Well shit, the solution to this is protocols that if they aren't followed lead to firings. Patients could easily ensure they are being followed by just looking in the publicly available database of them when we get survivors in charge.
When neglect is neglected: NIHSS observational measure lacks sensitivity in identifying post-stroke unilateral neglect
- Margaret Jane Moore,
- Kathleen Vancleef,
- Nir Shalev,
- Masud Husain,
- http://orcid.org/0000-0003-0416-5147Nele Demeyere
Author affiliations
Introduction
Unilateral
visual neglect is characterised by lateralised spatial–attentional
deficits, resulting in dramatic behavioural impairments.1
Neglect negatively impacts functional outcome and needs to be
successfully detected in order to inform neglect-specific as well as
general post-stroke rehabilitation goals and strategies. It is therefore
critically important to evaluate current clinical methods for detecting
and measuring the extent of this syndrome.
Observational
neurological assessments, such as the National Institutes of Health
Stroke Scale (NIHSS), rely predominantly on subjective impression of
impairment levels rather than objective measurements.2
Although the NIHSS was not designed as an individual diagnostic tool,
it is frequently employed as one. However, previous research has
suggested that observational assessments may not be sufficiently
sensitive to visual neglect.2–4
The purpose of this study was to evaluate the diagnostic sensitivity of
the NIHSS’ visual neglect item compared with a brief neuropsychological
cancellation test and to identify factors which modulate this
sensitivity.
Methods
428
patients who had an acute stroke (mean age, 71 (SD 12.8); mean time
post-stroke, 7.3 days (SD 7.4)) completed the NIHSS and Oxford Cognitive
Screen (OCS) Cancellation Task (mean interval, 1.2 days). 63.1% of
patients completed both tests on the same day and the NIHSS was
administered first in 33.9% of cases. The NIHSS Extinction/Inattention
and Visual Field items were considered in this investigation, with
Extinction/Inattention scores of 0 (none), 1 (mild) or 2 (profound) and
Visual Field scores of 0 (normal), 1 (partial) or 2 (complete).
The OCS is a brief stroke-specific cognitive screen which includes a highly sensitive Cancellation Task.5
This test was therefore used as the comparison standard for NIHSS
sensitivity calculations. In this Cancellation Task, patients are
instructed to search for and mark complete heart outlines while ignoring
incomplete hearts. Egocentric neglect was scored by subtracting the
number of targets identified on the left and right side of the page
while allocentric neglect was scored by subtracting the number of
right-gap and left-gap hearts identified. Egocentric asymmetries larger
than 3 and allocentric asymmetries greater than 1 represent significant
impairment.5
Results
First,
the sensitivity of the NIHSS to neglect was evaluated. 83/428 (19.4%)
and 199/428 (46.5%) patients exhibited neglect as reported by the NIHSS
and OCS, respectively. In comparison with the OCS, the NIHSS exhibited a
high neglect specificity (91.2%), though a low sensitivity (31.6%).
Interestingly, the Extinction/Inattention Item was not found to be
significantly more sensitive to neglect than the Visual Field Item
(sensitivity, 28.1%; McNemar’s, χ2=0.735, p=0.39).
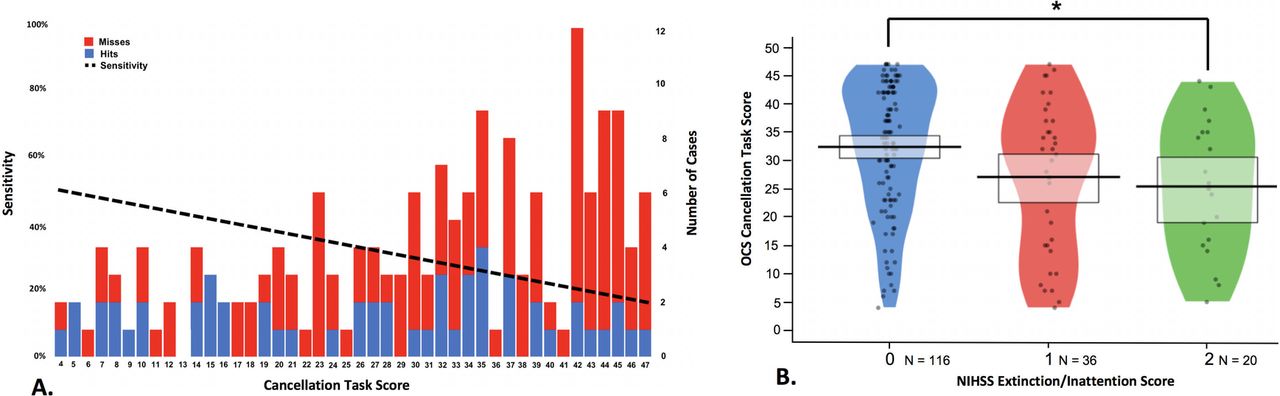
Next, the relationship between NIHSS sensitivity and neglect severity was investigated (figure 1).
A regression analysis demonstrated that patients with milder neglect on
the OCS cancellation were significantly less likely to be identified by
the NIHSS than patients with more severe neglect (R2=0.107,
F(1,42)=5.016, p=0.030, β=−0.327). Similarly, there was a significant
difference in cancellation total for neglect patients with different
Extinction/Inattention Item scores (F(2,169)=4.777, p=0.010). However,
there was large individual variability in all NIHSS item severity
categories and the NIHSS was still found to have a low sensitivity
(38.1%) when only the most severe neglect patients (cancellation totals
<10/50) were considered.
{kind=link}
Figure 1
(A)
Illustration of the relationship between cancellation score and
National Institutes of Health Stroke Scale (NIHSS) sensitivity. The
number of neglect cases of each severity level is denoted by bar height
(right y-axis). Cases which were successfully identified by the NIHSS
are blue and missed cases are red. The sensitivity linear regression
line is plotted as the dashed line. (B) Relationship between NIHSS
Inattention/Extinction Score and Oxford Cognitive Screen (OCS)
Cancellation Task score egocentric neglect patients. Score distribution
is represented by plot width, points represent individual cases, and
rectangles represent upper and lower quartiles. Lower cancellation
scores represent more severe neglect. *p<0.05.
No comments:
Post a Comment