You'll want to make sure your loved never hears the DNR, the nocebo effect might occur and your loved one completes the “self-fulfilling prophecy” by dying. You'll have to ask what is the objective reason the patient is expected to die. See how badly your stroke doctors know nothing factual about stroke:
All guesswork like this:
Mercury astronaut Scott Carpenter suffers stroke; full recovery expected
Oops!
Scott Carpenter - Obituary
End-of-Life Care Decision-Making in Stroke
 Lucy Gao
Lucy Gao Charlie W. Zhao
Charlie W. Zhao David Y. Hwang
David Y. Hwang- 1Yale School of Medicine, New Haven, CT, United States
- 2Division of Neurocritical Care and Emergency Neurology, Yale School of Medicine, New Haven, CT, United States
Stroke is one of the leading causes of death and long-term disability in the United States. Though advances in interventions have improved patient survival after stroke, prognostication of long-term functional outcomes remains challenging, thereby complicating discussions of treatment goals. Stroke patients who require intensive care unit care often do not have the capacity themselves to participate in decision making processes, a fact that further complicates potential end-of-life care discussions after the immediate post-stroke period. Establishing clear, consistent communication with surrogates through shared decision-making represents best practice, as these surrogates face decisions regarding artificial nutrition, tracheostomy, code status changes, and withdrawal or withholding of life-sustaining therapies. Throughout decision-making, clinicians must be aware of a myriad of factors affecting both provider recommendations and surrogate concerns, such as cognitive biases. While decision aids have the potential to better frame these conversations within intensive care units, aids specific to goals-of-care decisions for stroke patients are currently lacking. This mini review highlights the difficulties in decision-making for critically ill ischemic stroke and intracerebral hemorrhage patients, beginning with limitations in current validated clinical scales and clinician subjectivity in prognostication. We outline processes for identifying patient preferences when possible and make recommendations for collaborating closely with surrogate decision-makers on end-of-life care decisions.
Introduction: Epidemiology of Life-Sustaining Therapy for Severe Stroke Patients
Stroke is a leading cause of death and long-term disability in the United States (US) (1, 2). The term “stroke” for this review focuses on two subtypes: acute ischemic stroke (AIS) and intracerebral hemorrhage (ICH). Clinicians are often confronted with issues related to end-of-life (EOL) care for stroke patients, such as code status, dysphagia care, and airway management (3). In order to tailor these decisions to patients' wishes, goals-of-care (GOC) discussions regarding acceptable quality of life (QoL) that require collaboration with surrogate decision-makers of incapacitated patients are needed.
Code status changes are among the earliest decisions that may occur during hospitalization for severe stroke. In practice, do-not-resuscitate (DNR) orders are often placed as early as within 24 hours of emergency department admission for both ICH (4) and AIS (5) patients. Approximately 13–26% of stroke patients receive DNR orders within 24 hours of admission (4, 5), with higher proportions of DNR status among those who later die of stroke (6, 7). There is concern that the act of making a patient DNR by itself affects clinicians' impressions of prognosis and independently increases the likelihood of mortality in AIS (5) and ICH (8, 9). This possible “self-fulfilling prophecy” is a well-established concern in stroke care (10).
In the days to weeks after admission, issues of nutrition and airway management often come to the forefront of decision-making. Percutaneous endoscopic gastrostomy (PEG) placement is currently performed throughout the US in 8.8% of patients with AIS (11) and 10.4% for ICH (12), with variation amongst institutions (11, 12). Over half of PEG placements for AIS occur in the first week of admission (13). For stroke patients who have difficulty maintaining an open airway or who require prolonged mechanical ventilation, tracheostomy in the US is commonly performed 6–14 days after stroke onset (14, 15), with increasing numbers over the past two decades (14). Rates of life-sustaining interventions are higher in minority patients than white patients (16), including PEG (17, 18) and tracheostomy (18).
In conjunction with these decisions, surrogates and clinical teams often decide to forgo life-sustaining measures and instead pursue comfort measures only (CMO). Withdrawal of life-sustaining therapy (WLST) is more common in neuro-intensive care units (Neuro-ICUs) than medical intensive care units (MICUs) (19), with up to 26% of all ICH patients in one single-center series undergoing WLST (20). Almost half of all stroke deaths occur inpatient (21), and hospitalized stroke patients have extensive palliative care needs (22, 23) that may not always be met. In one single-center US study from 2009-2015, about 4% of AIS patients were discharged to hospice (22).
In this brief review, we discuss the issues that arise when making EOL care decisions regarding stroke patients. We discuss prognostication tools, their limitations, methods to determine an incapacitated patient's wishes including advance care planning documentation (ACP) and best practices for shared decision-making with surrogates.
Prognostication: Limitations of Clinical Scales
One factor in EOL decision-making involves prognostication of long-term outcome or natural disease history. Multiple clinical scales have been developed to predict mortality and functional outcome after stroke (24–26), several of which have been externally validated (Table 1).
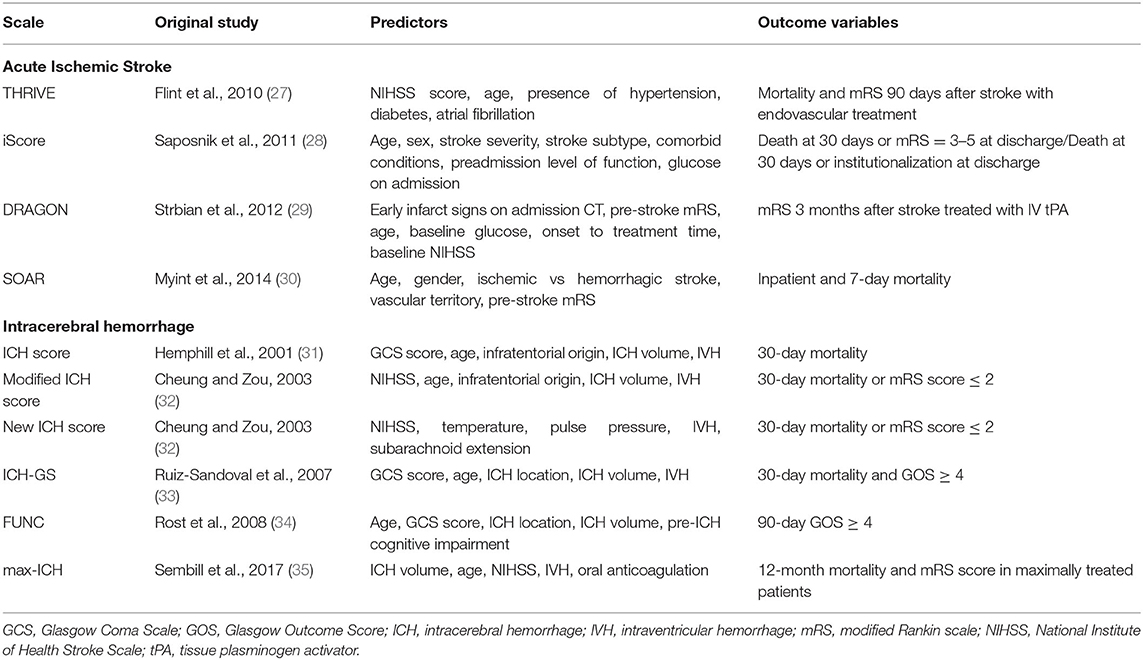
Table 1. Selected clinical scales developed for acute ischemic stroke and intracerebral hemorrhage.
Common predictor variables in AIS scales include age, stroke severity, pre-stroke functional status, comorbidities, and stroke subtype (24), with some scales utilizing imaging characteristics (36).
For ICH, many prognostication scales are based on variations of the “original” ICH score (33, 37–40), which was initially published with 30-day mortality data utilizing age, Glasgow Coma Scale at admission, ICH location, ICH volume, and presence of intraventricular hemorrhage (31).
Some published data suggest that scales largely outperform the “subjective” opinion of clinicians at predicting mortality and functional disability (41–43). However, these studies generally involved asking clinicians to prognosticate expected outcomes from hypothetical patient vignettes, which simplify and distill information that would otherwise be available in real-world clinical practice. In a comparison of the predictions of clinicians against common prognostication scales for 3-month functional status in real-world ICH patients, clinicians outperformed scales with regards to predictive accuracy (44).
This finding points towards the first of several limitations of prognostication scales—scales generate predictions using cohort data, yet prediction for individual patients may depend on variables not captured by scales. Furthermore, few models have been assessed for calibration (45) and robust external validation (25, 46), limiting their generalizability. Most scales were developed retrospectively, and data used to generate them include local practice patterns with regards to WLST, potentially incorporating the self-fulfilling prophesy. Finally, scales may not predict outcomes that are most important to patients and families, as the same functional outcome may lead to different perceptions of QoL for different patients. Clinicians have been shown to be poor at predicting a patient's future QoL, an inherently subjective quality, after stroke (47–49).
Despite these limitations, disclosing the results of a prognostication scale for a patient to a clinician impacts that clinician's clinical impression (50). Awareness of the limitations of scales can help ensure that the clinician utilizes these tools to complement clinical judgment rather than replace it. Recent studies suggest that making predictions based on clinical data from hospital day 5 rather than at admission may improve prognostication accuracy (51). Given the lack of objective tools for accurate prognostication and the potential for clinician bias to factor into decision-making, delaying prognostication may lead to improved prediction accuracy and clinical outcomes.
Goals-of-Care Conversations: Determining Patients' Wishes
Besides accurate neuro-prognostication, the ideal timing of GOC discussions regarding acceptable QoL for hospitalized stroke patients requires several considerations. GOC discussions, once initiated, are often iterative (1). Prognostic information should be tailored by amount and timing to the preferences of patients and families (52).
The aim of GOC discussions should be to ascertain the patient's wishes, or best estimates thereof, in order to provide goal-concordant care. As a means to this end, ACPs and surrogate decision-makers represent two sources of information for clinicians.
No comments:
Post a Comment