The problem you are completely missing is that doing nothing in the week after endovascular therapy leaves billions of neurons to die. Endovascular therapy is only the first step, doing nothing after that is incompetence.
From Three-Months to Five-Years: Sustaining Long-Term Benefits of Endovascular Therapy for Ischemic Stroke
 Aravind Ganesh1,
Aravind Ganesh1,  Johanna Maria Ospel2,
Johanna Maria Ospel2,  Martha Marko1,3,
Martha Marko1,3,  Wim H. van Zwam4,
Wim H. van Zwam4,  Yvo B. W. E. M. Roos5,
Yvo B. W. E. M. Roos5,  Charles B. L. M. Majoie6 and Mayank Goyal1,7,8*
Charles B. L. M. Majoie6 and Mayank Goyal1,7,8*- 1Department of Clinical Neurosciences, University of Calgary, Calgary, AB, Canada
- 2Department of Neuroradiology, University Hospital Basel, Basel, Switzerland
- 3Department of Neurology, Medical University of Vienna, Vienna, Austria
- 4Department of Radiology, Maastricht University Medical Centre, Maastricht, Netherlands
- 5Department of Radiology, Amsterdam UMC, Amsterdam, Netherlands
- 6Department of Neurology, Amsterdam UMC, Amsterdam, Netherlands
- 7Department of Radiology, University of Calgary, Calgary, AB, Canada
- 8Hotchkiss Brain Institute, University of Calgary, Calgary, AB, Canada
Background and Purpose: During the months and years post-stroke, treatment benefits from endovascular therapy (EVT) may be magnified by disability-related differences in morbidity/mortality or may be eroded by recurrent strokes and non-stroke-related disability/mortality. Understanding the extent to which EVT benefits may be sustained at 5 years, and the factors influencing this outcome, may help us better promote the sustenance of EVT benefits until 5 years post-stroke and beyond.
Methods: In this review, undertaken 5 years after EVT became the standard of care, we searched PubMed and EMBASE to examine the current state of the literature on 5-year post-stroke outcomes, with particular attention to modifiable factors that influence outcomes between 3 months and 5 years post-EVT.
Results: Prospective cohorts and follow-up data from EVT trials indicate that 3-month EVT benefits will likely translate into lower 5-year disability, mortality, institutionalization, and care costs and higher quality of life. However, these group-level data by no means guarantee maintenance of 3-month benefits for individual patients. We identify factors and associated “action items” for stroke teams/systems at three specific levels (medical care, individual psychosocioeconomic, and larger societal/environmental levels) that influence the long-term EVT outcome of a patient. Medical action items include optimizing stroke rehabilitation, clinical follow-up, secondary stroke prevention, infection prevention/control, and post-stroke depression care. Psychosocioeconomic aspects include addressing access to primary care, specialist clinics, and rehabilitation; affordability of healthy lifestyle choices and preventative therapies; and optimization of family/social support and return-to-work options. High-level societal efforts include improving accessibility of public/private spaces and transportation, empowering/engaging persons with disability in society, and investing in treatments/technologies to mitigate consequences of post-stroke disability.
Conclusions: In the longtime horizon from 3 months to 5 years, several factors in the medical and societal spheres could negate EVT benefits. However, many factors can be leveraged to preserve or magnify treatment benefits, with opportunities to share responsibility with widening circles of care around the patient.
Introduction
Endovascular therapy (EVT) is a highly efficacious treatment for acute ischemic stroke with large vessel occlusion (LVO), promoting post-stroke functional independence (1). Through successful reperfusion of brain tissue, EVT results in lower post-treatment infarct volumes when performed rapidly (2–4). However, fast and successful EVT alone does not guarantee a good outcome. Several critical factors operate in the post-stroke period that can influence the 3-month recovery of the patient. Some are unmodifiable, like advanced age and comorbidities like cardiovascular disease or cancer (Figure 1A) (5). Others are modifiable through attention to the quality of post-acute care, such as the occurrence of post-stroke complications like pneumonia or deep vein thrombosis (5, 6).
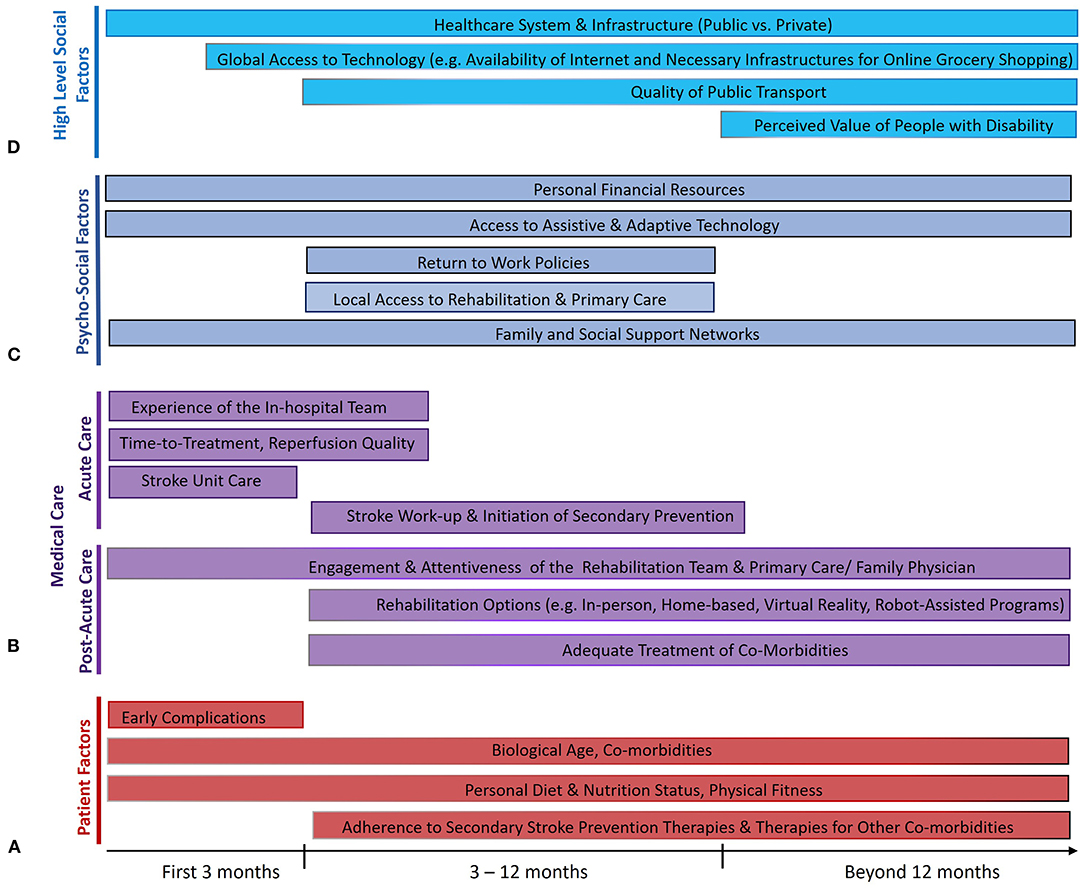
Figure 1. Factors that influence the maintenance of treatment benefits of endovascular therapy (EVT) from 3 months to 5 years after ischemic stroke from large vessel occlusion. Several factors relate to the individual patients themselves (A), some of which are modifiable (like risk of early complications) and rely on effective collaboration between patients and physicians, while several others directly relate to the quality of acute and post-acute medical care (B). Many psychosocioeconomic factors in the life of the patient also play a crucial role (C), as do higher-level societal factors (D) that influence the ability of the patient to reintegrate post-stroke and live a fulfilling life. The length of the bars reflects the portion of the post-stroke time period where each factor is thought to play an important role.
Notwithstanding the various potential pitfalls in stroke recovery from EVT to 3 months, the longer time horizon from 3 months to 5 years is fraught with even greater uncertainty. Some patients may experience further recovery from disability beyond 3 months, while some others successfully maintain their independence, with magnification of treatment-related differences in terms of long-term disability and mortality (7). On the other hand, EVT-related benefits may be eroded by recurrent strokes, accrual of non-stroke-related disability, or by non-stroke-related deaths, especially since stroke occurs more often in elderly people with progressive comorbidities. This raises the question of how we may maximally sustain the initial gains from EVT.
In this review, 5 years after EVT became the standard of care for acute ischemic stroke with LVO, we examine the current state of the literature on 5-year post-stroke outcomes, with particular attention to the modifiable factors that influence the evolution of outcome of the patients between 3 months and 5 years post-stroke. This knowledge may help us better ensure that the therapeutic benefits of EVT are sustained to the greatest possible extent until 5 years post-stroke and beyond.
No comments:
Post a Comment