You competent? doctor is closely watching this because of your increased risk of dementia posts stroke! NO? Because your doctor doesn't know of the dementia risk, OR IS TOO FUCKING LAZY TO BE FOLLOWING RESEARCH? Your choice!
Do you prefer your doctor and hospital incompetence NOT KNOWING? OR NOT DOING?
The reason you need dementia prevention:
1. A documented 33% dementia chance post-stroke from an Australian study? May 2012.
2. Then this study came out and seems to have a range from 17-66%. December 2013.
3. A 20% chance in this research. July 2013.
Of course, your incompetent doctor doesn't know about berberine either, right?
The latest here:
Intranasal Delivery of BACE1 siRNA and Berberine via Engineered Stem Cell Exosomes for the Treatment of Alzheimer’s Disease
Authors Sun C, Sha S, Shan Y, Gao X , Li L, Xing C, Guo Z, Du H
Received 15 November 2024
Accepted for publication 6 April 2025
Published 6 May 2025 Volume 2025:20 Pages 5873—5891
DOI https://doi.org/10.2147/IJN.S506793
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lijie Grace Zhang
Chunbin Sun,1,* Shuang Sha,1,* Yubang Shan,1 Xiaoyu Gao,1 Liang Li,1 Cencan Xing,1,2,* Zhongbao Guo,3,* Hongwu Du1,2,*
1School
of Chemistry and Biological Engineering, University of Science and
Technology Beijing, Beijing, 100083, People’s Republic of China; 2Daxing Research Institute, University of Science and Technology Beijing, Beijing, 100083, People’s Republic of China; 3China Testing & Certification International Group Co., Ltd, Beijing, 100024, People’s Republic of China
*These authors contributed equally to this work
Correspondence:
Hongwu Du, School of Chemistry and Biological Engineering, University
of Science and Technology Beijing, Beijing, 100083, People’s Republic of
China, Email hongwudu@ustb.edu.cn Zhongbao Guo, China Testing &
Certification International Group Co., Ltd, Beijing, 100024, People’s
Republic of China, Email gzb@ctc.ac.cn
Introduction:
Alzheimer’s disease (AD) is a common progressive and irreversible
neurodegenerative disease. AD accounts for 60%– 70% of all dementia
cases, ranking as the seventh leading cause of death globally. Human
umbilical cord mesenchymal stem cells (hUC-MSCs) characterized by their
abundant availability and low immunogenicity, have demonstrated
significant therapeutic potential for AD in both preclinical studies and
clinical trials. The use of exosomes can help mitigate the issues
associated with cellular therapies. However, the clinical application of
hUC-MSCs remains challenging due to their inability to effectively
traverse the blood-brain barrier (BBB) and reach pathological sites.
Therapeutic strategies utilizing exosomes derived from hUC-MSCs (Exos)
have emerged as an effective approach for AD intervention.
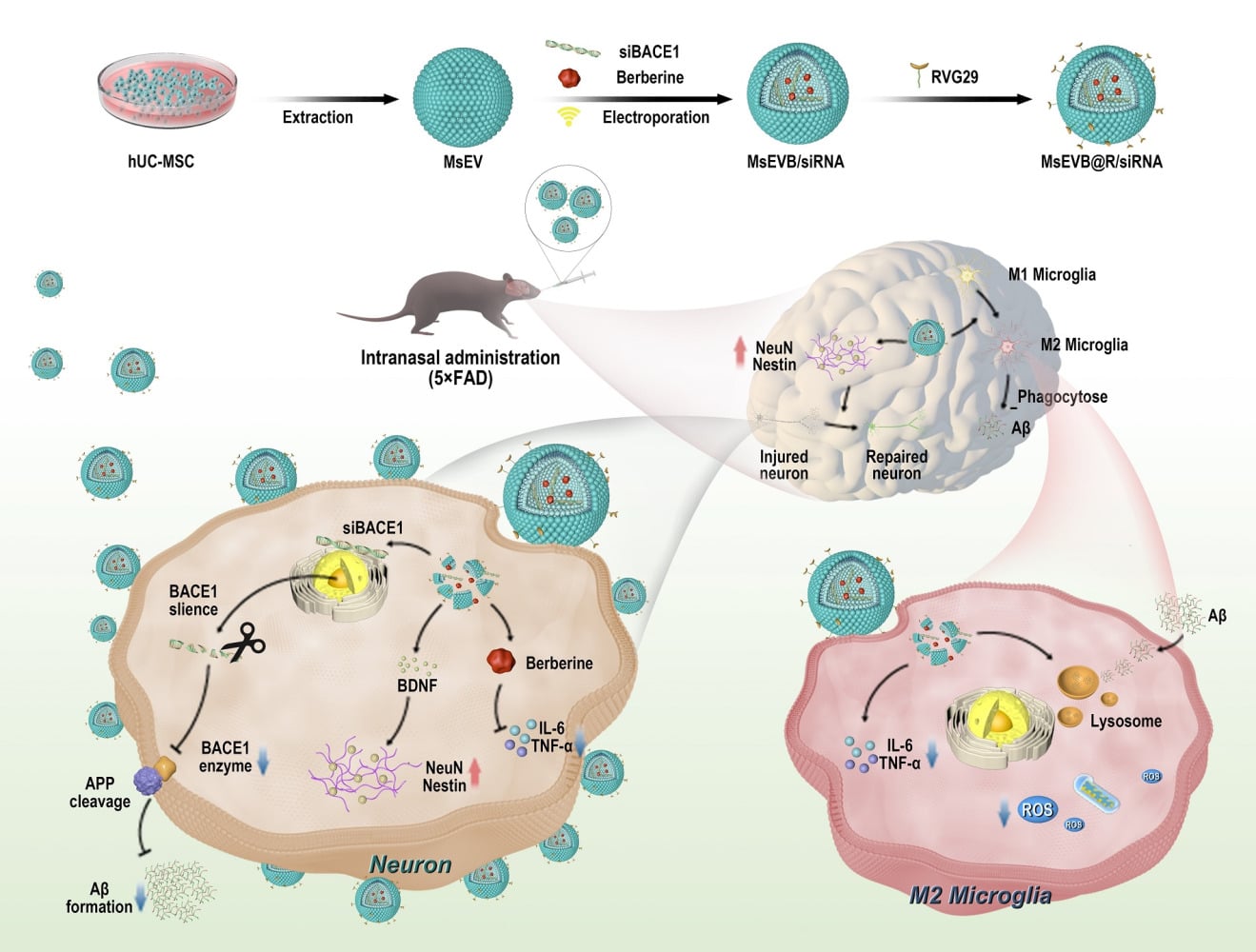
Methods:
Here, we used ultrasound to construct multifunctional Exos
(MsEVB@R/siRNA) for AD therapy. We obtained small interfering RNA for
β-site precursor protein lyase-1 (BACE1 siRNA) and berberine for
co-delivery into the brain. Berberine, a classical anti-inflammatory
agent, effectively alleviates neuroinflammation in AD pathogenesis.
BACE1 serves as the pivotal cleavage enzyme in amyloid β-protein (Aβ)
formation, where silencing BACE1 synthesis through BACE1 siRNA
significantly reduces Aβ production. In a 5xFAD mouse model, Exos
selectively targeted microglial and neuronal cells after nasal delivery
under the action of neural cell-targeting peptide rabies virus
glycoprotein 29 (RVG29).
Results: BACE1 siRNA and
berberine (BBR) loading enhanced the effectiveness of Exos in improving
cognitive function, promoting nerve repair and regeneration, reducing
inflammatory cytokine expression, and suppressing glial responses. BACE1
siRNA release was confirmed to reduce BACE1 expression and Aβ
deposition. Concurrently, berberine effectively suppressed the release
of inflammatory factors, thereby reducing neuroinflammation.
Conclusion: In conclusion, the nasal delivery of engineered exosomes is a potentially effective method for treating AD.
Keywords: Alzheimer’s disease, engineering exosomes, intranasal delivery
Graphical Abstract:
Introduction
Alzheimer’s disease (AD) is a neurodegenerative disease characterized by cognitive dysfunction.1 The primary pathological manifestations in patients with AD are amyloid β-protein (Aβ) deposition, neurofibrillary tangle formation, and neuroinflammation.2,3 Currently, more than 55 million people worldwide are living with dementia. AD accounts for 60%-80% of all cases of dementia and is rapidly becoming one of the leading causes of disability and death among the elderly.4 Projections indicate that AD-related healthcare expenditures will more than double by 2030, escalating from US 1.3 trillion annually in 2019 to US 2.8 trillion. The average annual medical expenditure for AD patients is threefold higher than that of non-AD individuals, necessitating long-term care.5 Furthermore, AD leads to workforce attrition and imposes substantial strain on social welfare systems. The disease also causes progressive memory loss and language impairment, severely compromising verbal communication abilities. AD patients face elevated risks of complications such as dysphagia and infections secondary to prolonged bed rest.6 Current clinical therapeutics for AD include cholinesterase inhibitors (eg, donepezil), N-methyl-D-aspartic acid receptor (NMDA) receptor antagonists (eg, memantine), and monoclonal antibodies like lecanemab. However, the therapeutic outcomes of currently available AD medications remain suboptimal.7 One of the principal contributors to this is the inherent blood-brain barrier (BBB). The BBB protects the brain from harmful substances and pathogens circulating in the blood, maintains a healthy microenvironment, and prevents most drugs from reaching the brain. This structure poses a major challenge in drug delivery for treating of brain diseases. Concurrently, developing drugs that inhibit Aβ production has faced multiple challenges.8,9 Compared with monotherapy, intranasal delivery of exosomes for AD treatment demonstrates enhanced therapeutic efficiency through improved drug bioavailability and reduced dosage requirements. This modality additionally alleviates hepatic and renal metabolic burdens associated with systemic drug administration.10,11 Moreover, the non-invasive nature of nasal administration simplifies clinical procedures, reduces healthcare costs, and improves cost-effectiveness.12,13 Therefore, in addition to continuous investigations on the mechanisms underlying AD, the development of multi-target directed ligand strategies (MTDLS) and one-compound multi-target strategies has great prospects in treating AD.
Cellular exosomes (Exos) are nanoparticles produced by most cells and serve as intercellular transport vehicles for biomolecular cargo from host cells to recipient cells.14 Stem cell-derived Exos have garnered considerable attention owing to their unique properties: less than 200 nm in diameter, they can easily bypass the BBB and protect their contents from degrading lipid biofilms. The abundant biomolecules derived from stem cells, including nucleic acids and metabolites may serve as alternatives to cellular therapeutics.15,16 Evidence suggests that Exos is a major component of transplanted MSCs in AD treatment. Compared to MSC,17,18 MSC-derived Exos has significant advantages, such as cell-free structure, low immunogenicity, specific and convenient delivery route, and ability to carry drugs, making it a suitable alternative for the MSC-based treatment of neurological diseases. Exos may play various roles in AD neuroinflammation, inhibition of Aβ production, nerve regeneration, and axon reconstruction.19,20 To target BBB penetration, nanoparticles capable of receptor-mediated endocytosis are designed to penetrate the BBB and treat brain diseases when administered intravenously. However, owing to the rapid clearance and metabolic changes in the systemic circulation, these drugs are cleared before they can be recognized by the receptor on the BBB, which further reduces the efficiency of the drugs. Thus, intranasal administration is a noninvasive and safe method for drugs to bypass the BBB and directly enter the brain via olfactory nerve axons or connective tissue surrounding the olfactory tract. Recent studies have shown that Exos can reach the hippocampus and play a neuroprotective role in the hippocampus when administered via the nasal route.21,22
AD involves multiple etiologies, including but not limited to Aβ deposition and neuroinflammation. Aβ is expressed at high levels in the brain of patients with AD and aggregates into toxic oligomers and fibers produced by the beta-secretase cleavage of amyloid precursor protein (APP). These aggregations trigger events that lead to neuronal damage and necrosis.23 In addition, the disease-related state of microglia M1 exacerbates neuroinflammation in the brain, impeding the clearance of toxic substances, including Aβ and tau, and further aggravates the disease.24,25 Combination drugs that block these pathways help slow the progression of AD. Small interfering RNA for β-site APP lyase-1 (BACE1 siRNA) downregulates the expression of β-secreting enzyme and reduces the synthesis of Aβ from the source. The inflammation suppressant berberine is then delivered in combined form in the microglia to suppress the cellular inflammatory state and help clear Aβ and tau proteins. Due to its anti-inflammatory effects, berberine can reshape the inflammatory microenvironment and alleviate AD symptoms.26
More at link.
No comments:
Post a Comment