I can't imagine many hospitals buying this and if it doesn't get you back to 100% walking in the hospital there really is no reason to use it.

The effect of pelvic movements of a gait training system for stroke patients: a single blind, randomized, parallel study
Journal of NeuroEngineering and Rehabilitation volume 18, Article number: 185 (2021)
Abstract
Background
Aging societies lead to higher demand for gait rehabilitation as age-related neurological disorders such as stroke and spinal cord injury increase. Since conventional methods for gait rehabilitation are physically and economically burdensome, robotic gait training systems have been studied and commercialized, many of which provided movements confined in the sagittal plane. For better outcomes of gait rehabilitation with more natural gait patterns, however, it is desirable to provide pelvic movements in the transverse plane. In this study, a robotic gait training system capable of pelvic motions in the transverse plane was used to evaluate the effect of the pelvic motions on stroke patients.
Method
Healbot T, which is a robotic gait training system and capable of providing pelvic movements in the transverse plane as well as flexion/extension of the hip and knee joints and adduction/abduction of the hip joints, is introduced and used to evaluate the effect of the pelvic movement on gait training of stroke patients. Gait trainings in Healbot T with and without pelvic movements are carried out with stroke patients having hemiparesis.
Experiment
Twenty-four stroke patients with hemiparesis were randomly assigned into two groups and 23 of them successfully completed the experiment except one subject who had dropped out due to personal reasons. Pelvis-on group was provided with pelvic motions whereas no pelvic movement was allowed for pelvis-off group during 10 sessions of gait trainings in Healbot T. Electromyography (EMG) signals and interaction forces as well as the joint angles of the robot were measured. Gait parameters such as stride length, cadence, and walking speed were measured while walking on the ground without assistance of Healbot T after gait training on 1st, 5th, and 10th day.
Result
Stride length significantly increased in both groups. Furthermore, cadence and walking speed of the pelvis-on group were increased by 10.6% and 11.8%. Although interaction forces of both groups except the thighs showed no differences, EMG signals from gluteus medius of the pelvis-on group increased by 88.6% during stance phase. In addition, EMG signals of biceps femoris, gastrocnemius medial, and gastrocnemius lateral of the pelvis-on group increased whereas EMG signals of the pelvis-off group except gastrocnemius lateral showed no difference after gait trainings.
Conclusion
Gait training using a robotic gait training system with pelvic movements was conducted to investigate the effects of lateral and rotational pelvic movements in gait training of stroke patients. The pelvic movements affected to increase voluntary muscle activation during the stance phase as well as cadence and walking speed.
Clinical trial registration
KCT0003762, 2018-1254, Registered 28 October 2018, https://cris.nih.go.kr/cris/search/search_result_st01_kren.jsp?seq=14310<ype=&rtype=
Introduction
As society is getting aged, the number of stroke patients is increasing [1]. By 2030, 70 million stroke patients and 12 million deaths by stroke in the world are anticipated [2, 3]. As a consequence, increased number of stroke patients have suffered from loss of gait function, which is essential for activities of daily living (ADL’s) [4].
Conventional therapies to recover the gait function impose physical load to the therapists as well as economical burden to the patients. In addition, the outcomes of gait training are often limited by inaccurate gait patterns and incorrect assessment of the patients [5, 6]. In order to reduce the burdens, robotic gait training systems have been studied and used [7, 8]. These robotic gait training systems effectively increased the time and intensity of training, which is crucial for better rehabilitation outcomes. Despite the increased time and intensity of training, however, reduced muscle activation was observed if the subjects remained completely passive in those gait training systems [9]. In order to overcome this drawback, several research activities have improved not only by control but also through modification of existing devices or creation of new devices to increase the level of participation of the patients by giving the patients a certain amount of freedom to change trajectories of the gait training systems [10,11,12,13,14].
Further improvements have been made to include pelvic movements in the transverse plane, which were excluded in the early designs due to higher complexity and costs to build the gait training systems. However, since lateral and rotational pelvic movements, which are two of the six determinants of walking [15], are responsible for balancing and weight-shifting during walking and increasing stride length [16,17,18], it is natural to include those movements for better gait training. Therefore, the lateral and rotational pelvic movements have been added in recently developed robotic gait training systems. Banala et al. added passive joints to a gait training system to allow lateral and rotational pelvic movements [19]. The passive joints including the ones allowing lateral and rotational movements in the transverse plane were held with springs to allow pelvic movements during gait training. In other cases, series elastic actuators were used to actuate an exoskeleton capable of providing translational and lateral movements in the transverse plane as well as joint rotation in the sagittal plane [20,21,22]. The experiments involving healthy subjects in these systems showed similar muscle activation compared to treadmill walking. However, the effects of the pelvic movements were not studied in depth. FreeD, which was an optional module to allow pelvic movements, was added to the Lokomat to accommodate more physiological gait patterns [18, 23, 24]. When compared to the case without the module, less compensatory movements of the trunk were observed when the pelvic motion was added. Hence, more natural gait patterns were obtained during training with less compensatory movement of the trunk.
In this study, Healbot T, which is a gait training system capable of providing pelvic movements, is introduced. The concept and feasibility of Healbot T was introduced in the previous studies and the effect of the pelvic movements on healthy people using a gait training system called COWALK-I was presented in [25, 26]. Healbot T, which was developed and improved from COWALK-I, was used to study the effect of pelvic movements during gait training of stroke patients with hemiparesis. The patients were randomly divided into two groups and asked to walk in Healbot T. During gait trainings, one group was provided with pelvic movements whereas the other group walked without pelvic movements. The group with pelvic motions showed increased muscle activation during the stance phase while interaction forces at the pelvis showed no significant difference. Stride length in both groups increased whereas cadence and walking speed of the pelvis-on group increased by 10.6% and 11.8%.
Healbot T
Healbot T is a gait training system designed for patients with stroke. It consists of an exoskeleton robot, a body weight support (BWS) system, a gravity compensator, and footplates, see Fig. 1.
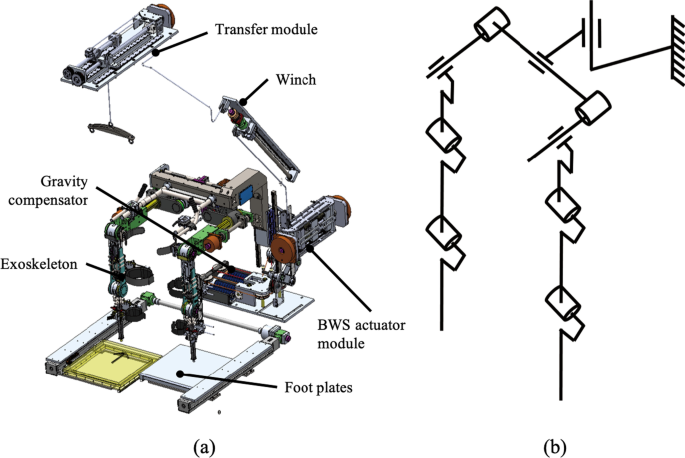
a Designed Healbot T. Healbot T consists of a lower limb exoskeleton robot with 9 active DoF and 1 passive DoF, a BWS system, a gravity compensator, and foot plates. b Schematics of Healbot T, which has 9 active joints and 1 passive joint for vertical displacement
The exoskeleton robot is designed to provide pelvic movements. It has 9 active joints, which are three prismatic joints for translational and rotational movements in the transverse plane and six rotational joints for adduction/abduction at the hip joint and extension/flexion of the hip and knee joints, and 1 passive joint for vertical displacement. For the rotational joints, six identical BLDC motors (K064050-EY2, Parker) with harmonic gear reducers (SHG-20-100-2SO, HDS) are used. Three prismatic joints are actuated with three identical BLDC motors (K089200-7Y2, Parker) with lead-screws to generate lateral, forward, and rotational pelvic movements in the transverse plane. Positions of the actuated joints are measured using absolute encoders (EQI-1131, Heidenhain) attached to the shaft of the motors.
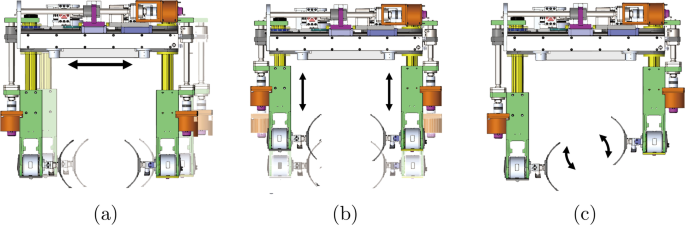
Pelvic movement generated with three prismatic joints a Lateral movement, b forward movement, c rotational movement
Pelvic movements in the transverse plane are generated using three prismatic joints. Lateral movement is generated by the prismatic joint in the center of the exoskeleton. Forward and rotational movements are produced by the prismatic joints at both sides. See Fig. 2.
The braces for securing the patients are located at the pelvis, thighs and calves of the exoskeleton. Force sensors (UMM31-K100, Dacell) are installed between the exoskeleton and the braces to measure the interaction forces. The footplates are synchronized to the horizontal position of the patients. In order to ensure safety, each joint angle is kept within a preset range of motion by mechanical and programmable limits.
The BWS system is designed for supporting the subjects having difficulty in controlling their trunk positions. The BWS system consists of an actuator module, a winch, and a transfer module as shown in Fig. 1.
Since the weight of the exoskeleton imposes physical burden to the subjects wearing the exoskeleton robot and adverse effect on the gait [27], a gravity compensator is designed to support the weight of the exoskeleton. The weight of the exoskeleton is supported by linear springs instead of counter masses to reduce the inertial effect on the exoskeleton. Using a 4-bar linkages and cable, the supporting force generated by the springs remains constant regardless of the position of the exoskeleton.
More at link.
No comments:
Post a Comment