Highly unlikely this could translate to stroke patients, it was tested on healthy people. And for me since I have no arm swing I could never assist my leg propulsion.
Using a simple rope-pulley system that mechanically couples the arms, legs, and treadmill reduces the metabolic cost of walking
Journal of NeuroEngineering and Rehabilitation volume 18, Article number: 96 (2021)
Abstract
Background
Emphasizing the active use of the arms and coordinating them with the stepping motion of the legs may promote walking recovery in patients with impaired lower limb function. Yet, most approaches use seated devices to allow coupled arm and leg movements. To provide an option during treadmill walking, we designed a rope-pulley system that physically links the arms and legs. This arm-leg pulley system was grounded to the floor and made of commercially available slotted square tubing, solid strut channels, and low-friction pulleys that allowed us to use a rope to connect the subject’s wrist to the ipsilateral foot. This set-up was based on our idea that during walking the arm could generate an assistive force during arm swing retraction and, therefore, aid in leg swing.
Methods
To test this idea, we compared the mechanical, muscular, and metabolic effects between normal walking and walking with the arm-leg pulley system. We measured rope and ground reaction forces, electromyographic signals of key arm and leg muscles, and rates of metabolic energy consumption while healthy, young subjects walked at 1.25 m/s on a dual-belt instrumented treadmill (n = 8).
Results
With our arm-leg pulley system, we found that an assistive force could be generated, reaching peak values of 7% body weight on average. Contrary to our expectation, the force mainly coincided with the propulsive phase of walking and not leg swing. Our findings suggest that subjects actively used their arms to harness the energy from the moving treadmill belt, which helped to propel the whole body via the arm-leg rope linkage. This effectively decreased the muscular and mechanical demands placed on the legs, reducing the propulsive impulse by 43% (p < 0.001), which led to a 17% net reduction in the metabolic power required for walking (p = 0.001).
Conclusions
These findings provide the biomechanical and energetic basis for how we might reimagine the use of the arms in gait rehabilitation, opening the opportunity to explore if such a method could help patients regain their walking ability.
Trial registration: Study registered on 09/29/2018 in ClinicalTrials.gov (ID—NCT03689647).
Background
The mechanical and neural benefits that stem from the natural coordination of the arms and legs during walking have inspired scientists and practitioners to emphasize this natural behavior during gait rehabilitation [1,2,3,4,5,6,7,8,9]. For instance, Behrman and Harkema [2] were the first to exploit the benefit of coordinating the arms' swinging motion with the stepping motion of the legs during treadmill training with body weight support [1, 2]. In a series of case studies, physical therapists would instruct patients to intentionally swing their arms or facilitate their arm motion with hand-held poles [2]. Alternatively, a recumbent stepper or cycle ergometer can allow for an individual to actively coordinate their arm and leg movements while remaining seated. As opposed to the passive arm motion facilitated by hand-held poles, these devices have the added benefit of putting the patient in control. Through this process, individuals can use their arms to modulate the amount and timing of assistance that help drive the motion of their legs, thereby becoming actively engaged in their gait re-training. Experiments studying the training effects of actively coordinating the arms and legs with these devices have shown functional improvements in walking performance in individuals with incomplete spinal cord injury [10] or chronic stroke [11, 12]. The improvements seen in recumbent stepping and cycling may have arisen from exploiting the neural coupling that underlies the coordinated motion of the arms and legs [2,3,4].
While recumbent stepping and cycling have shown benefits, a notable concern is that this type of activity lacks some gait-related task specificity [13]. For example, the recumbent stepping and cycling kinematics of the hip, knee, elbow, and shoulder joints are fundamentally different from walking [5, 13]. Additionally, these devices do not allow the lower limbs to undergo continuous loading and unloading, as done during treadmill training with body weight support. The act of rhythmically loading and unloading the legs is recognized as a critical sensory cue for promoting walking recovery during gait rehabilitation [14, 15]. In order to promote walking recovery, the training task should have similar sensory cues as the goal task [2, 16]. Therefore, developing a strategy where an individual can simultaneously benefit from actively coordinating the arms and legs (as done in recumbent stepping and cycling) and rhythmically loading and unloading the leg during treadmill walking could further optimize task specificity and enhance walking recovery. However, an approach that allows an individual to actively use their arms to drive the motion of their legs during treadmill walking has remained elusive.
To explore this idea, we developed a rope-pulley system that physically links the ipsilateral arm and leg during treadmill walking (Fig. 1). With this approach, we imagined that individuals could use their arms to assist the legs, allowing them to be more actively engaged in their gait re-training. This approach would require a greater demand from the arms, but we suspected this would lower the demand placed on the legs. Therefore, we set out to establish proof-of-concept by first understanding how our method of linking the arms and legs would influence the mechanical, muscular, and metabolic demands of walking in a cohort of healthy, neurologically-unimpaired individuals. We presumed that a user could pull on the rope as the arm swings backward and, thus, generate a force along the rope to assist with ipsilateral leg swing. We reasoned that increasing the muscular demand of the arms would incur a metabolic cost; however, if the assistive force is transmitted effectively along the rope, we expected this assistive force to decrease the muscular and metabolic demand to swing the leg, which is estimated to comprise between 10 and 33% of the net metabolic cost of walking [17,18,19]. Given our logic, we hypothesized that (1) walking with the arm-leg pulley system would increase the arm’s muscular demand to generate an assistive force, but a trade-off would be a decrease in the leg’s muscular demand to swing the leg, and (2) any metabolic cost incurred to actively use the arms would be counterbalanced by the reduction in the cost to swing the legs, bringing about no change in the net metabolic cost of walking. A test of our first hypothesis would provide proof-of-concept that it is possible to actively use the arms to move the legs during treadmill walking. A test of our second hypothesis would give insight into whether this approach comes at the expense of an increased metabolic cost or not. Our overall goal in this study is to provide a fundamental understanding of how physically coupling the arms and legs affects the biomechanics and energetics of walking. We believe this fundamental understanding will provide insight into its potential use as a rehabilitation strategy for individuals with impaired lower limb function, such as those recovering from a spinal cord injury or stroke.
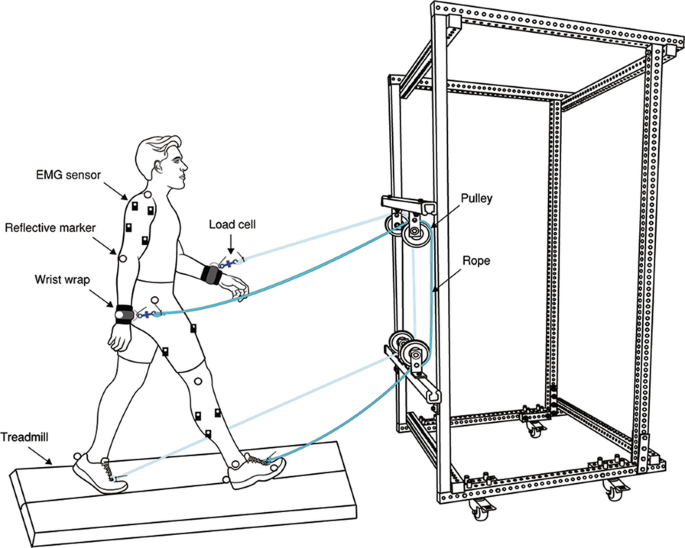
Arm-leg rope pulley system. Subjects walked on a split-belt force measuring treadmill while attached to a simple device that connects the ipsilateral arm and leg using a rope. The horizontal pulley bars are height adjustable, allowing for relative changes in rope length. Furthermore, the load cell is in series with the rope and used to measure rope tension during treadmill walking. Note that the reflective markers were attached to both sides while EMG sensors were placed only on the right side of the body due to a limited number of sensors available in our lab
Methods
Participants
Eight healthy, young subjects participated in this study (3 women and 5 men; age = 23.25 ± 3.37 years, mass = 73.88 ± 18.46 kg, height = 173.84 ± 13.95 cm; mean ± SD). Prior to the experimental session, a telephone interview was conducted to ensure the participants met the inclusion criteria of a healthy participant, i.e., physically active, non-smoker, body mass index < 30.0 kg/m2, and free from musculoskeletal injuries. A health screen form was then completed, reviewed, and signed by the subject the day of the experimental session. In addition, they read and signed an informed consent document. This study was reviewed and approved by the University of Houston Institutional Review Board.
No comments:
Post a Comment