So if you know when you are going to have a stroke contact your doctor and get this preconditioning protocol done so you have less damage from your stroke.
Review Cerebral Ischemic Tolerance and Preconditioning: Methods, Mechanisms, Clinical Applications, and Challenges
 Yulei Hao
Yulei Hao Meiying Xin
Meiying Xin Liangshu Feng
Liangshu Feng Xinyu Wang
Xinyu Wang Xu Wang
Xu Wang Di Ma* and
Di Ma* and  Jiachun Feng
Jiachun Feng- Department of Neurology and Neuroscience Center, The First Hospital of Jilin University, Changchun, China
Stroke is one of the leading causes of morbidity and mortality worldwide, and it is increasing in prevalence. The limited therapeutic window and potential severe side effects prevent the widespread clinical application of the venous injection of thrombolytic tissue plasminogen activator and thrombectomy, which are regarded as the only approved treatments for acute ischemic stroke. Triggered by various types of mild stressors or stimuli, ischemic preconditioning (IPreC) induces adaptive endogenous tolerance to ischemia/reperfusion (I/R) injury by activating a multitude cascade of biomolecules, for example, proteins, enzymes, receptors, transcription factors, and others, which eventually lead to transcriptional regulation and epigenetic and genomic reprogramming. During the past 30 years, IPreC has been widely studied to confirm its neuroprotection against subsequent I/R injury, mainly including local ischemic preconditioning (LIPreC), remote ischemic preconditioning (RIPreC), and cross preconditioning. Although LIPreC has a strong neuroprotective effect, the clinical application of IPreC for subsequent cerebral ischemia is difficult. There are two main reasons for the above result: Cerebral ischemia is unpredictable, and LIPreC is also capable of inducing unexpected injury with only minor differences to durations or intensity. RIPreC and pharmacological preconditioning, an easy-to-use and non-invasive therapy, can be performed in a variety of clinical settings and appear to be more suitable for the clinical management of ischemic stroke. Hoping to advance our understanding of IPreC, this review mainly focuses on recent advances in IPreC in stroke management, its challenges, and the potential study directions.
Introduction
Cerebrovascular disease is one of the main diseases that lead to human death and disability worldwide, which endangers the health and life of middle-aged and elderly people (1, 2). About 795,000 new or recurrent cerebrovascular diseases occur every year, among which 87% are ischemic cerebrovascular diseases (1). Ischemic cerebrovascular diseases are mainly cerebral infarctions caused by the interruption of cerebral blood flow due to thrombus, embolism, or other reasons in the cerebral blood vessels, resulting in energy metabolism depletion and disorders of ion homeostasis; membrane depolarization; inhibition of high-energy phosphates; cellular potassium efflux; and water, sodium, and chloride influx, followed by a subsequent host cascade of mechanisms, including excitotoxicity, calcium overload, oxidative/nitrative stress, free radical generation, apoptosis, and inflammation, which trigger irreversible brain injury (3). Therein, neurons, glial cells, endothelial cells, and their interconnections are severely damaged and trigger each other in a positive feedback loop and eventually lead to damage and death of nerve cells.
The currently approved treatments for acute cerebral ischemia include the venous injection of thrombolytic tissue plasminogen activator (tPA) within 4.5 h and thrombectomy within 24 h after the appearance of neurological symptoms, which, however, could inevitably induce ischemia/reperfusion (I/R) injury (1, 4). However, the narrow therapeutic window and potential side effects limit their clinical application. In the past few decades, researchers have also carried out a large number of experimental studies on cerebral ischemic neuroprotective agents, but the results were not as expected when these agents were used clinically. Therefore, it is necessary to further fully understand the complex cascade mechanism of its pathological process and advance cost-effective and neuroprotective strategies for ischemic stroke treatment.
Being challenged by nutrient and oxygen deprivation, the brain starts potent endogenous defensive mechanisms against the complex deleterious cascade mechanism, which is also an underlying mechanism leading to irreversible lethal ischemic injury (5). Thus, the endogenous defensive mechanisms that protect the brain against ischemic stimuli and recovers from injury become an increasing hot spot. Ischemic preconditioning (IPreC), referring to a non-injurious and sublethal ischemic insult, can mediate complex endogenous protective mechanisms and provide ischemic tolerance and potent protection against a subsequent, otherwise lethal, ischemia (6, 7). IPreC is considered to be a potential and powerful neuroprotective mechanism that can cope with extreme metabolic stress, such as hypoxia or ischemia, which has aroused great interest in neurological experiments and clinical fields (8). In addition, studies have found a variety of physical and pharmacological stimuli can also induce ischemic tolerance (9–13). Over the past decades, researchers have made significant progress in signifying the endogenous mechanisms of IPreC and in applying the above mechanisms of action to routine clinical practice.
Understanding Cerebral Ischemic Preconditioning
In the past 30 years, ischemic tolerance, as an effective protective strategy for ischemic diseases, has attracted wide attention and in-depth research. According to the time and process of sublethal ischemic injury and ischemic stroke, ischemic tolerance can be divided into the following three types: (1) ischemic preconditioning (IPreC), when sublethal ischemia insult is performed before ischemic disease; (2) ischemic perconditioning, when the ischemic stroke occurs and sublethal ischemia insults should be initiated at the same time; and (3) ischemic post-conditioning, when sublethal ischemia insult is implemented after the ischemic stroke. The above three methods may be involved in different endogenous protective mechanisms. In 1986, Murry et al. first described IPreC in myocardiac tissue, and most IPreC research focused on enhancing the resistance of the myocardium to subsequent fatal ischemic injury (13, 14). Studies have found that ischemic tolerance caused by IPreC is a common phenomenon and can be observed in various organs and tissues, such as heart, central nervous system (CNS), liver, retina, skeletal muscle, kidney, and intestine (15–17). Among them, tissues that are sensitive to hypoxia, such as myocardium, brain, and kidney, are the most promising targets for clinical application of IPreC (17–19).
Initially, an in vitro model of hippocampal slices was used to confirm the adaptability of rat brain tissue to anoxia, which caused wide concern in 1986 (20). In 1989, research showed that brief hypothermia could trigger neuroprotection (21). In 1990, Kitagawa et al. demonstrated that non-lethal ischemic insult could afford sufficient neuroprotection against neuronal death in the hippocampus CA1 region following subsequent lethal ischemic stress (22). In 1991, Kirino et al. also showed protective effect of non-lethal ischemic treatment in a global ischemia model of gerbils (23). During the late 1990s, a large number of research results consistently signified the IPreC-induced neuroprotection against lethal ischemic injury in focal and global cerebral ischemia of different animals (24, 25). One of the disadvantages of IPreC, which cannot be ignored, is that IPreC is capable of leading to serious damage with only small changes in the timing, durations, and location of sublethal ischemic insults (26). Therefore, researchers work tirelessly to find other safe and effective methods to safely induce ischemic tolerance. Remote ischemic preconditioning (RIPreC) is a method in which cerebral ischemic tolerance is induced after a brief short-term I/R duration in distant organs or tissue (27). RIPreC was reported in the myocardium in 1993 (15) and was also confirmed to be neuroprotective against ischemic stroke in 2011 (28).
By now, numerous studies have shown that different inducers/stressors can mediate cerebral ischemic tolerance. In addition to classic mechanical IPreC methods, including local ischemic preconditioning (LIPreC) and RIPreC, there are still many types of endogenous or exogenous stimuli that can induce experimental animals, brain tissue slice and cell cultures develop ischemic tolerance, named cross-preconditioning, mainly including chronic hypoxia (29, 30), hyperoxic or oxidative stress (31), hypothermia or hyperthermia (32), pharmacological treatment and chemical agent application (33–37), cortical spreading depression (38, 39), electroacupuncture (40), sports activity (41), and others [(9, 11, 12); Table 1].
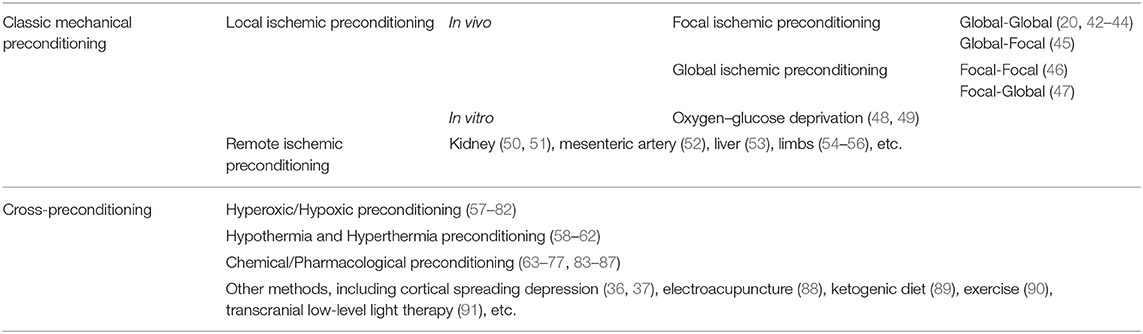
Table 1. Representative reported methods of cerebral ischemic preconditioning.
No comments:
Post a Comment