Reducing
the metabolic cost of walking through use of assistive devices such as
exoskeletons would allow humans to walk further with less effort and
fatigue and could allow those with physical disabilities to be able to
walk. The idea of creating mechanical devices to assist human movement
and reduce metabolic cost has been around since the year 1890 [
1].
During the twentieth century, many scientists have focused their
efforts on creating mechanical devices that reduce the metabolic cost of
human movement [
2],
and during the last decade, use of an unpowered passive-elastic
exoskeleton has reduced the metabolic cost of walking compared to
walking without an exoskeleton by improving efficiency (quotient of
mechanical and metabolic power) [
3,
4].
Distinct
biomechanical tasks needed to walk, such as supporting body weight and
redirecting/accelerating the center of mass, require leg muscle force
and work, and thus incur a metabolic cost. The single limb support phase
of walking has been modelled as an inverted pendulum [
5,
6,
7]. In this model, the body’s mass is represented by a point mass and the stance leg by a rigid massless strut [
6,
7].
During the single support phase, mechanical energy is conserved through
the phasic exchange of kinetic and gravitational energy. However, the
muscles of the leg must produce force to support body weight during
single support and thus require metabolic energy [
8].
The muscles of the leg must also generate mechanical work to transition
body mass from step to step during the double support phase and this
incurs a greater metabolic cost than body weight support [
8,
9,
10].
Redirecting the center of mass during the step-to-step transition
requires approximately 45% of the overall net metabolic power; whereas
supporting body weight requires approximately 28% of the overall net
metabolic power needed for steady-speed level-ground walking [
8].
To facilitate walking, the muscles surrounding the ankle, knee, and hip
joints dissipate and generate mechanical work; these changes in
negative and positive energy could be exploited by a passive-elastic
exoskeleton to reduce metabolic cost.
The muscles surrounding the
ankle joint are primarily responsible for absorbing/producing power to
facilitate the redirection of the center of mass during the step-to-step
transition [
11].
Over a stride, the muscles surrounding the knee joint dissipate or
absorb/store net negative mechanical power and work, whereas the muscles
surrounding the ankle and hip joints generate net positive mechanical
power and work [
12].
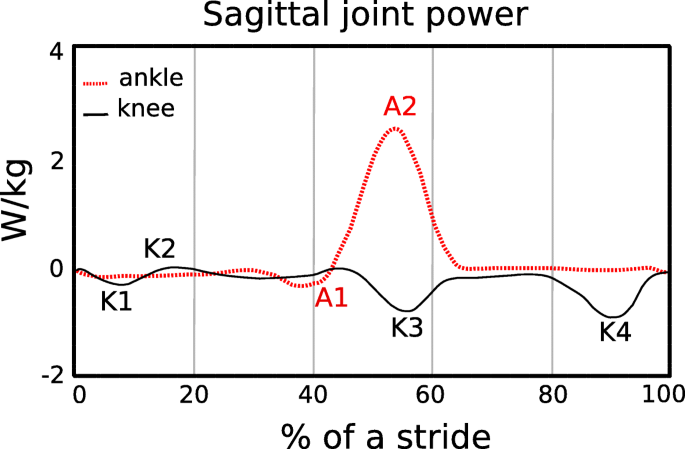
Negative and positive peaks in joint power indicate when mechanical
energy is absorbed and generated, respectively, during a stride (Fig.
1).
Negative peak power indicates eccentric contraction of the ankle
plantar-flexor muscles from heel-strike through tibial progression, knee
extensor muscles during heel-strike, rectus femoris during late stance,
and biceps femoris during late stance (Fig.
1).
Positive power regions primarily correspond to concentric contraction
of the ankle plantar-flexor muscles during late stance, knee extensor
muscles during early stance and hip flexor muscles during early swing
phase. All these muscle contractions incur a metabolic cost. Thus, an
exoskeleton that stores energy corresponding with the eccentric
contraction of the knee extensor muscles and returns this energy during
the concentric contraction of the ankle plantar-flexor muscles could
decrease the metabolic cost of walking.
In
order to reduce the metabolic cost of walking, use of an exoskeleton
should not alter kinematic gait parameters such as stride length and
step width, or kinetic parameters such as ground reaction forces.
Previous studies have shown that when people walk with stride lengths
and stride frequencies different from preferred, the metabolic cost of
walking increases [
14,
15,
16].
Walking speed is the product of stride length and stride frequency. At a
fixed walking speed, the relationship between stride frequency and
metabolic cost is represented by a U–shaped curve with the minimum
metabolic cost corresponding to the preferred stride frequency [
17].
Similarly, previous studies show that when humans walk with wider or
narrower step widths compared to preferred, their metabolic cost
increases [
18,
19,
20]. Step width indicates the lateral distance between the midlines of the feet [
21]. At a fixed walking speed, metabolic cost increases with the square of step width [
19].
Thus, use of an exoskeleton that results in changes to stride length,
stride frequency and step width compared to preferred could increase the
metabolic cost of walking.
The development of wearable devices
such as exoskeletons has been motivated by the challenge to reduce the
metabolic cost of walking. In 1890, Nicholas Yagn conceptualized and
received a patent for the first exoskeleton for assisting walking,
running, and jumping using pneumatically powered gas bags [
1].
Since then, many investigators have developed electrically powered or
battery-powered lower limb exoskeletons for medical applications,
neurorehabilitation therapy, augmentation, and military use [
2,
22,
23,
24,
25].
Most of the recent powered exoskeletons use actuators to provide
assistance at the ankle joint during powered plantarflexion at the end
of the stance phase of walking [
25,
26,
27,
28,
29,
30].
Specifically, use of powered exoskeletons has reduced the muscle
activity and lower limb joint work needed by the user during
level-ground walking compared to wearing the exoskeleton with the power
turned off. Together with the timing of the assistance, the weight of
these devices (12 kg to 38 kg [
22])
may be one of the reasons why use of a powered exoskeleton does not
decrease metabolic cost compared to normal walking without any wearable
system [
24].
With
new methodological innovations, current research shows that
exoskeletons can improve the metabolic cost of walking. Malcolm et al. [
30]
used optimal actuation timing predicted by a mathematical model
combined with a tethered electrically-powered exoskeleton that assists
ankle plantarflexion, and found that use of the exoskeleton reduced the
metabolic cost of walking at 1.38 m/s by 6.0 ± 2.0% (mean ± SD) compared
to walking without the exoskeleton. Mooney et al. [
25]
developed a battery-powered exoskeleton that utilizes a mathematical
model to control the magnitude of positive mechanical power provided by
the exoskeleton during ankle powered plantarflexion, and reduced
metabolic cost by 8 ± 3% compared to walking without an exoskeleton at
1.5 m/s. Thus, through the optimal timing and magnitude of applied
power, use of a powered exoskeleton can reduce the metabolic cost of
walking.
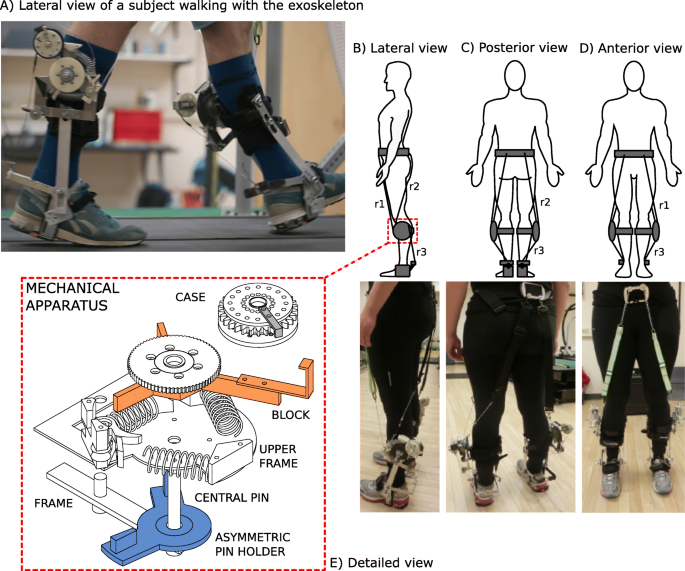
The way that an exoskeleton is attached to a person can
affect the assistance provided to the person and thus the metabolic cost
of walking. Panizzolo et al. [
31]
have investigated the use of an exosuit equipped with compliant
textiles that provide assistance instead of rigid structures, such as
those used in other powered exoskeletons. This approach aimed to improve
the interface between the exoskeleton and the body [
32] and reduce the mass on distal body segments to have less of an effect on metabolic cost [
33,
34].
In particular, the exosuit was designed to provide assistance during
both ankle joint plantarflexion at the end of the stance phase and hip
joint flexion during the early swing phase. Using this exosuit, net
metabolic power in the powered condition was 14.2 ± 6.1% lower than in
the unpowered condition, but net metabolic power was not reduced with
respect to normal walking at 1.5 m/s.
Use of passive-elastic
exoskeletons has reduced the metabolic cost of walking by enhancing the
mechanism of elastic energy storage and return at the ankle joint, with
springs in parallel to the Achilles tendon [
3,
25].
Recent studies demonstrate that storing and returning elastic energy
during the phases of ankle joint negative and positive mechanical power
can significantly reduce metabolic cost [
3,
35]. Collins et al. [
3]
has shown that use of a passive-elastic exoskeleton in parallel with
the ankle joint that stores and returns energy during the negative and
positive phases of ankle joint power (Fig.
1)
reduced metabolic cost by 7.2 ± 2.6% (mean ± SD) compared to walking
without an exoskeleton at 1.25 m/s. Many others have investigated how
use of a passive-elastic exoskeleton, which does not require an external
power supply and is not equipped with sensors or actuators, affects
walking [
3,
36,
37,
38,
39]. Panizzolo et al. [
3]
demonstrated that it is possible to reduce the metabolic cost of
walking by more than 3% with a passive device that assists the hip joint
compared to normal walking. Rome et al. [
38]
found that use of rubber bands in parallel with the hip joint can
reduce the metabolic costs of carrying loads during walking, whereas
Dean et al. [
39]
has shown that the use of a two-joint passive-elastic exoskeleton that
works in parallel with the hip and knee joints can reduce the activity
of lower limb muscles compared to normal walking [
39].
We
aimed to determine if a passive-elastic exoskeleton in parallel with
the knee and ankle joints could reduce the metabolic cost of walking. We
built an exoskeleton that stores energy from knee extension during the
late leg swing phase, which corresponds to negative peak knee power
(Fig.
1, K4) since it represents the greatest magnitude of energy absorption/storage during the stride [
12].
Then, we designed the exoskeleton to release the energy stored from
knee extension to assist ankle powered plantarflexion, which corresponds
to positive peak ankle power during late stance (Fig.
1,
A2). We designed our experiments to test three hypotheses. First, we
hypothesized that the use of a passive-elastic exoskeleton that resists
knee extension during the late leg swing phase would reduce metabolic
power during level-ground walking compared to walking without an
exoskeleton. Second, we hypothesized that the use of a passive-elastic
exoskeleton that stores energy from knee extension during the late leg
swing phase and returns energy for ankle powered plantarflexion during
late stance would reduce metabolic power during level-ground walking
compared to walking without an exoskeleton. Third, we hypothesized that
the use of a passive-elastic exoskeleton would not change stride length,
ground contact time, peak ground reaction forces, and step width during
level ground walking compared to walking without an exoskeleton.
 , Cheryl Forchuk , RN, PhD, Julie Walsh , BSc, Jennifer Fogarty , PhD & Michael Borrie , BSc, MB ChB, FRCPC
, Cheryl Forchuk , RN, PhD, Julie Walsh , BSc, Jennifer Fogarty , PhD & Michael Borrie , BSc, MB ChB, FRCPC