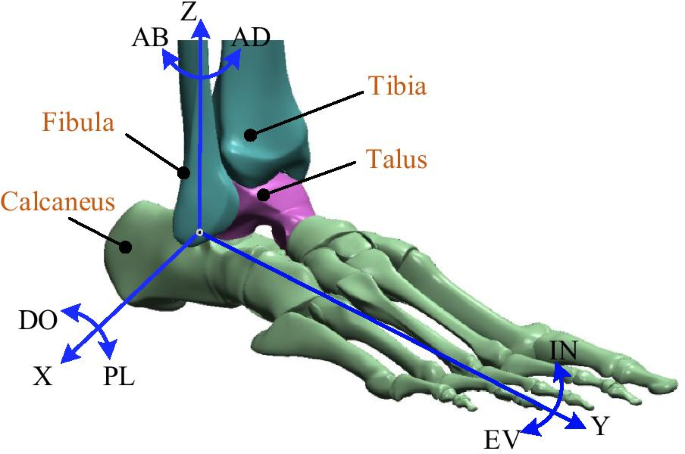
Anatomy of AJC and its rotational motions [1]
Therefore, it is of vital importance to replace traditional ankle rehabilitation training by developing ankle rehabilitation robots, which have the benefits of providing long-term accurate and uniform rehabilitation training as well as the ability to adaptively modify the difficulty of rehabilitation training according to real-time feedback from training [9]. In addition, the application of robot-assisted ankle rehabilitation techniques allows real-time data collection throughout the training process to further determine the accuracy of the training [10], therein allowing an assessment of the biomechanical properties of the AJC [11] and mobility [12] to customize future treatments [13]. Particularly, these techniques can effectively reduce the labor intensity of medical staff, improve the effect of ankle rehabilitation training and compensate for the shortage of rehabilitation medical resources. The parallel ankle rehabilitation robots (PARRs) and wearable devices are the most studied technologies for ankle rehabilitation, in which, the PARRs have a fixed platform and can be used for multiple degree of freedom (DOF) rehabilitation with a small size and high rigidity, while wearable devices are known as exoskeleton or powered orthoses and are often used for gait training. The advantage of a PARR compared with a wearable device is that the lower leg will not follow the swing during the process of ankle rehabilitation training, which can allow avoiding a secondary injury to the ankle joint.
Various reviews of robotic devices for ankle rehabilitation have been performed [6, 14,15,16,17]. However, references [6, 15,16,17] mainly focused on the mechanical design of ankle rehabilitation robots and covered both PARRs and wearable robots, while reference [14] focused on the effectiveness of robot-assisted therapy on ankle rehabilitation with both PARRs and wearable ones, and they concluded that wearable robots are more suitable for gait training, while PARRs are better suited for ankle exercises. Therefore, there is no systematic and comprehensive review specifically on the development of PARRs. With increasing research on PARRs, different mechanism configurations, actuator types, and rehabilitation training methods have been proposed, which may present a challenge to researchers new to this field.
The purpose of this paper is to provide a systematic review of the state of the art in PARR technology, with consideration of the mechanism configurations, actuator types, and rehabilitation training methods, thus serving as a tutorial for engineers who will design or control PARRs, making them aware of the advantages and limitations of different mechanical and control choices. From a research point of view, this paper also proposes a taxonomy expansion and a review of future research directions. The following sections review the PARRs with regard to the mechanism configurations, actuator types with different trajectory tracking control techniques, and rehabilitation training methods; we also compare, analyze and summarize them separately. Finally, the research hotspots and trends are discussed, and we present the takeaways regarding PARRs as the findings of this review.
No comments:
Post a Comment