https://scientiaportal.wordpress.com/2016/11/09/amusia-and-stroke/
Although a complete musical anti-talent
myself, that doesn’t prohibit me from fully enjoying the works of the
masters in the art. When my family is out of earshot, I even bellow –
because it cannot be called music – from the top of my lungs alongside
the most famous tenors ever recorded. A couple of days ago I loaded one
of my most eclectic playlists. While remembering my younger days as an
Iron Maiden concert goer (I never said I listen only to classical music
:D) and screaming the “Fear of the Dark” chorus, I wondered what’s new
on the front of music processing in the brain.
And I found an interesting recent paper
about amusia. Amusia is, as those of you with ancient Greek proclivities
might have surmised, a deficit in the perception of music, mainly the
pitch but sometimes rhythm and other aspects of music. A small
percentage of the population is born with it, but a whooping 35 to 69%
of stroke survivors exhibit the disorder.
So Sihvonen et al. (2016)
decided to take a closer look at this phenomenon with the help of 77
stroke patients. These patients had an MRI scan within the first 3 weeks
following stroke and another one 6 months poststroke. They also
completed a behavioral test for amusia within the first 3 weeks
following stroke and again 3 months later. For reasons undisclosed, and
thus raising my eyebrows, the behavioral assessment was not performed at
6 months poststroke, nor an MRI at the 3 months follow-up. It would be
nice to have had behavioral assessment with brain images at the same
time because a lot can happen in weeks, let alone months after a stroke.
Nevertheless, the authors used a novel
way to look at the brain pictures, called voxel-based lesion-symptom
mapping (VLSM). Well, is not really novel, it’s been around for 15 years
or so. Basically, to ascertain the function of a brain region,
researchers either get people with a specific brain lesion and then look
for a behavioral deficit or get a symptom and then they look for a
brain lesion. Both approaches have distinct advantages but also
disadvantages (see Bates et al., 2003). To overcome the
disadvantages of these methods, enter the scene VLSM, which is a
mathematical/statistical gimmick that allows you to explore the
relationship between brain and function without forming preconceived
ideas, i.e. without forcing dichotomous categories. They also looked at
voxel-based morphometry (VBM), which a fancy way of saying they looked
to see if the grey and white matter differ over time in the brains of
their subjects.
After much analyses, Sihvonen et al.
(2016) conclude that the damage to the right hemisphere is more likely
conducive to amusia, as opposed to aphasia which is due mainly to damage
to the left hemisphere. More specifically,
“damage to the right temporal areas, insula, and putamen forms the crucial neural substrate for acquired amusia after stroke. Persistent amusia is associated with further [grey matter] atrophy in the right superior temporal gyrus (STG) and middle temporal gyrus (MTG), locating more anteriorly for rhythm amusia and more posteriorly for pitch amusia.”
The more we know, the better chances we have to improve treatments for people.
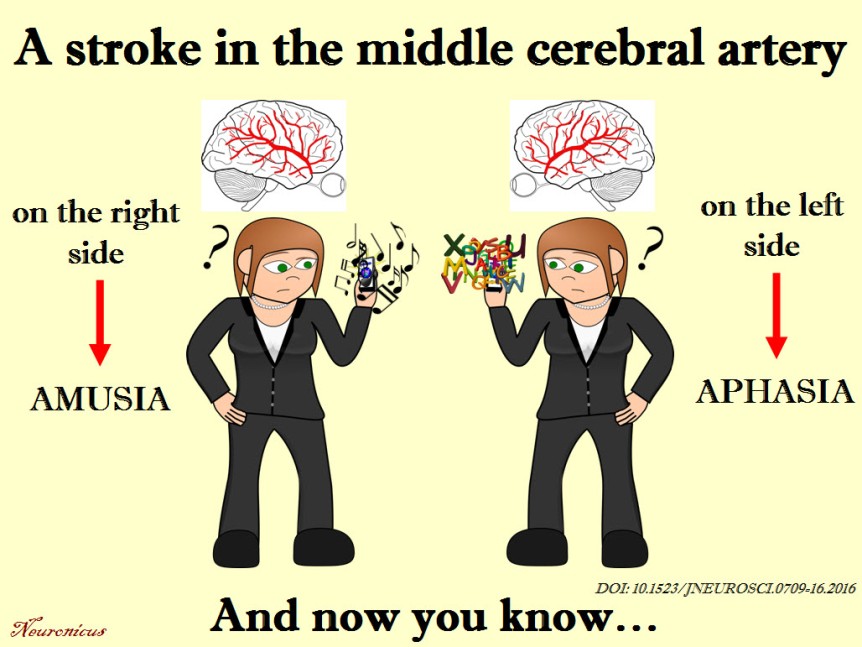
unless you’re left-handed, then things are reversed.
References:
1. Sihvonen AJ, Ripollés P, Leo V, Rodríguez-Fornells A, Soinila S, & Särkämö T. (24 Aug 2016). Neural Basis of Acquired Amusia and Its Recovery after Stroke. Journal of Neuroscience, 36(34):8872-8881. PMID: 27559169, DOI: 10.1523/JNEUROSCI.0709-16.2016. ARTICLE | FULLTEXT PDF2.Bates E, Wilson SM, Saygin AP, Dick F, Sereno MI, Knight RT, & Dronkers NF (May 2003). Voxel-based lesion-symptom mapping. Nature Neuroscience, 6(5):448-50. PMID: 12704393, DOI: 10.1038/nn1050. ARTICLE
By Neuronicus, 9 November 2016
No comments:
Post a Comment