My conclusion on mobile stroke units is that they are just as big a failure as hospital ER units. Unless you accept the tyranny of low expectations that survival is the only thing worth measuring. If you would actually talk to survivors sometime you might find out they want 100% recovery, and YOU ARE DOING NOTHING TO GET THERE.
These much faster options are available to diagnose stroke, do you know of them?
Maybe you want these much faster objective diagnosis options.
Hats off to Helmet of Hope - stroke diagnosis in 30 seconds; February 2017
Microwave Imaging for Brain Stroke Detection and Monitoring using High Performance Computing in 94 seconds March 2017
New Device Quickly Assesses Brain Bleeding in Head Injuries - 5-10 minutes April 2017
Ski-Mask Design AIR Coil Offers Whole-Brain Imaging Without Claustrophobia
The latest here:
Impact of mobile stroke units
Abstract
Since its first introduction in clinical practice in 2008, the concept of mobile stroke unit enabling prehospital stroke treatment has rapidly expanded worldwide. This review summarises current knowledge in this young field of stroke research, discussing topics such as benefits in reduction of delay before treatment, vascular imaging-based triage of patients with large-vessel occlusion in the field, differential blood pressure management or prehospital antagonisation of anticoagulants. However, before mobile stroke units can become routine, several questions remain to be answered. Current research, therefore, focuses on safety, long-term medical benefit, best setting and cost-efficiency as crucial determinants for the sustainability of this novel strategy of acute stroke management.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Stroke is an important cause of mortality and disability, with severe medical and economic consequences.1 Efficient causal treatments for acute stroke are thrombolysis2 and intra-arterial therapy (IAT),3 however, both are extremely time-sensitive. Many studies showed improved outcomes when delays before treatment were reduced. For example, in the Highly Effective Reperfusion Evaluated in Multiple Endovascular Stroke trial, 10 min earlier thrombectomy estimated to gain 39 disability-free days.4
In addition to decreasing the effectiveness of recanalising strategies, delays also preclude many patients from receiving such treatment at all. This fact is reflected in the low reported rates of treatment: in US registries, approximately 10% of patients who had an acute ischaemic stroke were treated with thrombolysis and approximately 2% with IAT.5 6 The main reasons for treatment delays are related to arriving too late in the hospital for treatment, indicating the urgency for reconfiguration of current systems of care.7
This review focuses on current advances in prehospital stroke treatment and the recently developed mobile stroke units (MSUs) aimed at enabling a timely delivery of acute stroke treatment.
Search strategy and selection criteria
We searched the PubMed database for articles containing the term stroke in combination with prehospital or Mobile Stroke Unit and published between 1 January 2015 and 31 December 2020. The search yielded 787 published articles. We examined these articles with a focus on originality, timeliness and relevance to the scope of this review.
The MSU concept: ‘bringing the hospital to the patient’
At present, acute stroke management guidelines recommend that, after first assessment and stabilisation, patients who had a stroke should rapidly be transported to the nearest stroke-ready hospital for diagnostic work-up and acute treatment.8 9 However, effective treatments are now available that could, in principle, be administered directly at the emergency site. Therefore, in contrast to the current practice of awaiting patients to arrive at the hospital before diagnosis and treatment can begin, a scientific concept for the delivery of stroke treatment directly at the emergency site was first published in 200310 and was first introduced in clinical practice in 2008.11 12 This concept was made possible by the implementation of all required equipment for diagnosis and treatment in an ambulance, including CT, point-of-care (POC) laboratory, telemedicine connection to hospitals and advanced stroke medications.
Apart from a reduction in treatment delays by cutting transport times and reducing the number of crucial interfaces between groups of various healthcare professionals, an equally important advantage of MSUs is the option of diagnosis-based triage decision-making with regard to transport to the individually required target hospital. The MSU, acting synergistically with hospital-based stroke units, was aimed to extend specialised stroke care to the prehospital phase of stroke management.10
Technical aspects
MSU ambulance
The ambulance, the basis of the MSU, varies worldwide with regard to dimensions according to the specific needs of the various regions and healthcare systems. Some MSUs focus on small and lightweight standard solutions, thereby reducing costs, facilitating speed, allowing access to narrow roads and increasing acceptance by Emergency Medical Services (EMS) healthcare professionals, who find their familiar working environment. However, larger vehicles may be advantageous in other specific settings. For example, providing extra space allows relatives to accompany the patient in the MSU to provide history and informed consent for later medical procedures. They may also incorporate larger scanners, and their more robust construction allows coping with challenging street conditions.
Imaging
Imaging is the cornerstone of acute stroke treatment. It provides the answers to two key questions: (1) whether the patient is a candidate for tissue plasminogen activator (tPA), that is, by exclusion of intracranial haemorrhage, and (2) whether the patient should undergo IAT in a comprehensive stroke centre (CSC) because of large-vessel occlusion (LVO). For that reason, cerebral imaging is a main component of the MSU concept.
Although mobile CT scanners dedicated to head imaging and constructed for use in intensive care units and with acceptable resolution (eg, Tomoscan M, Philips, The Netherlands) have been available since the 1990s, they were first placed into an ambulance for prehospital stroke care in 2008.11 A common disadvantage of all mobile head scanners is their inability to scan below the C2 vertebra; such a capability could be relevant for assessing obstructions of proximal neck vessels. However, at present, there is no clear evidence for recanalisation of proximal carotid or vertebral artery occlusions, and no guidelines currently recommend this procedure. One project, carried out in Memphis, Tennessee, USA, uses a whole-body scanner that not only allows scanning of the proximal brain-supplying vessels but also provides higher resolution, although at the expense of a larger size and more weight.13
Whereas unenhanced imaging can already exclude haemorrhage, multimodal imaging, including vascular (CT angiography) and perfusion (CT perfusion) imaging, is crucial for identifying LVO and the tissue at risk. CT angiography in the field has been shown to allow rapid detection of LVO, a precondition for correct decision-making for or against transfer to a thrombectomy-capable stroke centre14–17 (figure 1A,B).

Prehospital unenhanced CT scans (A) and CT angiography images (B) of a patient who had an acute stroke caused by large-vessel occlusion of the left middle cerebral artery (arrow), enabling a triage decision to transport a patient to a CSC for intra-arterial therapy. Prehospital unenhanced CT scanning (C) and CT angiography images (D) of a patient with a hypertensive intracerebral haemorrhage in the basal ganglia with a ‘spot sign’ (arrow), indicating ongoing bleeding and enabling a triage decision to transport to a CSC for neurointensive care. CSC, comprehensive stroke centre.
Automated imaging assessment software
The presence of early infarct signs indicating that ischaemic injury has existed already for some hours is an important predictor of poorer response to thrombolysis and of a higher rate of worse events.18 As a solution to the problem of high inter-rater variability in detecting those signs, the Alberta Stroke Program Early CT Score (ASPECTS) was developed to provide a standardised topographic system for scoring CT scans in acute stroke management.
Because determination of ASPECTS requires substantial experience, automated image analysis tools have been developed more recently.19 During MSU missions, such software can support decision-making for or against thrombolysis in the field, as previously shown.20 Apart from ischaemic brain damage, they may also allow detection of LVO, even on non-contrast CT scans, thereby potentially contributing to improve prehospital triage decision-making.21
Prehospital POC laboratory
MSUs contain a complex POC laboratory for performing laboratory tests in the field. Quantification of haematological, clinical chemistry and coagulation markers can be obtained with small, commercially available portable laboratory devices. Before such equipment was implemented in the MSU, a study showed that the results of POC testing indeed agreed with those of analyses in centralised hospital laboratories.22 The POC laboratory platform can also quantify renal function markers, which are relevant for the performance of CT angiography.16 To the best of our knowledge, only the first randomised trial in Homburg, Germany, performed between 2008 and 2011, placed the same set of POC laboratory devices found in the MSU also in the hospital; this similarity served to improve the comparability of the study groups.14
Telecommunication between MSU and hospital
Telecommunication between the MSU and the hospital is a crucial component of the MSU.23 Telemedical interaction includes real-time bidirectional audio–video communication and exchange of videos, CT scans and other potentially relevant information.10 Telemedicine connection enables the MSU team to obtain valuable guidance from hospital experts.10 11
Commercially available telestroke systems have been refined over time and now allow the transmission of imaging and communication data into the picture archiving and communication system of the hospital.11 After initial problems with connectivity, important improvements in the reliability of telestroke systems have been reported with the establishment of 4G networks. Studies have shown that telemedical assessments were successful for 99 of 100 patients (99%)24 and achieved a success rate of 100% for 11 treated patients.25 A study involving 174 patients compared assessment by a vascular neurologist aboard the MSU and a remote telemedicine-based vascular neurologist. The comparison found 98% satisfactory connectivity and 88% agreement in the decision for or against the administration of tPA.26 A study by Bowry et al,27 involving 50 consecutively assessed patients, found that telemedical consultation of a vascular specialist achieved a level of accuracy for neurological assessment that was comparable with the accuracy achieved by an on-board vascular neurologist, without causing treatment delays. Finally, some studies have described in detail the integration of data generated aboard the MSU into a hospital’s electronic health records.28 29
Staffing and dispatch of MSUs
Because a 100% reliable connection could not be achieved in the initial phase of MSU research, a vascular neurologist trained in the administration of radiation or even a neuroradiologist had to be part of the MSU personnel for compliance with regional regulations. As connectivity improved, it became possible to rely on paramedics, nurses and technicians who were guided remotely by hospital experts via telemedicine.24 However, most projects are still based on the presence of vascular physicians in the MSU.
Because current legal restrictions usually lag behind novel developments, most MSU projects act ‘on top’ to rather than replacing the conventional EMS in response to acute stroke. In some settings, however, MSUs with a vascular physician on-board act alone when the EMS code ‘stroke’ is activated.30 In Norway, MSUs are staffed with anaesthesiologists, trained in stroke medicine.31 32 In general, modalities of interaction between MSU and regular EMS strongly depend on the regional EMS system’s rules, conventions and resources, which are highly divergent.17
Team approach and efficiency at intersections
Whereas in the hospital various members of the stroke rescue chain are subsequently activated and interact, separated by different locations, the MSU staff works at one site, on one patient, and at the same time, in a parallel workflow manner. The fact that treatment in an MSU holds, so far, the ‘world record’ in time to treatment14 can, apart from reduction of transport times, be explained by such highly structured team approach and the considerable reduction of intersections between the various groups of healthcare professionals.
Interaction between EMS and MSU
More in general, to prevent delays and restrict or even completely prevent implementation of an MSU, agreements for cooperation with stakeholders of healthcare systems with competing interests must be settled early in the planning stage of the MSU programme. The legal and procedural obstacles obviously differ widely according to region, healthcare political framework and EMS configuration.
The mode of interaction between a conventional EMS ambulance and MSU is rather heterogeneous in the current programmes. Although nearly all MSU projects act in addition to conventional EMS, an MSU at Southend, UK acts alone.30 Although in most projects (USA, Europe) the MSU is dispatched in parallel to the regular EMS, the MSU can, in addition, also be activated in a tiered manner by the first responding EMS on scene (eg, Houston, Texas, USA). Finally, in some locations the MSU can also be directly activated by the patients or relatives in case of stroke (Bangkok, Thailand).
Identification of stroke during the telephone call from patients or bystanders is a challenge for EMS dispatchers; their reported success rates range from 30% to 83%.17 33 For the dispatch of MSUs, the correct identification of stroke symptoms is crucial. On the one hand, sensitivity must be as high as possible so that strokes are not missed; on the other hand, specificity must also be good so that the number of MSU dispatches to patients who had stroke mimics remains as low as possible. In many regions, stroke recognition in the dispatch office is based on standard questions that are in turn based on stroke scales, such as the Face, Arm, Speech, Time (FAST) Scale, the extended FAST Scale,34 the Dispatcher Identification Algorithm for Stroke Emergencies Scale35 or the Recognition of Stroke in the Emergency Room Scale,14 36 although to date, none of the scales appears to possess sufficiently high sensitivity and specificity.17
Additional
MSUs: prehospital thrombolysis
Evidence
The first randomised trial performed in Homburg, Germany, between 2008 and 2011, found that MSU-based stroke management significantly reduces times to treatment.14 Symptom onset-to-treatment time was 72 min (IQR: 53–108) for the intervention group (MSU) and 153 min (IQR: 136–198, p=0.0011) in the control group (standard care). Alarm-to-therapy decision times were 35 min (IQR: 31–39) for the MSU group and 76 min (IQR: 63–94, p<0.001) for the control group.14 These symptom onset-to-needle times were far superior to those found in all earlier registries or process quality improvement studies, including those with maximally streamlined in-hospital processes resulting in impressive door-to-needle times of even 20 min.23 37 Importantly, treatment quality and patient safety were not reduced when treatment occurred in an MSU.14
Some years later, in 2011, further MSUs hit the road. A pronounced time gain was also observed by a large, randomised study, the Pre-Hospital Acute Neurological Therapy and Optimization of Medical Care in Stroke (PHANTOM-S) Study performed in Berlin, Germany, with median symptom onset-to-treatment times of 81 min (IQR: 56–129)38 and by observational studies in Houston, Texas, USA, with a mean symptom onset-to-treatment time of 98 min,39 and in Cleveland, Ohio, USA, with a median alarm-to-treatment time of 64 min (IQR: 58.3–72.5)40 among other studies in various countries and healthcare environments. The time gains in previous controlled studies are presented in figure 2.

Gains in time from emergency call (left) or symptom onset (right) to treatment or treatment decision conferred by use of mobile stroke units (MSUs) in comparison with standard treatment in various controlled studies. The referring studies were published by (1) Taqui et al,40 (2) Ebinger et al,38 (3) Walter et al,14 (4) Shownkeen et al,55 (5) Kummer et al,56 (6) Grotta et al57 and (7) Ebinger et al.58 tPA, tissue plasminogen activator.
The golden hour in stroke
Stroke physicians adopted the term ‘golden hour’ from trauma surgeons who first described the importance of the very early period after injury for the patient’s chances of survival. Indeed, analysis of an American registry showed that treatment of acute stroke within the golden hour is associated with a higher frequency of discharge to home, freedom from disability at discharge, and reduced rates of in-hospital complications and mortality.41
Before MSUs were implemented, only very few patients who had a stroke could be treated during the first hour: fewer than 1%–2% were treated with thrombolysis during the golden hour in the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study,42 the Safe Implementation of Treatments in Stroke Study43 or the Get With The Guidelines-Stroke registry.41 A ceiling effect in conventional stroke management, associated with transport times and unavoidable intersections between the different groups of healthcare professionals, may explain why treatment during the golden hour is so rare. Until now, only the MSU approach has been able to break this ‘golden hour limit’ for the majority of patients, as was demonstrated by the results of a randomised trial (figure 3).14 Further studies have corroborated this dramatic increase in golden hour treatment with MSUs: the PHANTOM-S trial in Berlin, Germany, in which the rate of treatment within the first 60 min increased from 4.9% to 31%,44 or the MSU project in Houston, Texas, in which 31% of the patients received thrombolysis during the golden hour.25

Rates of therapy decisions for or against thrombolysis (end of all required diagnostic work-up, including laboratory and imaging studies) during the golden hour for patients treated in a mobile stroke unit (MSU) and those given standard treatment in the first randomised trial.14
Treatment of haemorrhagic stroke
There is evidence that the ‘time is brain’ concept is valid for not only ischaemic stroke, but also haemorrhagic stroke. For example, haemorrhage enlargement occurs very early in the course of disease. Clarifying the haemorrhagic cause of stroke by using prehospital CT in MSUs allows appropriate triage decisions with regard to the transfer to specialised centres with neurosurgical services. One study found that on-scene information about presence of the ‘spot sign’ in CT angiography, indicating ongoing haematoma enlargement,45 can be valuable in triage decision-making (figure 1C,D).16 Further, imaging in the field, apart from detection of subarachnoid haemorrhage allowed the detection of its vascular cause itself, a ruptured and still bleeding aneurysm, thereby enabling, after prenotification, to hand over the patient to the neurointerventional team directly in the angiography suite of a CSC.16
Finally, recommendations for blood pressure management differ depending on whether the stroke is of ischaemic or haemorrhagic origin.46 So far, only MSUs due to their imaging capabilities allow differential blood pressure management already on-scene.11 The on-board POC laboratory can also provide relevant information about possible anticoagulant use, thereby allowing reversal of the effects not only of warfarin but also of novel oral anticoagulants such as idarucizumab for dabigatran or andexanet alpha for factor-Xa inhibitors.47 Indeed, in MSUs, feasibility of neutralising effects of dabigatran by idarucizumab has been shown in case of subdural haemorrhage.48 Apart from that, reversal of the effects of dabigatran has also been shown to be feasible for patients who had an ischaemic stroke, thereby enabling subsequent thrombolysis even for previously anticoagulated patients.49
Role in triage of patients who had an acute stroke
Current stroke guidelines recommend that patients who had a stroke should be transported ‘to the closest available stroke centre, or, if no such facility is nearby, to the most appropriate institution that provides stroke care’.8 9 However, for most patients with LVO, the closest hospital is a primary stroke centre (PSC) that cannot offer thrombectomy. This subgroup of patients must be secondarily transferred to a CSC with the capability of performing IAT. This approach is called the ‘drip-and-ship’ concept, in case that a thrombolytic agent is administered in the receiving PSC before secondary transfer to a CSC.17 Importantly, it has been shown that such interhospital transfers cause detrimental delays ranging from 96 min to 111 min.50 Even when the distance between a PSC and a CSC is as small as 15 miles, interhospital transfer times of 104 min have been reported.51
Apart from causing substantial delays before treatment, secondary transfers raise safety concerns due to the difficulty of adequate monitoring of patients during transfers and because of the repeated necessity of additional contrast-enhanced imaging in the target hospital, thereby increasing the risk of renal insufficiency.
In this context, MSUs can be viewed as a triage tool, because on-board vascular imaging detects LVO52 as precondition for correct triage decisions with regard to the appropriate target hospital (figure 4). This assumption was verified in a randomised trial involving 116 patients, which found that the diagnosis of LVO by vascular imaging in the MSU enables correct triage decisions with regard to the appropriate target hospital (PSC vs CSC) with a sensitivity and specificity of 100%, thereby completely abolishing the need for secondary transfer.34
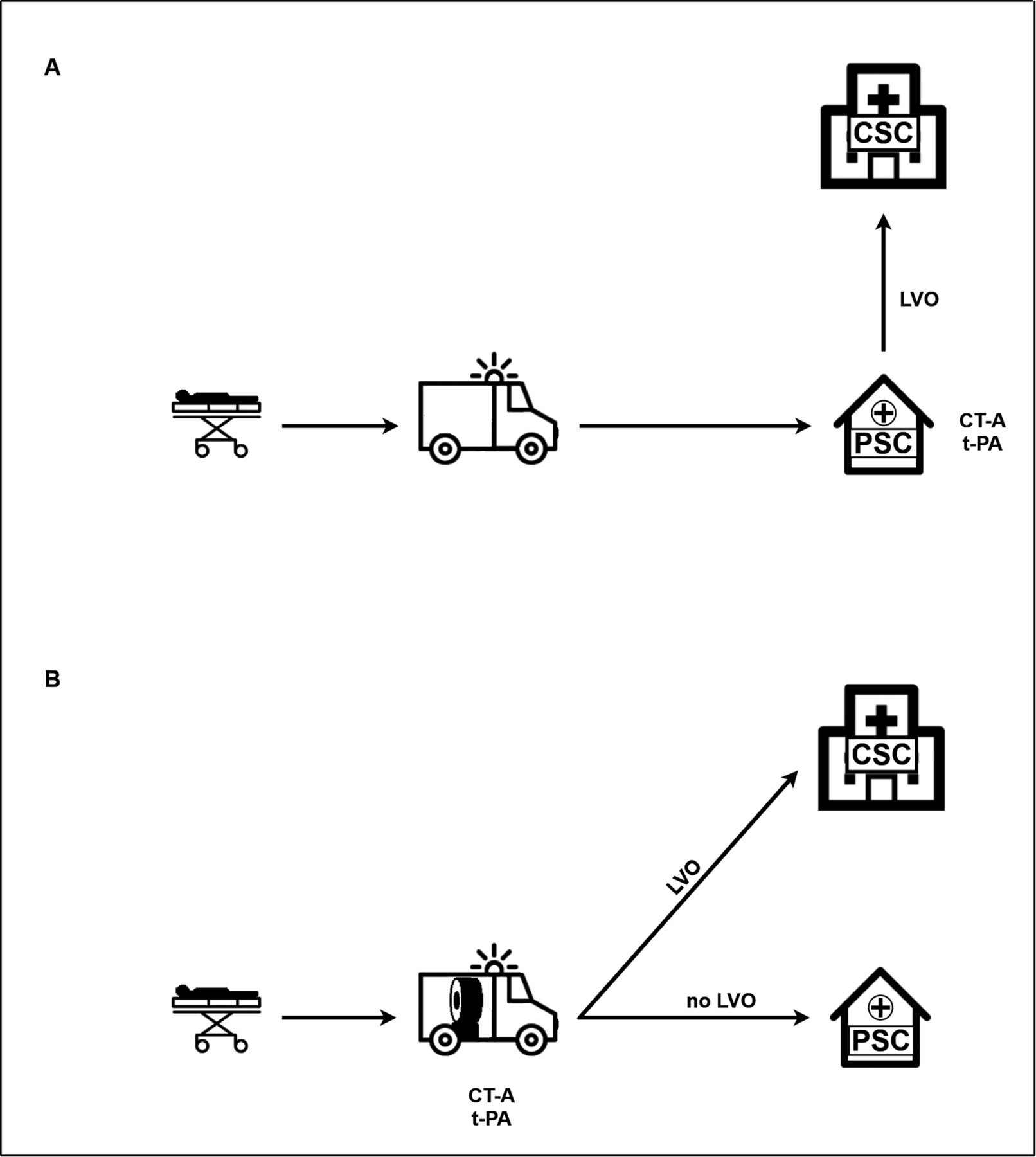
In conventional stroke management, patients are transferred to the nearest stroke centre, which is usually a PSC. In case of presence of LVO, patients are, after thrombolysis, secondarily transferred to a CSC for intra-arterial therapy (‘drip-and-ship concept’) (A). In stroke management with a mobile stroke unit, LVO is diagnosed by vascular imaging on scene, enabling accurate triage decisions with regard to transport to the appropriate target hospital. Secondary interhospital transfers are no longer required (B).34 CSC, comprehensive stroke centre; CT-A, CT angiography; LVO, large-vessel occlusion; PSC, primary stroke centre; tPA, tissue plasminogen activator.
In this regard, Czap et al53 reported that implementation of CT angiography in the field also allows the reduction of in-hospital delays before IAT from 94.5 min (IQR: 69.8–117.3) to 41.0 min (IQR: 30.0–63.5; p<0.001), due to the option of earlier alerting of the endovascular team.
Open questions
Safety
Although the equipment in the MSU and the level of expertise of MSU personnel are similar to those found in hospitals,11 concerns about the safety of MSU treatment have been raised.
Radiation emission by currently used radiation-shielded mobile scanners is within the range of that of fixed scanners in the hospital. A recent study confirmed that the 1-year occupational radiation exposures in MSUs using the Ceretom scanner (Neurologica, Boston, Massachusetts, USA) was 1.14 mSv, similar to the radiation exposure associated with in-hospital scanners and well below the dose limit of 5 mSv.54
Moreover, there are concerns that, in the prehospital arena, thrombolysis may accidentally be administered to patients who had stroke mimics more frequently than in hospitals because of the reduced time for observation of the disease course. This concern is, however, not specific to MSUs but applies to all interventions to improve process quality in stroke management. In the previously reported controlled studies that varied in size of study population, inclusion criteria or dispatch algorithms,14 38 40 55–58 a variable rate of mimics has been reported ranging between 9% and 40.9%; however, those rates were comparable with the respective control group at each study site.
So far, clinical studies have shown that the incidence of complications and the mortality rates among MSU-treated patients are not higher than those among patients treated in hospitals.11 14 24 25 38 59 In the previously reported controlled studies, rates of haemorrhagic complications among patients treated with intravenous tPA in an MSU ranged from 0% to 3.5%, that were, again, similar to those reported for the respective control groups.14 38 40 55–58 In this regard, it has been shown that compared with later thrombolysis, earlier thrombolysis is associated not with higher but, conversely, with lower haemorrhagic complication rates.60 Despite this first evidence, safety endpoints should remain integral components of future MSU studies.
Effects on long-term outcomes
According to the ‘time is brain’ concept, the reduction of delays before treatment is generally considered to translate into better clinical outcomes,2 61 although the first trials were not designed or powered to determine differences in long-term outcomes.14 44
However, a meta-analysis of 11 previous trials involving 6065 patients treated in MSUs found that these patients had a 1.46 greater likelihood of better short-term outcomes than did patients given conventional care in a hospital (p=0.02), although mortality rates did not differ.62 In 2020, a large, non-randomised trial (Berlin Prehospital or Usual Delivery of Acute Stroke Care) performed in Berlin, Germany, found that 749 patients in an MSU group (MSU available) exhibited significantly better modified Rankin Scale (mRS) scores at day 90 than did 794 patients in a conventional treatment group (MSU not available) (OR: 0.74, p<0.005).58 Finally, positive effects on long-term outcomes could be demonstrated in a randomised trial: the Benefits of Stroke Treatment Delivered by a Mobile Stroke Unit Compared to Standard Management by Emergency Medical Services Study was a prospective, multicentre, alternating-week, cluster-controlled trial performed at seven sites in the USA and involved 1047 tPA-eligible patients. The results showed that tPA treatment was administered significantly more frequently and more rapidly to patients in the MSU group: one-third of them were treated within the first, golden hour. Their primary outcome variable was mean mRS score at day 90. The results showed that the mean utility-weighted mRS scores were 0.726 for the MSU group and 0.657 for the group treated in a standard ambulance (difference, 0.069; p=0.002). Thus, on average, for every 100 patients treated in an MSU rather than in a standard ambulance, 27 would have less disability, and 11 of the 27 would be disability-free.57
What is the optimal setting?
The efficiency of MSUs depends on the healthcare system, EMS configuration, legal requirements, market forces and population structure of a specific region.
Moreover, whether the urban, suburban or rural environment is the optimal setting remains uncertain. On the one hand, because the number of dispatches increases with population density, MSUs would appear at first glance to be most beneficial in urban regions. A study performed in a very densely populated area (Manhattan, New York, USA) with a very high density of stroke centres found a time gain of 29.7 min; this time gain was similar to gains found in other, much less populated regions.56 This finding also suggests that a reduction in transport time is only one of several factors contributing to the time gain conferred by MSUs. On the other hand, remote rural regions are often strongly underserved with regard to stroke treatment, and transport delays are the main reason for very low thrombolysis rates in such regions.63 64 The medical value of MSUs, therefore, could be particularly high in such highly disadvantaged regions.34 65 66
Interestingly, as a means of increasing the action radius of MSUs, studies have evaluated a rendezvous concept, involving meeting the regular EMS en route. The MSU in Edmonton, Alberta, Canada, meets the regular ambulance at a predesignated site to reduce travel time, thereby extending the operating radius to as much as 250 km.66 Supporting such a rendezvous concept, a study performed in Houston, Texas, USA found no statistically significant difference in time to treatment between 169 patients transported by such a rendezvous pathway and 169 patients transported by the MSU alone (means±SD: 36.0±10 min vs 37.0±10.0 min, p=0.65).67
Finally, specifically in remote regions, for example, in Australia or Norway, even aircraft equipped with equipment allowing the diagnosis and treatment of acute stroke could be a possible solution for a more equitable distribution of stroke care delivery. A concept and technical solutions for an Air-MSU, in which a helicopter or aeroplane is customised—analogously to MSUs—with a CT scanner, laboratory equipment and telemedicine connectivity, have previously been proposed.68
Computational modelling of potential MSU missions can be supportive in consideration of the most efficient placement of future MSU programmes.69 70 For this aim, even smartphone applications have been developed (https://gntem3.shinyapps.io/ambmc/). Conditional probability modelling studies may also provide important information about the potential superiority of the MSU approach over other approaches, such as the drip-and-ship strategy, in a given region. So far, such estimates have shown that the benefits of MSUs depend mainly on a sufficient dispatch accuracy, the reached reduction of delay before thrombolysis and the process quality in stroke centres.71
Finally, for rational deployment of MSUs, one study involving 195 treated patients addressed the best working time for MSUs. Morning (52.3%) and evening (35.8%) shifts accounted for 88.1% of the MSU missions, whereas night missions accounted for only 11.9%.72 Very few MSUs operate 24/7 so far.73
Are MSUs too expensive?
In contrast to evidence supporting that the best chance of rescuing brain tissue from irreversible damage lies within the first hours and decreases rapidly thereafter, most resources are allocated to the later time after admission to the hospital. In this line, most MSU projects are still not adequately reimbursed but are funded by research grants, hospitals or charity organisations.
In contrast to previous concerns, the first estimation of the cost-effectiveness of an MSU showed a favourable benefit–cost ratio.65 74 Dietrich et al65 calculated a large number of scenarios based on data from the first controlled trial in Homburg, Germany.14 Benefit–cost ratios gradually increased as the number of MSU personnel has decreased (because of telemedicine) and the population density increased. Maximal benefit–cost ratios between 2.16 and 6.85 were found at an optimal operating distance between 26.73 and 40.32 miles, depending on the staff configuration. However, even in rural areas, benefit–cost ratios are higher than 1. This calculation did not even include additional beneficial effects of MSUs, such as correct triage decision-making with regard to LVO, prehospital differential blood pressure management or anticoagulant antagonisation.65
An estimate by Gyrd-Hansen et al,74 based on data from the PHANTOM-S Study in Berlin, Germany,38 found that the annual net cost of MSU deployment (€963 954) was counterbalanced by a healthcare cost gain related to the avoidance of 80 cases of disability, equalling 29.7 quality-adjusted life-years (QALYs). This calculation produced an incremental cost-effectiveness ratio of €32 456 per QALY.
Finally, an economic evaluation based on data obtained from MSU missions in Melbourne, Australia, concluded that 16.90 disability-adjusted life-years (DALYs) could be avoided with improvements in access to thrombolysis and that even 27.94 DALYs could be avoided with earlier access to IAT enabled by deployment of MSUs. Use of the MSU was estimated to cost an additional $A30 982 per DALY avoided.75
There are several options for improving the cost-effectiveness of MSUs in the future: (1) reduction of personnel costs by using telemedicine consultations rather than on-board personnel24 26; (2) better integration of the MSU in routine EMS responses to maximise synergistic effects; (3) reduction of hardware costs by using commercially available standard-ambulance solutions76 and by producing mobile scanners at higher volumes by more market competitors; (4) calculating the ideal number and locations of MSUs needed in a specific region to efficiently serve patients who had a stroke while keeping the number of simultaneous calls at a minimum; (5) using MSUs for traumatic brain injury,77 status epilepticus73 or subarachnoid haemorrhage16 77 78; and, finally, (6) increasing the utilisation rate of MSUs by improving stroke identification algorithms in the dispatch office. However, we can expect that, in the end, decisions about implementation of MSU will be based more on clinical evidence criteria than on explicit cost-effectiveness criteria.
Conclusion and outlook
In conclusion, research into prehospital stroke treatment enabled by MSUs is a young field, which has been rapidly developing over recent years, with an expanding number of projects over the world (figure 5). Although MSUs are still experimental in some locations, their use is nearly routine in others. The proportion of MSU-treated patients worldwide is, however, still small. Further research is needed to define their best placement, their optimal integration into a given healthcare environment, and their long-term medical benefit and cost-effectiveness as a precondition for the sustainability of this concept.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
World map of mobile stroke unit projects.
There is much room for research in further improvement of the MSU concept, for example, the integration of novel diagnostic or therapeutic options that may become relevant in the future (table 1). For example, the use of tenecteplase, a thrombolytic drug that requires only a bolus rather than an infusion, could simplify on-scene treatment while offering similar or even greater effectiveness to alteplase. In addition, the long-standing topic of neuroprotection aimed at attenuating the detrimental cascade of molecular events in ischaemic neuronal injury is currently experiencing a revival in the era of prehospital stroke treatment options. The so far disappointing results of the hundreds of neuroprotection trials may be explained by the delivery of treatment too late and it is currently discussed that the most promising neuroprotective candidates should be re-evaluated when administered much earlier, for example, by use of MSUs.
Potential future diagnostic and therapeutic tools to be used in MSUs
Finally, we can expect that MSUs will strongly profit from future technological advances and from the improvement of connectivity promised by the 5G technology. In support of such research and of collaboration among healthcare professionals active in this field, the Prehospital Stroke Treatment Organization has been founded as a non-profit international consortium open to everyone involved in this field (www.prestomsu.org).
No comments:
Post a Comment