http://www.mdpi.com/2305-6320/4/4/72

1
School of Rehabilitation, Université de Montréal, Montréal, QC H3N 1X7, Canada
2
Centre for Interdisciplinary Research in Rehabilitation of Greater Montreal—IRGLM Site, Montreal, QC H3S 2J4, Canada
3
School of Rehabilitation, Université de Sherbrooke, Sherbrooke, QC J1H 5N4, Canada
4
Research
Center on Aging, Centre intégré universitaire de santé et des services
sociaux de l’Estrie-CHUS, Sherbrooke, QC J1H 4C4, Canada
*
Author to whom correspondence should be addressed.
Academic Editor: Gerhard Litscher
Received: 25 August 2017 / Revised: 25 September 2017 / Accepted: 27 September 2017 / Published: 30 September 2017
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
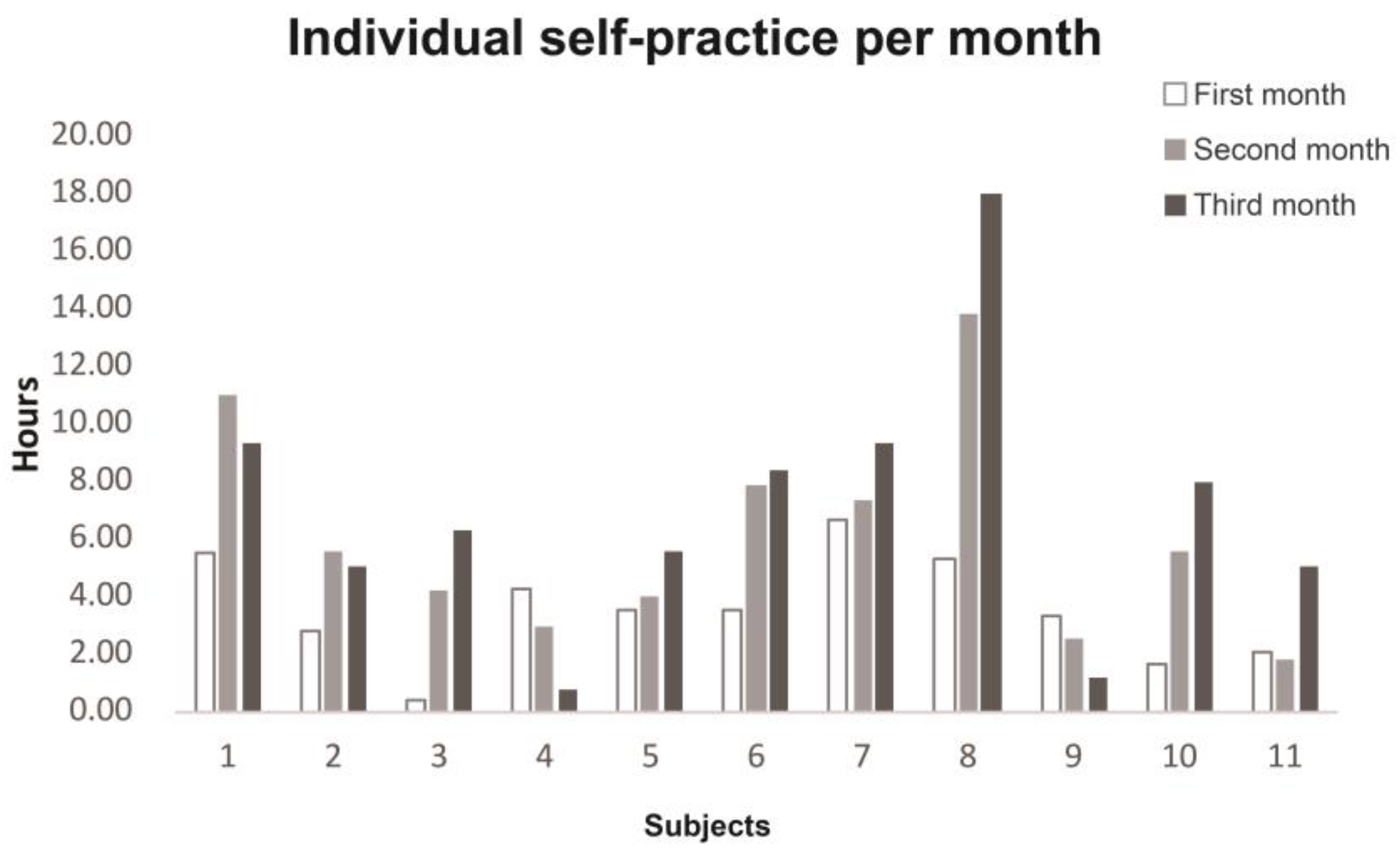
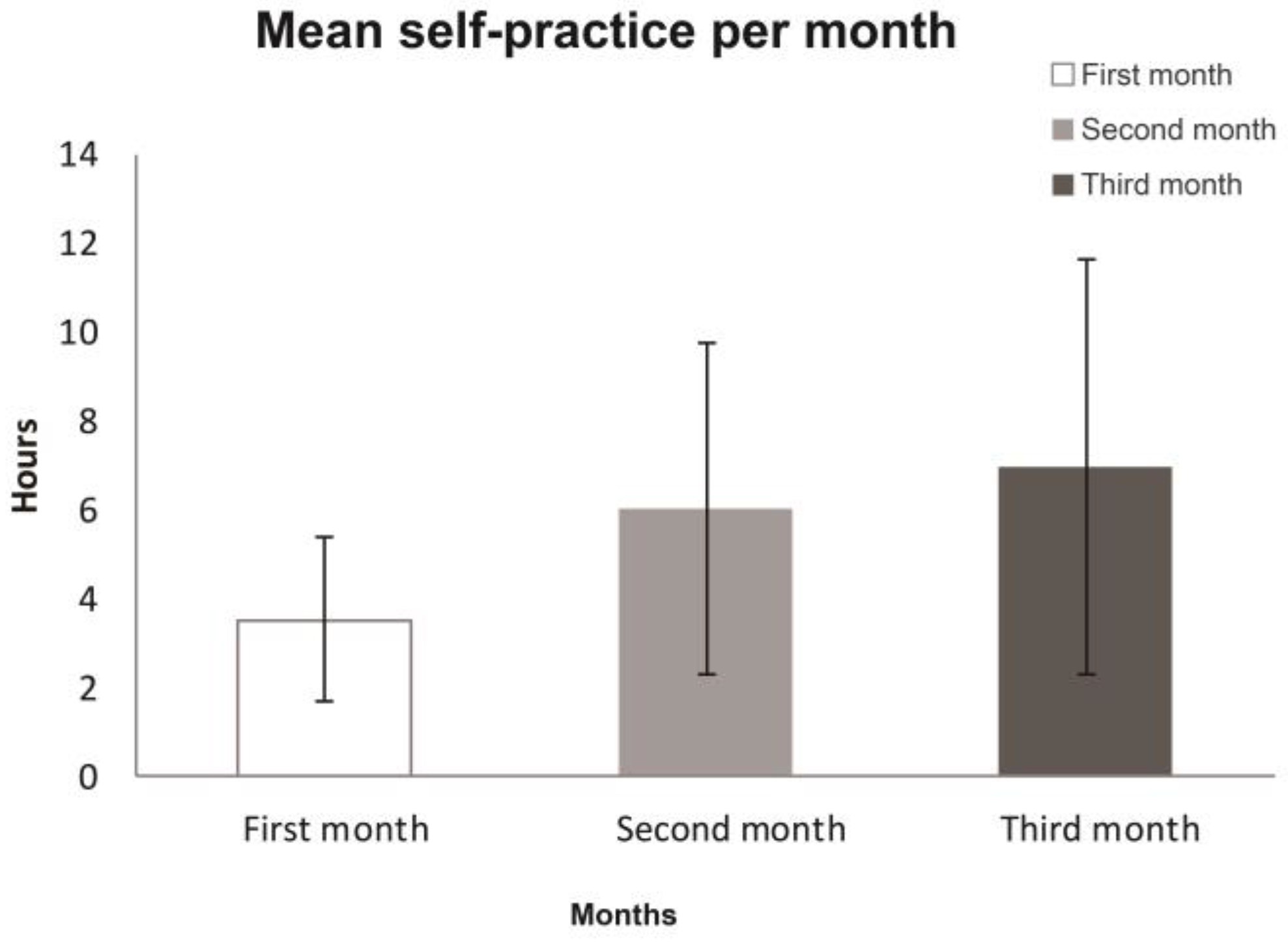
Background: Tai chi (TC) has been reported as being beneficial for improving balance post stroke, yet its utility in upper limb rehabilitation remains unknown.Methods: Twelve chronic stroke survivors with persistent paresis of an upper limb underwent 60 minutes of adapted TC twice a week for eight weeks, with a 4-week follow up. A 10-min TC home program was recommended for the days without sessions. TC level of performance, attendance to the sessions, duration of self-practice at home, and adapted TC movements used were recorded.
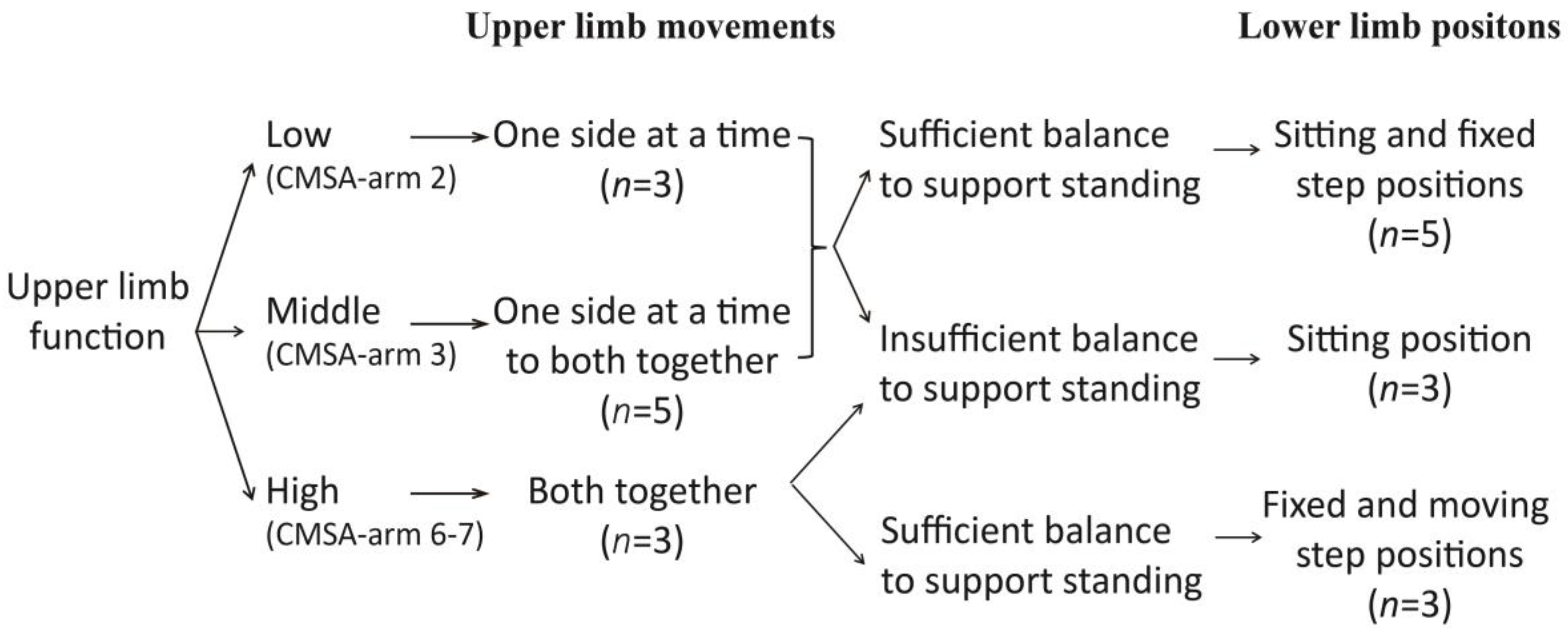
Results: Eleven participants completed the study. A clinical reasoning algorithm underlying the adaptation of TC was elaborated throughout the trial. Participants with varying profiles including a severely impaired upper limb, poor balance, shoulder pain, and severe spasticity were not only capable of practicing the adapted TC, but attended all 16 sessions and practiced TC at home for a total of 16.51 ± 9.21 h. The degree of self-practice for subgroups with low upper limb function, shoulder pain, or moderate-to-severe spasticity was similar to that of subgroups with greater upper limb function, no shoulder pain, and minimal-to-no spasticity.
Conclusion: Adapted TC seems feasible for upper limb rehabilitation post stroke. Although the study was based on a small sample size and requires confirmation, low upper limb function, insufficient balance, spasticity, and shoulder pain do not appear to hinder the practice of TC. View Full-Text
No comments:
Post a Comment