But are the exercises being monitored delivering 100% recovery? If not, why are you supporting the tyranny of low expectations that survivors jest have to deal with limited recovery?
Design, development, and evaluation of an interactive personalized social robot to monitor and coach post-stroke rehabilitation exercises
User Modeling and User-Adapted Interaction (2023)
Abstract
Socially assistive robots are increasingly being explored to improve the engagement of older adults and people with disability in health and well-being-related exercises. However, even if people have various physical conditions, most prior work on social robot exercise coaching systems has utilized generic, predefined feedback. The deployment of these systems still remains a challenge. In this paper, we present our work of iteratively engaging therapists and post-stroke survivors to design, develop, and evaluate a social robot exercise coaching system for personalized rehabilitation. Through interviews with therapists, we designed how this system interacts with the user and then developed an interactive social robot exercise coaching system. This system integrates a neural network model with a rule-based model to automatically monitor and assess patients’ rehabilitation exercises and can be tuned with individual patient’s data to generate real-time, personalized corrective feedback for improvement. With the dataset of rehabilitation exercises from 15 post-stroke survivors, we demonstrated our system significantly improves its performance to assess patients’ exercises while tuning with held-out patient’s data. In addition, our real-world evaluation study showed that our system can adapt to new participants and achieved 0.81 average performance to assess their exercises, which is comparable to the experts’ agreement level. We further discuss the potential benefits and limitations of our system in practice.
1 Introduction
As the world’s older population continues to grow at an unprecedented rate, the current supply of care providers is insufficient to meet the current and ongoing demand for care services (Dall et al. 2013). Researchers have explored an opportunity of socially assistive robots (Feil-Seifer et al. 2005; Tapus and Mataric 2006) that aim to enable people with cognitive, sensory, and motor impairments or assist the clinical workforce (Riek 2017). One potential application is socially assistive robots for rehabilitation therapy (Matarić et al. 2007; Lee et al. 2020, 2022). During rehabilitation, patients require completing a significant amount of self-directed exercises (O’Sullivan et al. 2019; Lee et al. 2022). However, low treatment adherence is a problem across several healthcare disciplines of physiotherapy (Kåringen et al. 2011). To address these problems, there has been increasing attention on social robot coaching systems (Riek 2017; Matarić et al. 2007; Lee et al. 2020, 2022). These systems autonomously monitor patients’ exercises and provide encouragement to support patients’ engagement in well-being-related or rehabilitation exercises through social interaction (Tapus et al. 2007; Feil-Seifer et al. 2005).
Prior work on robotic exercise coaching systems has demonstrated that older adults or post-stroke subjects can successfully exercise and stay engaged with a robot over sessions (Fasola and Matarić 2013; Görer 2013). However, despite the potential of a robot to monitor and guide exercises, prior work is limited to providing generic, predefined corrective feedback on patient’s exercise performance (e.g., checking angular difference with the prespecified motion (Görer 2013; Fasola and Matarić 2013; Guneysu and Arnrich 2017)). It is still challenging to empower a social robot exercise coaching system to generate tailored corrective feedback on an individual patient’s motion (Görer 2013) and adopt these systems broadly yet.
In this work, we design, develop, and evaluate a socially assistive robot coaching system that automatically monitors and coaches physical rehabilitation therapy. Specifically, we selected a test domain as stroke, which is the second leading cause of death and disability (Feigin et al. 2017). We then conducted interviews with therapists to design and develop a socially assistive robot coaching system. This system integrates a machine learning (ML) model with a rule-based (RB) model and can be tuned with held-out user data to assess the performance of exercises for personalized post-stroke therapy (Fig. 1a) (Lee et al. 2020). Building upon the previous work (Lee et al. 2020), we demonstrated the benefit of our approach to adapt a new user and provide personalized assessment compared to the commonly used transfer learning technique on a feed-forward neural network model (Zhuang et al. 2020) (i.e., pretrains a model using the dataset from post-stroke survivors and then fine-tune it based on the data from a new post-stroke survivor).
During the real-world study with ten participants, our interactive system can be adapted to new participants and achieved 0.81 average performance to assess participants’ quality of motion, which is comparable to experts’ agreement level (i.e., 0.80 average performance). Overall, participants expressed positive opinions on our system to monitor and provide feedback on their exercises, but also described practical issues to be improved.
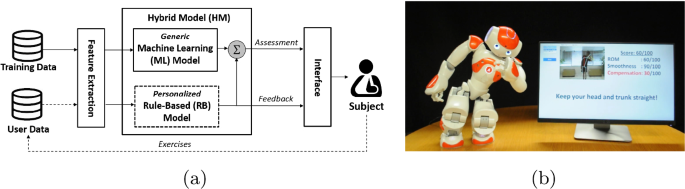
a Flow diagram of an interactive approach of a socially assistive robot for personalized physical therapy. b a setup of the system with a visualization interface and a socially assistive robot that provides corrective feedback (e.g., audio, visual, gestures of the robot)
No comments:
Post a Comment