Use the labels in the right column to find what you want. Or you can go thru them one by one, there are only 33,818 posts. Searching is done in the search box in upper left corner. I blog on anything to do with stroke. DO NOT DO ANYTHING SUGGESTED HERE AS I AM NOT MEDICALLY TRAINED, YOUR DOCTOR IS, LISTEN TO THEM. BUT I BET THEY DON'T KNOW HOW TO GET YOU 100% RECOVERED. I DON'T EITHER BUT HAVE PLENTY OF QUESTIONS FOR YOUR DOCTOR TO ANSWER.
Changing stroke rehab and research worldwide now.Time is Brain!trillions and trillions of neuronsthatDIEeach day because there areNOeffective hyperacute therapies besides tPA(only 12% effective). I have 523 posts on hyperacute therapy, enough for researchers to spend decades proving them out. These are my personal ideas and blog on stroke rehabilitation and stroke research. Do not attempt any of these without checking with your medical provider. Unless you join me in agitating, when you need these therapies they won't be there.
What this blog is for:
My blog is not to help survivors recover, it is to have the 10 million yearly stroke survivors light fires underneath their doctors, stroke hospitals and stroke researchers to get stroke solved. 100% recovery. The stroke medical world is completely failing at that goal, they don't even have it as a goal. Shortly after getting out of the hospital and getting NO information on the process or protocols of stroke rehabilitation and recovery I started searching on the internet and found that no other survivor received useful information. This is an attempt to cover all stroke rehabilitation information that should be readily available to survivors so they can talk with informed knowledge to their medical staff. It lays out what needs to be done to get stroke survivors closer to 100% recovery. It's quite disgusting that this information is not available from every stroke association and doctors group.
Friday, July 31, 2020
Cardiac MRI Reveals Post-Recovery Heart Damage in 78 Percent of COVID-19 Patients
Scans show cardiovascular impact lingers after the acute phase of viral infection and into recovery.
MRI
scans reveal that heart damage caused by COVID-19 remains present in 78
percent of patients who test positive for -- and recover from -- the
virus, a new study has revealed.
In an article published July 27 in JAMA Cardiology,
investigators from Germany revealed that the majority of patients who
recover from the viral infection sustain cardiovascular damage
regardless of any pre-existing conditions or their severity of disease.
“The
results of our study provide important insights into the prevalence of
cardiovascular involvement in the early convalescent stage,” wrote the
team led by Valentina Puntmann, M.D., Ph.D., from the Institute for
Experimental and Translational Cardiovascular Imaging at the University
Hospital Frankfurt. “Our findings demonstrate that participants with a
relative paucity of pre-existing cardiovascular condition and with
mostly home-based recovery had frequent cardiac inflammatory
involvement, which was similar to the hospitalized sub-group with
regards to severity and extent.”
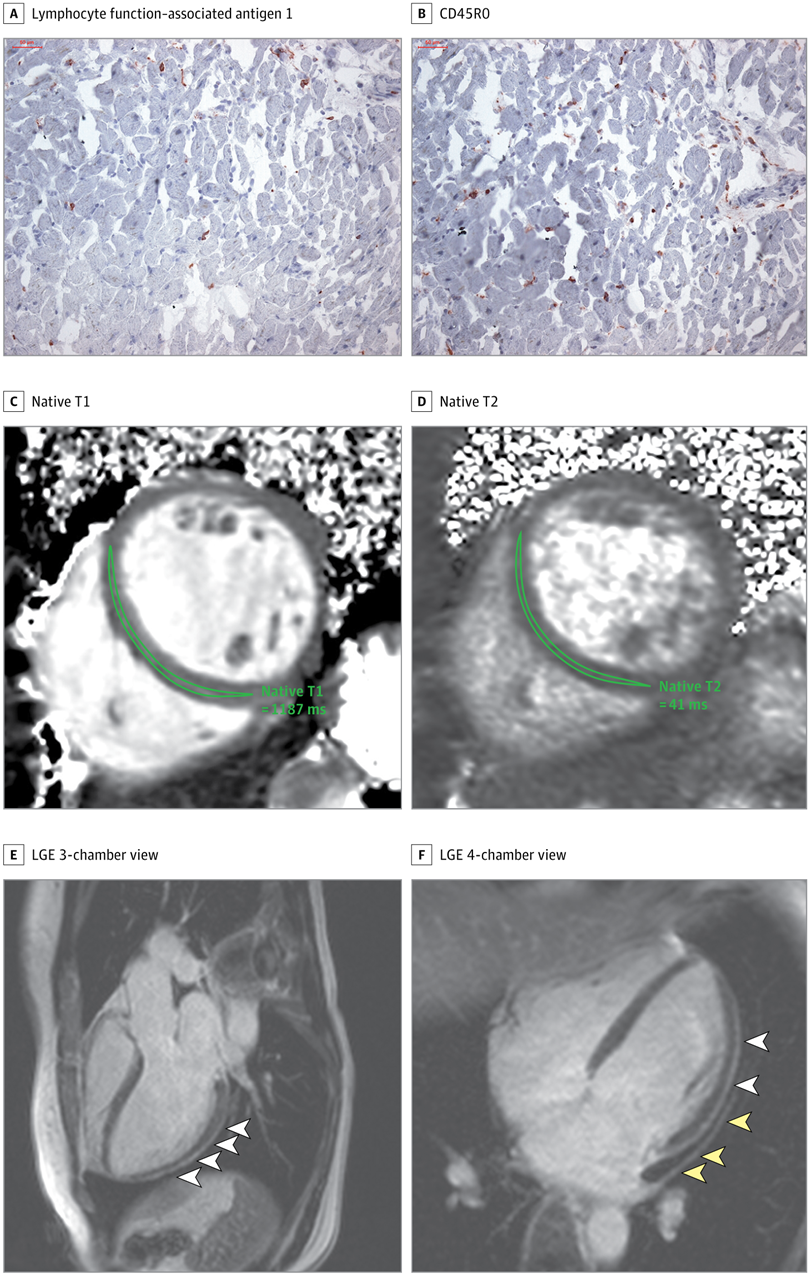
High-sensitivity
troponin T level on the day of cardiac magnetic resonance imaging was
17.8 pg/mL. The patient recovered at home from COVID-19 illness with
minimal symptoms, which included loss of smell and taste and only mildly
increased temperature lasting 2 days. There were no known previous
conditions or regular medication use. Histology revealed intracellular
edema as enlarged cardiomyocytes with no evidence of interstitial or
replacement fibrosis. A and B, Immunohistochemical staining revealed
acute lymphocytic infiltration (lymphocyte function–associated antigen 1
and activated lymphocyte T antigen CD45R0), as well as activated
intercellular adhesion molecule 1. C and D, Cardiac magnetic resonance
imaging revealed enlarged volumes in myocardial mapping acquisitions,
including significantly raised native T1 and native T2. E and F,
Pericardial effusion and enhancement (yellow arrowheads) and epicardial
and intramyocardial enhancement (white arrowheads) were seen on late
gadolinium enhancement (LGE) acquisition. Courtesy: JAMA Cardiology
In
addition, the study analysis revealed that the cardiovascular damage
lingers even after the acute phase of the disease has passed and
patients have begun their recovery. The team identified the presence of
ongoing inflammation in the heart muscle and the heart lining in most
patients, pointing to two potentially dangerous heart conditions –
myocarditis and pericarditis.
Consequently, they said, there is a
need for more research to determine the full extent of the long-term
impacts of COVID-19 on the heart.
To investigate how the virus
affects the heart, Puntmann’s team evaluated 3T MRI scans from an
unselected cohort of 100 patients who had recently recovered from
COVID-19. To their knowledge, this was the first such study. Most
patients (53 percent) were male, the average age was 46, and the
majority (67 percent) recovered at home. The severity of their disease
course varied from asymptomic to severe enough to require
hospitalization. Pre-existing conditions present among all patients
included hypertension, diabetes, previously identified coronary artery
disease, asthma, and chronic obstructive pulmonary disease. No patient
had prior heart failure or cardiomyopathy.
Additionally, compared
to healthy patients, individuals who recovered from COVID-19 experienced
left ventricular ejection fraction, higher left ventricle volumes,
higher left ventricle mass, and raised native T1 and T2, indicating
active inflammatory processes. Among the specific results, 78 percent of
patients had abnormal cardiac MRI findings, including raised myocardial
native T1 in 73 percent of patients and increased myocardial native T2
in 60 percent of patients, as well as detectable high-sensitivity
troponin in 76 percent of patients. Thirty-two percent of patients
experienced myocardial late gadolinium enhancement, and 22 percent saw
pericardial enhancement.
“Our findings may provide an indication
of potentially considerable burden of inflammatory disease in large and
growing parts of the population and urgently require confirmation in a
larger cohort,” the team said. “Although the long-term health effects of
these findings cannot yet be determined, several of the abnormalities
described have been previously related to worse outcome in inflammatory
cardiomyopathies.”
Most of the imaging findings, they said, indicate ongoing perimyocarditis after the acute phase of COVID-19 infection.
There
were limitations to the study, however, the team said. The findings
have not yet been validated with the pediatric patient population, nor
do the results represent patients who have current acute COVID-19
infection.
Even with these limitations, though, the results from
this study are informative, said Clyde Yancey, M.D., chief of cardiology
at Northwestern University Feinberg School of Medicine in an
accompanying editorial.
Not only do they point to the presence of residual left ventricular
dysfunction and sustained inflammation, but they also highlight other
important clinical patho-physiologies, such as clinical syndromes
consistent with acute myocarditis, immunologic responses, and
microvascular clot formation.
“When added to the postmortem
pathological findings [from other studies,] we see that plot thickening,
and we are inclined to raise a new and very evident concern that
cardiomyopathy and heart failure related to COVID-19 may potentially
evolve as the natural history of this infection becomes clearer,” said
Yancey, who is also the deputy editor of JAMA Cardiology. “We
wish not to generate additional anxiety, but rather to incite other
investigators to carefully examine existing and prospectively collect
new data in other populations to confirm or refute these findings.”
Further
investigation of these practical concerns, he said, could continue to
shed light on additional aspects of the COVID-19 crisis.
 In
addition, the study analysis revealed that the cardiovascular damage
lingers even after the acute phase of the disease has passed and
patients have begun their recovery. The team identified the presence of
ongoing inflammation in the heart muscle and the heart lining in most
patients, pointing to two potentially dangerous heart conditions –
myocarditis and pericarditis.
In
addition, the study analysis revealed that the cardiovascular damage
lingers even after the acute phase of the disease has passed and
patients have begun their recovery. The team identified the presence of
ongoing inflammation in the heart muscle and the heart lining in most
patients, pointing to two potentially dangerous heart conditions –
myocarditis and pericarditis.
No comments:
Post a Comment