Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 33,729 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke. DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
Is your doctor testing for this? To implement the protocols to prevent the next stroke and to cure the cerebral small vessel disease? Why not? Isn't your doctor supposed to be competent in all things stroke?
Cerebral
small vessel disease (cSVD) is a major cause of stroke and dementia.
This review summarizes recent developments in advanced neuroimaging of
cSVD with a focus on clinical and research applications.
In the
first section we highlight how advanced structural imaging techniques,
including diffusion MRI, enable improved detection of tissue damage,
including characterization of tissue appearing normal on conventional
MRI. These techniques enable progression to be monitored and may be
useful as surrogate endpoint in clinical trials. Quantitative MRI,
including iron and myelin imaging, provides insights into tissue
composition on the molecular level.
In the second section, we
cover how advanced MRI techniques can demonstrate functional or dynamic
abnormalities of the blood vessels, which could be targeted in
mechanistic research and early-stage intervention trials. Such
techniques include the use of dynamic contrast enhanced MRI to measure
blood-brain barrier permeability, and MRI methods to assess
cerebrovascular reactivity.
In the third section we discuss how
the increased spatial resolution provided by ultra-high field MRI at 7T
allows imaging of perforating arteries, and flow velocity and
pulsatility within them.
The advanced MRI techniques we describe
are providing novel pathophysiological insights in cSVD and allow
improved quantification of disease burden and progression. They have
application in clinical trials, both in assessing novel therapeutic
mechanisms, and as a sensitive endpoint to assess efficacy of
interventions on parenchymal tissue damage. We also discuss challenges
of these advanced techniques and suggest future directions for research.
So politely ask your doctor what are the EXACT DIET PROTOCOLS for all these conditions. S/he has had decades to come up with them, why don't they exist yet? The Mediterranean and DASH diets are not protocols(They are not specific enough to be of any use), therefore useless.
For stroke
prevention; for dementia prevention; for cognitive improvement; for
cholesterol reduction; for plaque removal; for Parkinsons prevention; for
inflammation reduction; for blood pressure reduction.
Two servings of avocado per week, compared with not eating any
avocado, was associated with lower risk for CVD and CHD, but not stroke,
researchers reported.
According to data published in the Journal of the American Heart Association, replacing half of one daily serving of margarine, butter, egg, yogurt, cheese or processed meats with avocado was tied to lower risk for CVD.
Data were derived from Pacheco LS, et al. J Am Heart Assoc. 2022;doi:10.1161/JAHA.121.024014.
“Avocados are a nutrient-rich food item with favorable
bioactive food compounds including monounsaturated and polyunsaturated
healthy fats, soluble fiber, vegetable proteins, phytosterols and
polyphenols and there are potential biological mechanisms by which
avocados offer cardioprotective benefits, which is through modulating CV
risk factors,” Lorena S. Pacheco, PhD, MPH, RDN, postdoctoral
research fellow in the nutrition department at the Harvard T.H. Chan
School of Public Health, told Healio. “The primary monounsaturated fatty
acid present in avocados is oleic acid, and it is suggested that it
helps in reducing hypertension, inflammation and insulin sensitivity.
Additionally, they contain plant sterols, that could have favorable
effects on lipid profiles. Moreover, the soluble fiber intake in
avocados can also lead to a better lipid profile.”
The researchers
reported that the Hass avocado, the most consumed variety in the U.S.,
contains approximately 13 g of oleic acid in a medium-sized fruit, which
is comparable to the amount of oleic acid in 1.5 oz of almonds or 2
tablespoons of olive oil. Additionally, half of an avocado contains
approximately 20% of the daily recommended fiber, 10% of daily
recommended potassium, 5% of daily recommended magnesium and 15% of
daily recommended folate.
“This study aimed to examine the
association between avocado consumption with CVD, which includes CHD and
stroke, in two large U.S. prospective cohort studies,” Pacheco told
Healio. “We also wanted to estimate the risk of CVD, CHD and stroke when
we substitute different fat-containing food sources with the same
amount of avocado.”
CV effects of weekly avocado intake
Researchers
included 68,786 women from NHS and 41,701 men from HPFS who had no
cancer, CHD or stroke at baseline. Avocado intake was evaluated using
validated food frequency questionnaires at baseline and then every 4
years. Median follow-up was approximately 13 years for women and 14
years for men.
Overall, participants with higher avocado
consumption also had higher total energy intake and diet quality,
including greater intake of fruits, vegetables, whole grains, nuts and
dairy products compared with those with lower avocado consumption.
For the present analysis, half of an avocado was classified as a single serving.
Researchers
reported that individuals who ate at least two servings of avocado per
week experienced 16% lower risk for CVD (HR = 0.84; 95% CI, 0.75-0.95; P for trend = .0007) and 21% lower risk for CHD (HR = 0.79; 95% CI, 0.68-0.91; P
for trend < .001) compared with those who did not consume avocado.
However, they observed no association between avocado intake and risk
for stroke (P for trend = .78).
“We defined CVD as the
composite of fatal CHD and nonfatal MI and fatal and nonfatal stroke,”
Pacheco told Healio. “Thus, we did find an association with CVD but not
with stroke, meaning that the risk of CVD is primarily driven by CHD. As
my co-authors and I discuss in the paper, our stroke findings could be
explained by chance or the lack of statistical power in our models.”
For
every half-serving increase in avocado intake per day, researchers
observed an approximately 20% lower risk for CVD (HR = 0.8; 95% CI,
0.71-0.91), according to the study.
Moreover, replacing half of
one daily serving of margarine, butter, egg, yogurt, cheese or processed
meats with a half serving of avocado was associated with a 16% to 22%
lower risk for CVD, according to the study.
“We know avocados
impart heart-healthy benefits. Yet, avocados are also calorie-rich, so
pairing them with chips or the like compromises those benefits since we
need to consider your portion of avocado and your portion of chips,”
Pacheco told Healio. “In most cases, when you have guacamole or similar
spreads, it is easy to overconsume them, increasing your overall
calories. Besides this, most of us do not pay attention to the serving
size on the bag of chips and keep ‘munching away’, making this a
troublesome combination.”
Benefits of a routine healthy diet
“We
desperately need strategies to improve intake of AHA-recommended
healthy diets — such as the Mediterranean diet — that are rich in
vegetables and fruits,” Cheryl Anderson, PhD, MPH, FAHA,
professor and dean of the Herbert Wertheim School of Public Health and
Human Longevity Science at University of California, San Diego, and
chair of the AHA Council on Epidemiology and Prevention, said in the
release. “Although no one food is the solution to routinely eating a
healthy diet, this study is evidence that avocados have possible health
benefits. This is promising because it is a food item that is popular,
accessible, desirable and easy to include in meals eaten by many
Americans at home and in restaurants.”
Nicotinamide
adenine dinucleotide (NAD) is an important cofactor in numerous
metabolic reactions. NAD concentrations decline with age, which may
contribute to age-associated conditions such as Parkinson’s disease.
Preclinical studies show that replenishing NAD by supplementation with
nicotinamide riboside (NR), a biosynthetic precursor to NAD, can promote
health span and neuroprotection. Brakedal et al. performed a
randomized, double-blind phase 1 clinical trial of NR supplementation in
30 patients newly diagnosed with Parkinson’s disease. They found that
NR supplementation was safe and that concentrations of NAD in the brain
increased in most patients receiving NR. These patients had signs of
altered cerebral metabolism and mild clinical improvement, although
further testing is needed with a larger cohort to confirm any clinical
benefit.
This
study aimed to examine whether robotic self-training improved
upper-extremity function versus conventional self-training in
mild-to-moderate hemiplegic chronic stroke patients.
METHODS:
Study
design was a multi-center, prospective, randomized, parallel-group
study comparing three therapist-guided interventions (1-hour sessions,
3×/wk, 10 weeks). We identified 161 prospective patients with chronic,
poststroke, upper-limb hemiplegia treated at participating
rehabilitation centers. Patients were enrolled between November 29,
2016, and November 12, 2018 in Japan. A blinded web-based allocation
system was used to randomly assign 129 qualifying patients into 3
groups: (1) conventional self-training plus conventional therapy
(control, N=42); (2) robotic self-training (ReoGo-J) plus conventional
therapy (robotic therapy [RT], N=44); or (3) robotic self-training plus
constraint-induced movement therapy (N=43). Primary outcome: Fugl-Meyer
Assessment for upper-extremity. Secondary outcomes: Motor Activity
Log-14 amount of use and quality of movement; Fugl-Meyer Assessment
shoulder/elbow/forearm, wrist, finger, and coordination scores; Action
Research Arm Test Score; Motricity Index; Modified Ashworth Scale;
shoulder, elbow, forearm, wrist, and finger range of motion; and Stroke
Impact Scale (the assessors were blinded). Safety outcomes were adverse
events.
RESULTS:
Safety
was assessed in 127 patients. An intention-to-treat full analysis set
(N=121), and a per-protocol set (N=115) of patients who attended 80% of
sessions were assessed. One severe adverse event was recorded, unrelated
to the robotic device. No significant differences in Fugl-Meyer
Assessment for upper-extremity scores were observed between groups (RT
versus control: −1.04 [95% CI, −2.79 to 0.71], P=0.40; RT versus movement therapy: −0.33 [95% CI, −2.02 to 1.36], P=0.90).
The RT in the per-protocol set improved significantly in the Fugl-Meyer
Assessment for upper-extremity shoulder/elbow/forearm score (RT versus
control: −1.46 [95% CI, −2.63 to −0.29]; P=0.037).
CONCLUSIONS:
Robotic
self-training did not improve upper-limb function versus usual
self-training, but may be effective combined with conventional therapy
in some populations (per-protocol set).
The THRIVE score and the THRIVE-c calculation are validated ischemic
stroke outcome prediction tools based on patient variables that are
readily available at initial presentation. Randomized controlled trials
(RCTs) have demonstrated the benefit of endovascular treatment (EVT) for
many patients with large vessel occlusion (LVO), and pooled data from
these trials allow for adaptation of the THRIVE-c calculation for use in
shared clinical decision making regarding EVT.
Methods:
To
extend THRIVE-c for use in the context of EVT, we extracted data from
the Virtual International Stroke Trials Archive (VISTA) from 7 RCTs of
EVT. Models were built in a randomly selected development cohort using
logistic regression that included the predictors from THRIVE-c: age, NIH
Stroke Scale (NIHSS) score, presence of hypertension, diabetes
mellitus, and/or atrial fibrillation, as well as randomization to EVT
and, where available, the Alberta Stroke Program Early CT Score
(ASPECTS).
Results: Good outcome(But not 100% recovery, so it wasn't a good outcome. Words matter, use the correct ones. 'We failed at 100% recovery') was achieved in 366/787
(46.5%) of subjects randomized to EVT and in 236/795 (29.7%) of subjects
randomized to control (P<0.001), and the improvement in outcome with
EVT was seen across age, NIHSS, and THRIVE-c good outcome prediction.
Models to predict outcome using THRIVE elements (age, NIHSS, and
comorbidities) together with EVT, with or without ASPECTS, had similar
performance by ROC analysis in the development and validation cohorts
(THRIVE-EVT ROC area under the curve [AUC] = 0.716 in development, 0.727
in validation, P=0.30; THRIVE-EVT+ASPECTS ROC AUC = 0.718 in
development, 0.718 in validation, P=0.12).
Conclusion:
THRIVE-EVT may be used alongside the original THRIVE-c calculation to
improve outcome probability estimation for patients with acute ischemic
stroke, including patients with or without LVO, and to model the
potential improvement in outcomes with EVT for an individual patient
based on variables that are available at initial presentation. Online
calculators for THRIVE-c estimation are available at www.thrivescore.org
and www.mdcalc.com/thrive-score-for-stroke-outcome.
Our stroke researchers should have been heavily involved in this for a decade.
With NO LEADERSHIP IN STROKE, it takes forever to make research usable. That is a disgusting timeline. Every stroke 'leader' should be fired.
If we had any leadership at all in stroke,
when these nanorobots were introduced we would have had drug delivery
and roto-rooter abilities already accomplished.
Tiny machines that deliver therapeutic payloads to
precise locations in the body are the stuff of science fiction. But some
researchers are trying to turn them into a clinical reality.
Cancer drugs usually take a scattergun approach.
Chemotherapies inevitably hit healthy bystander cells while blasting
tumours, sparking a slew of side effects. It is also a big ask for an
anticancer drug to find and destroy an entire tumour — some are
difficult to reach, or hard to penetrate once located.
A
long-dreamed-of alternative is to inject a battalion of tiny robots into
a person with cancer. These miniature machines could navigate directly
to a tumour and smartly deploy a therapeutic payload right where it is
needed. “It is very difficult for drugs to penetrate through biological
barriers, such as the blood–brain barrier or mucus of the gut, but a
microrobot can do that,” says Wei Gao, a medical engineer at the
California Institute of Technology in Pasadena.
Among his inspirations is the 1966 film Fantastic Voyage,
in which a miniaturized submarine goes on a mission to remove a blood
clot in a scientist’s brain, piloted through the bloodstream by a
similarly shrunken crew. Although most of the film remains firmly in the
realm of science fiction, progress on miniature medical machines in the
past ten years has seen experiments move into animals for the first
time.
There are now numerous micrometre- and nanometre-scale
robots that can propel themselves through biological media, such as the
matrix between cells and the contents of the gastrointestinal tract.
Some are moved and steered by outside forces, such as magnetic fields
and ultrasound. Others are driven by onboard chemical engines, and some
are even built on top of bacteria and human cells to take advantage of
those cells’ inbuilt ability to get around. Whatever the source of
propulsion, it is hoped that these tiny robots will be able to deliver
therapies to places that a drug alone might not be able to reach, such
as into the centre of solid tumours. However, even as those working on
medical nano- and microrobots begin to collaborate more closely with
clinicians, it is clear that the technology still has a long way to go
on its fantastic journey towards the clinic.
In the 1966 film Fantastic Voyage, a miniaturized medical team goes on a mission to remove a blood clot in a scientist’s brain.Contributor: Collection Christophel/Alamy Stock Photo
Poetry in motion
One of the key challenges for a robot operating inside the human body is getting around. In Fantastic Voyage,
the crew uses blood vessels to move through the body. However, it is
here that reality must immediately diverge from fiction. “I love the
movie,” says roboticist Bradley Nelson, gesturing to a copy of it in his
office at the Swiss Federal Institute of Technology (ETH) Zurich in
Switzerland. “But the physics are terrible.” Tiny robots would have
severe difficulty swimming against the flow of blood, he says. Instead,
they will initially be administered locally, then move towards their
targets over short distances.
When it comes to design, size
matters. “Propulsion through biological media becomes a lot easier as
you get smaller, as below a micron bots slip between the network of
macromolecules,” says Peer Fischer, a robotics researcher at the Max
Planck Institute for Intelligent Systems in Stuttgart, Germany. Bots are
therefore typically no more than 1–2 micrometres across. However, most
do not fall below 300 nanometres. Beyond that size, it becomes more
challenging to detect and track them in biological media, as well as
more difficult to generate sufficient force to move them.
Scientists
have several choices for how to get their bots moving. Some opt to
provide power externally. For instance, in 2009, Fischer — who was
working at Harvard University in Cambridge, Massachusetts, at the time,
alongside fellow nanoroboticist Ambarish Ghosh — devised a glass
propeller, just 1–2 micrometres in length, that could be rotated by a
magnetic field1.
This allowed the structure to move through water, and by adjusting the
magnetic field, it could be steered with micrometre precision. In a 2018
study2, Fischer launched a swarm of micropropellers into a pig’s eye in vitro,
and had them travel over centimetre distances through the gel-like
vitreous humour into the retina — a rare demonstration of propulsion
through real tissue. The swarm was able to slip through the network of
biopolymers within the vitreous humour thanks in part to a silicone oil
and fluorocarbon coating applied to each propeller. Inspired by the
slippery surface that the carnivorous pitcher plant Nepenthes uses to catch insects, this minimized interactions between the micropropellers and biopolymers.
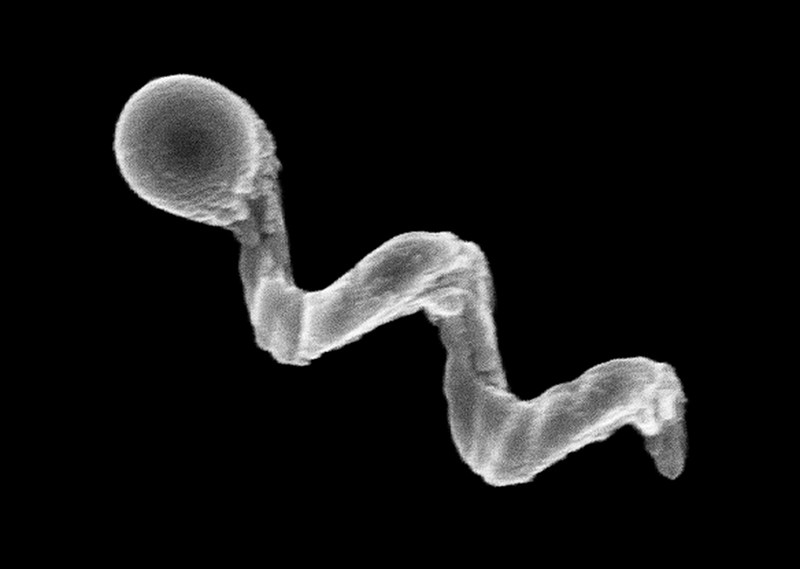
An electron microscope image of a glass nanopropeller.Credit: Conny Miksch, MPI-IS
Another way to provide propulsion from outside the body is
to use ultrasound. One group placed magnetic cores inside the membranes
of red blood cells3,
which also carried photoreactive compounds and oxygen. The cells’
distinctive biconcave shape and greater density than other blood
components allowed them to be propelled using ultrasonic energy, with an
external magnetic field acting on the metallic core to provide
steering. Once the bots are in position, light can excite the
photosensitive compound, which transfers energy to the oxygen and
generates reactive oxygen species to damage cancer cells.
This
hijacking of cells is proving to have therapeutic merits in other
research projects. Some of the most promising strategies aimed at
treating solid tumours involve human cells and other single-celled
organisms jazzed up with synthetic parts. In Germany, a group led by
Oliver Schmidt, a nanoscientist at Chemnitz University of Technology,
has designed a biohybrid robot based on sperm cells4.
These are some of the fastest motile cells, capable of hitting speeds
of 5 millimetres per minute, Schmidt says. The hope is that these
powerful swimmers can be harnessed to deliver drugs to tumours in the
female reproductive tract, guided by magnetic fields. Already, it has
been shown that they can be magnetically guided to a model tumour in a
dish.
Credit: Leibniz IFW, Dresden
“We could load anticancer drugs efficiently into the head of
the sperm, into the DNA,” says Schmidt. “Then the sperm can fuse with
other cells when it pushes against them.” At the Chinese University of
Hong Kong, meanwhile, nanoroboticist Li Zhang led the creation of
microswimmers from Spirulina microalgae cloaked in the mineral
magnetite. The team then tracked a swarm of them inside rodent stomachs
using magnetic resonance imaging5. The biohybrids were shown to selectively target cancer cells. They also gradually degrade, reducing unwanted toxicity.
Another
way to get micro- and nanobots moving is to fit them with a chemical
engine: a catalyst drives a chemical reaction, creating a gradient on
one side of the machine to generate propulsion. Samuel Sánchez, a
chemist at the Institute for Bioengineering of Catalonia in Barcelona,
Spain, is developing nanomotors driven by chemical reactions for use in
treating bladder cancer. Some early devices relied on hydrogen peroxide
as a fuel. Its breakdown, promoted by platinum, generated water and
oxygen gas bubbles for propulsion. But hydrogen peroxide is toxic to
cells even in minuscule amounts, so Sánchez has transitioned towards
safer materials. His latest nanomotors are made up of honeycombed silica
nanoparticles, tiny gold particles and the enzyme urease6.
These 300–400-nm bots are driven forwards by the chemical breakdown of
urea in the bladder into carbon dioxide and ammonia, and have been
tested in the bladders of mice. “We can now move them and see them
inside a living system,” says Sánchez.
Breaking through
A
standard treatment for bladder cancer is surgery, followed by
immunotherapy in the form of an infusion of a weakened strain of Mycobacterium bovis
bacteria into the bladder, to prevent recurrence. The bacterium
activates the person’s immune system, and is also the basis of the BCG
vaccine for tuberculosis. “The clinicians tell us that this is one of
the few things that has not changed over the past 60 years,” says
Sánchez. There is a need to improve on BCG in oncology, according to his
collaborator, urologic oncologist Antoni Vilaseca at the Hospital
Clinic of Barcelona. Current treatments reduce recurrences and
progression, “but we have not improved survival”, Vilaseca says. “Our
patients are still dying.”
The nanobot approach that Sánchez is
trying promises precision delivery. He plans to insert his bots into the
bladder (or intravenously), to motor towards the cancer with their
cargo of therapeutic agents to target cancer cells, using abundant urea
as a fuel. He might use a magnetic field for guidance, if needed, but a
more straightforward replacement of BCG with bots that do not require
external control, perhaps using an antibody to bind a tumour marker,
would please clinicians most. “If we can deliver our treatment to the
tumour cells only, then we can reduce side effects and increase
activity,” says Vilaseca.
An optical microscopy video showing a swarm of urease-powered nanomotors swimming in urea solution.Credit: Samuel Sánchez Ordóñez
Not all cancers can be reached by swimming through liquid,
however. Natural physiological barriers can block efficient drug
delivery. The gut wall, for example, allows absorption of nutrients into
the bloodstream, and offers an avenue for getting therapies into
bodies. “The gastrointestinal tract is the gateway to our body,” says
Joseph Wang, a nanoengineer at the University of California, San Diego.
However, a combination of cells, microbes and mucus stops many particles
from accessing the rest of the body. To deliver some therapies, simply
being in the intestine isn’t enough — they also need to be able to
burrow through its defences to reach the bloodstream, and a nanomachine
could help with this.
In 2015, Wang and his colleagues, including Gao, reported the first self-propelled robot invivo, inside a mouse stomach7.
Their zinc-based nanomotor dissolved in the harsh stomach acids,
producing hydrogen bubbles that rocketed the robot forwards. In the
lower gastrointestinal tract, they instead use magnesium. “Magnesium
reacts with water to give a hydrogen bubble,” says Wang. In either case,
the metal micromotors are encapsulated in a coating that dissolves at
the right location, freeing the micromotor to propel the bot into the
mucous wall.
Some bacteria have already worked out their own ways to sneak through the gut wall. Helicobacterpylori,
which causes inflammation in the stomach, excretes urease enzymes to
generate ammonia and liquefy the thick mucous that lines the stomach
wall. Fischer envisages future micro- and nanorobots borrowing this
approach to deliver drugs through the gut.
Solid tumours are another difficult place to deliver a drug.
As these malignancies develop, a ravenous hunger for oxygen promotes an
outside surface covered with blood vessels, while an oxygen-deprived
core builds up within. Low oxygen levels force cells deep inside to
switch to anaerobic metabolism and churn out lactic acid, creating
acidic conditions. As the oxygen gradient builds, the tumour becomes
increasingly difficult to penetrate. Nanoparticle drugs lack a force
with which to muscle through a tumour’s fortifications, and typically
less than 2% of them will make it inside8. Proponents of nanomachines think that they can do better.
Sylvain
Martel, a nanoroboticist at Montreal Polytechnic in Canada, is trying
to break into solid tumours using bacteria that naturally contain a
chain of magnetic iron-oxide nanocrystals. In nature, these Magnetococcus
species seek regions that have low oxygen. Martel has engineered such a
bacterium to target active cancer cells deep inside tumours8.
“We guide them with a magnetic field towards the tumour,” explains
Martel, taking advantage of the magnetic crystals that the bacteria
typically use like a compass for orientation. The precise locations of
low-oxygen regions are uncertain even with imaging, but once these
bacteria reach the right location, their autonomous capability kicks in
and they motor towards low-oxygen regions. In a mouse, more than half
the bacteria injected close to tumour grafts broke into this tumour
region, each laden with dozens of drug-loaded liposomes. Martel
cautions, however, that there is still some way to go before the
technology is proven safe and effective for treating people with cancer.
In
the Netherlands, chemist Daniela Wilson at Radboud University in
Nijmegen and colleagues have developed enzyme-driven nanomotors powered
by DNA that might similarly be able to autonomously home in on tumour
cells9.
The motors navigate towards areas that are richer in DNA, such as
tumour cells that undergoing apoptosis. “We want to create systems that
are able to sense gradients by different endogenous fuels in the body,”
Wilson says, suggesting that the higher levels of lactic acid or glucose
typically found in tumours could also be used for targeting. Once in
place, the autonomous bots seem to be picked up by cells more easily
than passive particles are — perhaps because the bots push against
cells.
Nanoroboticist Sylvain Martel (middle) discusses a new computer interface with two members of his team.Credit: Caroline Perron
Fiction versus reality
Inspirational though Fantastic Voyage
might have been for many working in the field of medical nanorobotics,
there are some who think the film has become a burden. “People think of
this as science fiction, which excites people, but on the other hand
they don’t take it so seriously,” says Martel. Fischer is similarly
jaded by movie-inspired hype. “People sometimes write very liberally as
if nanobots for cancer treatment are almost here,” he says. “But this is
not even in clinical trials right now.”
Nonetheless, advances in
the past ten years have raised expectations of what is possible with
current technology. “There’s nothing more fun than building a machine
and watching it move. It’s a blast,” says Nelson. But having something
wiggling under a microscope no longer has the same draw, without medical
context. “You start thinking, ‘how could this benefit society?’” he
says.
With this in mind, many researchers creating nanorobots for
medical purposes are working more closely with clinicians than ever
before. “You find a lot of young doctors who are really interested in
what the new technologies can do,” Nelson says. Neurologist Philipp
Gruber, who works with stroke patients at Aarau Cantonal Hospital in
Switzerland, began a collaboration with Nelson two years ago after
contacting ETH Zurich. The pair share an ambition to use steerable
microbots to dissolve clots in people’s brains after ischaemic stroke —
either mechanically, or by delivering a drug. “Brad knows everything
about engineering,” says Gruber, “but we can advise about the problems
we face in the clinic and the limitations of current treatment options.”
Sánchez
tells a similar story: while he began talking to physicians around a
decade ago, their interest has warmed considerably since his experiments
in animals began three to four years ago. “We are still in the lab, but
at least we are working with human cells and human organoids, which is a
step forward,” says his collaborator Vilaseca.
As these seedlings
of clinical collaborations take root, it is likely that oncology
applications will be the earliest movers — particularly those that
resemble current treatments, such as infusing microbots instead of BCG
into cancerous bladders. But even these therapeutic uses are probably at
least 7–10 years away. In the nearer term, there might be simpler tasks
that nanobots can be used to accomplish, according to those who follow
the field closely.
For example, Martin Pumera, a nanoroboticist at
the University of Chemistry and Technology in Prague, is interested in
improving dental care by landing nanobots beneath titanium tooth
implants10.
The tiny gap between the metal implants and gum tissue is an ideal
niche for bacterial biofilms to form, triggering infection and
inflammation. When this happens, the implant must often be removed, the
area cleaned, and a new implant installed — an expensive and painful
procedure. He is collaborating with dental surgeon Karel Klíma at
Charles University in Prague.
Another problem the two are tackling
is oral bacteria gaining access to tissue during surgery of the jaws
and face. “A biofilm can establish very quickly, and that can mean
removing titanium plates and screws after surgery, even before a
fracture heals,” says Klíma. A titanium oxide robot could be
administered to implants using a syringe, then activated chemically or
with light to generate active oxygen species to kill the bacteria.
Examples a few micrometres in length have so far been constructed, but
much smaller bots — only a few hundred nanometres in length — are the
ultimate aim.
Clearly, this is a long way from parachuting bots into hard-to-reach tumours deep inside a person. But the rising tide of invivo
experiments and the increasing involvement of clinicians suggests that
microrobots might just be leaving port on their long journey towards the
clinic.
Your study design is completely fucking wrong, you're not measuring 100% recovery. Survivors don't want better functional outcome, THEY WANT 100% RECOVERY. Do you never talk to survivors without using your tyranny of low expectations?
Randomized
controlled trials (RCTs) have demonstrated powerful efficacy of
endovascular thrombectomy (EVT) for large vessel occlusion in the
anterior circulation. The effect of EVT for acute basilar artery
occlusion (BAO) in the posterior circulation remains unproven. Here, we
highlight the latest findings of observational studies and RCTs of EVT
for BAO, with a focus on the predictors of functional outcomes, the
limitations of recent RCTs, and critical thinking on future study
design. Pooled data from large retrospective studies showed 36.4%
favorable outcome at 3 months and 4.6% symptomatic intracranial
hemorrhage (sICH). Multivariate logistic regression analysis revealed
that higher baseline NIHSS score, pc-ASPECTS < 8, extensive baseline
infarction, large pontine infarct, and sICH were independent predictors
of poor outcome. Two recent randomized trial BEST (Endovascular
treatment vs. standard medical treatment for vertebrobasilar artery
occlusion) and BASICS (Basilar Artery International Cooperation Study)
failed to demonstrate significant benefit of EVT within 6 or 8 h after
stroke symptom onset. The limitations of these studies include slow
enrollment, selection bias, high crossover rate, and inclusion of
patients with mild deficit. To improve enrollment and minimize risk of
diluting the overall treatment effect, futile recanalization and
re-occlusion, optimal inclusion/exclusion criteria, including enrollment
within 24 h of last known well, NIHSS score ≥ 10, pc-ASPECTS ≥ 8, no
large pontine infarct, and the use of rescue therapy for underlying
atherosclerotic stenosis, should be considered for future clinical
trials.
Introduction
Acute
basilar artery occlusion (BAO) results in ischemia in brainstem,
occipital lobes, and part of the thalami or cerebellum. Without
reperfusion therapy, the rate of mortality or severe disability was as
high as 90% [1, 2]. With intravenous or intra-arterial thrombolysis, the rate of death or dependency decreased to 78% and 76%, respectively [2, 3]. Although successful endovascular thrombectomy (EVT) for acute BAO was reported almost 2 decades ago [4, 5], its efficacy remains unproven.
In
2015, 5 landmark randomized controlled trials (RCTs) demonstrated
powerful efficacy of EVT in patients with acute ischemic stroke (AIS)
from large vessel occlusion in the anterior circulation (AC) within
6–12 h of symptom onset [6,7,8,9,10].
In 2018, DAWN and DEFUSE-3 showed similar efficacy in patients with
salvageable ischemic penumbra within 16–24 h after last known well [11, 12].
These studies also revealed that EVT during extended time window was
not associated with higher risk of symptomatic intracranial hemorrhage
(sICH). The aim of this review was to highlight the latest findings of
EVT for acute BAO and critical thinking on future study designs.
The layperson explanation: Anti-dopaminergic antiemetics, widely used for nausea and vomiting due
to migraine, chemotherapy, radiotherapy, or surgery, raised the risk of ischemic stroke?. (The BMJ)
Be careful out there.
Risk of first ischaemic stroke and use of antidopaminergic antiemetics: nationwide case-time-control study
Correspondence to: A Bénard-Laribière, Service de Pharmacologie Médicale, Hôpital Pellegrin, Bordeaux, France, anne.benard@u-bordeaux.fr
Accepted 15 February 2022
Abstract
Objective To estimate the risk of ischaemic stroke associated with antidopaminergic antiemetic (ADA) use.
Design Case-time-control study.
Setting Data from the nationwide French reimbursement healthcare system database Système National des Données de Santé (SNDS).
Participants
Eligible participants were ≥18 years with a first ischaemic stroke
between 2012 and 2016 and at least one reimbursement for any ADA in the
70 days before stroke. Frequencies of ADA reimbursements were compared
for a risk period (days -14 to -1 before stroke) and three matched
reference periods (days -70 to -57, -56 to -43, and -42 to -29) for each
patient. Time trend of ADA use was controlled by using a control group
of 21 859 randomly selected people free of the event who were
individually matched to patients with stroke according to age, sex, and
risk factors of ischaemic stroke.
Main outcome measures
Association between ADA use and risk of ischaemic stroke was assessed
by estimating the ratio of the odds ratios of exposure evaluated in
patients with stroke and in controls. Analyses were adjusted for time
varying confounders (anticoagulants, antiplatelets, and prothrombotic or
vasoconstrictive drugs).
Results
Among the 2612 patients identified with incident stroke, 1250 received
an ADA in the risk period and 1060 in the reference periods. The
comparison with the 5128 and 13 165 controls who received an ADA in the
same periods yielded a ratio of adjusted odds ratios of 3.12 (95%
confidence interval 2.85 to 3.42). Analyses stratified by age, sex, and
history of dementia showed similar results. Ratio of adjusted odds
ratios for analyses stratified by ADA was 2.51 (2.18 to 2.88) for
domperidone, 3.62 (3.11 to 4.23) for metopimazine, and 3.53 (2.62 to
4.76) for metoclopramide. Sensitivity analyses suggested the risk would
be higher in the first days of use.
Conclusions
Using French nationwide exhaustive reimbursement data, this
self-controlled study reported an increased risk of ischaemic stroke
with recent ADA use. The highest increase was found for metopimazine and
metoclopramide.
Introduction
The
risk of ischaemic stroke with centrally acting antidopaminergic
antipsychotics has been highlighted in large observational studies,
especially in older patients and among people with dementia.123
The risk is considerable at the start of treatment, 12 times higher in
the first month of use, and progressively declines over time and falls
to baseline after three months of treatment.456
Dopamine receptor antagonism is the main determinant of antipsychotic
action. Although antipsychotics also block a variety of other receptors
(muscarinic, histaminergic, serotoninergic, adrenergic), possible
mechanisms by which these drugs might cause stroke could relate to this
dopamine antagonism.6
Research is lacking on the risk of stroke for non-antipsychotic
dopamine receptor antagonists, such as antidopaminergic antiemetics
(ADAs). ADAs are peripheral D2 receptor antagonists with a direct effect
on the chemoreceptor trigger zone, which lies outside the blood-brain
barrier. However, some ADAs, such as metoclopramide, cross the
blood-brain barrier and are also low potency central antidopaminergics.
Moreover, stroke occurrence can be triggered by mechanisms that do not
require any crossing of the blood-brain barrier because blood vessels
are located outside the blood-brain barrier. ADAs are widely used in
general practice for the treatment of nausea and vomiting of different
causes (migraine, chemotherapy or radiotherapy, postoperative). Given
the well known risk of ischaemic stroke associated with antidopaminergic
antipsychotics and the widespread use of ADAs, we assessed the
association between ischaemic stroke and ADAs in a real world setting.
Not going to happen with me, pets would prevent spur of the moment travel and be extremely expensive to board on long vacations. Both of which prevent dementia by increasing social connections. Those social connections are much more important to me than having a pet and I believe more likely to prevent dementia. But I'm not medically trained, so don't listen to me.
Researchers
found that adults ages 50 or older who had owned any kind of pet for
more than five years showed slower decline in verbal memory compared to
non-pet owners. Photo credit: Shutterstock
Our furry, feathered, finned, scaled and shelled animal friends may do more than bring us emotional comfort.
Owning a pet for over five years may help keep cognitive skills sharp
as you age, according to a new study by researchers at the University
of Florida, University of Michigan and Virginia Commonwealth University.
The researchers found that adults ages 50 or older who had owned any
kind of pet for more than five years showed slower decline in verbal
memory — being able to recall words, for example — over time compared to
non-pet owners.
“We can’t show that this is causal but it does show that pets could
buffer or have a protective effect on older adults’ cognition and we
think it has to do with some of the mechanism related to stress
buffering,” said Jennifer Applebaum, a doctoral candidate in sociology
and National Institutes of Health predoctoral Fellow at the University
of Florid. Applebaum is the lead author of the study.
Applebaum said the researchers are not recommending pet ownership as a
therapeutic intervention. However, “an unwanted separation from a pet
can be devastating for an owner and marginalized populations are most
at-risk of these unwanted outcomes,” she said. “We do recommend that
people who own pets be supported in keeping them via public policy and
community partnerships.”
Among policies that could be considered: reducing or eliminating pet
fees in rental housing, foster or boarding support during times of
health crisis or other emergencies and free or low-cost veterinary care
for low-income owners.
This is the first study to examine the impact of pet ownership over
time on cognitive function among a national sample of U.S. adults ages
50 or older. The 1,300 people studied are participants in the Health and
Retirement Study, a longitudinal survey that is tracking 20,000 adults
in the U.S. to learn about aging-related issues.
The average age of those included was 65; 53% owned pets, with nearly
one-third owning pets for more than five years. While all types of pets
were included in the study, dogs were the most prevalent, Applebaum
said, followed by cats.
Over six years, cognitive scores declined slower in pet owners and
was strongest in long-term pet owners. The effect was most pronounced
for White and Black adults, men, adults with advanced degrees and people
with incomes of less than $125,000. More research is needed to fully
explain the findings, Applebaum said.
There are many studies of mental and physical health benefits of pet
ownership, though results have been inconclusive. However, a positive
relationship with a pet is thought to buffer stress via emotional
support, which also may promote healthy cognitive aging. Taking care of a
pet – walking a dog, feeding a cat – also boost physical activity,
which is linked to cognitive health.
“These findings provide early evidence to suggest that long-term pet
ownership could be protective against cognitive decline, providing a
novel and fundamental step to examine how sustained relationships with
companion animals contribute to brain health,” according to the authors.
Applebaum said it is possible that people who owned a pet for less
than five years also experienced other significant stressors or did not
have positive experiences with their pets and so did not reap health
benefits from those interactions.
The research team will present the preliminary study, which is
currently under review for publication, at the American Academy of
Neurology 74th Annual Meeting in April.
Applebaum became interested in issues related to pet ownership and
social inequality while working in animal shelters. She completed a
master’s in veterinary medicine before pursuing her doctorate.
“I am interested the impact of social inequalities on people and
pets,” Applebaum said. “That got me more broadly interested in how pets
impact health and how that plays out in a household between both owners
and pets.”
We've known for years that neuroprotection studies have failed. 1000+ according to Dr. Michael Tymianski, of the Toronto Western Hospital Research Institute in Canada states; over the last half-century, there have been more than 1,000 drugs(So what are they?)aimed at preventing brain damage that have failed to work in people, even though they worked well in mice or rats. If you called it by the correct name, neuronal cascade of death, it sounds like it needs solving immediately rather than the milquetoast term 'neuroprotection'.
1Department of Neurology, The Hague Medical Center, The Hague, Netherlands
2Department of Neurology, Leiden University Medical Center, Leiden, Netherlands
3Department of Radiology and Nuclear Medicine, Erasmus University Medical Center, Rotterdam, Netherlands
4Department of Neurology, Erasmus University Medical Center, Rotterdam, Netherlands
5Department of Neurology, Rijnstate Hospital, Arnhem, Netherlands
6Department of Clinical Neurophysiology, Technical Medical Centre, University of Twente, Enschede, Netherlands
7Department of Radiology, Leiden University Medical Center, Leiden, Netherlands
8Department of Radiology, The Hague Medical Center, The Hague, Netherlands
9Department of Neurology, Amsterdam University Medical Center, Amsterdam, Netherlands
Background: Clinical trials of
neuroprotection in acute ischemic stroke (AIS) have provided
disappointing results. Reperfusion may be a necessary condition for
positive effects of neuroprotective treatments. This systematic review
provides an overview of efficacy of neuroprotective agents in
combination with reperfusion therapy in AIS.
Methods: A literature search was
performed on the following databases, namely PubMed, Embase, Web of
Science, Cochrane Library, Emcare. All databases were searched up to
September 23rd 2021. All randomized controlled trials in which patients
were treated with neuroprotective strategies within 12 h of stroke onset
in combination with intravenous thrombolysis (IVT), endovascular
therapy (EVT), or both were included.
Results: We screened 1,764
titles/abstracts and included 30 full reports of unique studies with a
total of 16,160 patients. In 15 studies neuroprotectants were tested for
clinical efficacy, where all patients had to receive reperfusion
therapies, either IVT and/or EVT. Heterogeneity in reported outcome
measures was observed. Treatment was associated with improved clinical
outcome for: 1) uric acid in patients treated with EVT and IVT, 2)
nerinetide in patients who underwent EVT without IVT, 3) imatinib in
stroke patients treated with IVT with or without EVT, 4) remote ischemic
perconditioning and IVT, and 5) high-flow normobaric oxygen treatment
after EVT, with or without IVT.
Conclusion: Studies specifically testing
effects of neuroprotective agents in addition to IVT and/or EVT are
scarce. Future neuroprotection studies should report standardized
functional outcome measures and combine neuroprotective agents with
reperfusion therapies in AIS or aim to include prespecified subgroup
analyses for treatment with IVT and/or EVT.
Introduction
Intravenous thrombolytic therapy (IVT) has become
standard care for acute ischemic stroke (AIS), but only a small minority
(12%) of patients is eligible for IVT because of the limited time
window and contra-indications (1). The absolute benefit of treatment with IVT is limited and is estimated to be 4–10% (2).
In the last decade, endovascular therapy (EVT) to mechanically reopen
the occluded cerebral artery has led to an improvement of functional
outcome in patients with AIS caused by large vessel occlusion (LVO) (3).
However, despite high recanalization rates (70–90%) chances of good
functional outcome after EVT remain relatively low (30–60%) (3, 4).
Currently only 10% of patients after EVT are without stroke symptoms at
3 months follow-up with a modified Rankin Scale (mRS) score of 0 (3, 5).
This implies the need for additional treatment and systems-based
interventions to further improve recovery of patients with AIS. A wide
range of neuroprotective agents has been investigated in the past to
reduce brain injury and thereby improve patient recovery. Despite
promising results from animal studies, none of the tested
neuroprotective strategies appeared effective in clinical trials (6).
Earlier trials may have failed due to a lack of recanalization in
treating patients with AIS. As ischemic tissue will eventually become
infarcted if blood flow is not restored, adequate reperfusion is
probably a necessary condition for recovery with or without additional
neuroprotective treatments (4, 7–9). The four primary treatment targets are reduction of excitotoxicity, oxidative stress, inflammation, and cellular apoptosis (10). In patients with adequate recanalization, another targeted mechanism is reducing reperfusion injury (7, 11).
With the introduction of IVT and EVT, drugs with neuroprotective
properties can now be investigated in combination with reperfusion
therapy. This systematic review provides an overview of randomized
controlled trials (RCTs) of neuroprotective agents in AIS as an adjunct
to IVT and/or EVT.








 E. M. Vos
E. M. Vos V. J. Geraedts
V. J. Geraedts A. van der Lugt
A. van der Lugt D. W. J. Dippel
D. W. J. Dippel M. J. H. Wermer
M. J. H. Wermer J. Hofmeijer
J. Hofmeijer A. C. G. M. van Es7,8,
A. C. G. M. van Es7,8,  C. M. P. C. D. Peeters-Scholte
C. M. P. C. D. Peeters-Scholte{kind=link}