What a FUCKING SHITSHOW! Guidelines; NOT PROTOCOLS! Doesn't anyone in stroke have a functioning brain?
Send me personal hate mail on this: oc1dean@gmail.com. I'll print your complete statement with your name and my response in my blog. Or are you afraid to engage with my stroke-addled mind? No excuses are allowed! You're medically trained; it should be simple to precisely state EXACTLY WHY you aren't working on 100% recovery protocols with NO EXCUSES! I've never received any communications from any stroke association. You'd think they would want to talk to their fiercest critic, but no, they are hiding under a rock someplace, probably don't even know I exist! Swearing at me is allowed, I'll return the favor. Don't even attempt to use the excuse that brain research is hard.
Breaking Down the 2026 Acute Ischemic Stroke Guidelines

Acute ischemic stroke (AIS) occurs when a cerebral artery becomes suddenly occluded, leading to interruption of blood flow and oxygen delivery to brain tissue. It accounts for approximately 85% of all strokes and represents a neurologic emergency in which rapid diagnosis and treatment are critical to preserving brain function and reducing long-term disability.¹
The recently published stroke guidelines, developed and maintained by the American Heart Association in collaboration with its stroke-focused division, the American Stroke Association, were written by experts in vascular neurology, emergency medicine, neurointervention, neurosurgery, neuroradiology, and rehabilitation medicine. Final documents underwent peer review and were published in the journal Stroke to support evidence-based stroke care across diverse health care settings.²
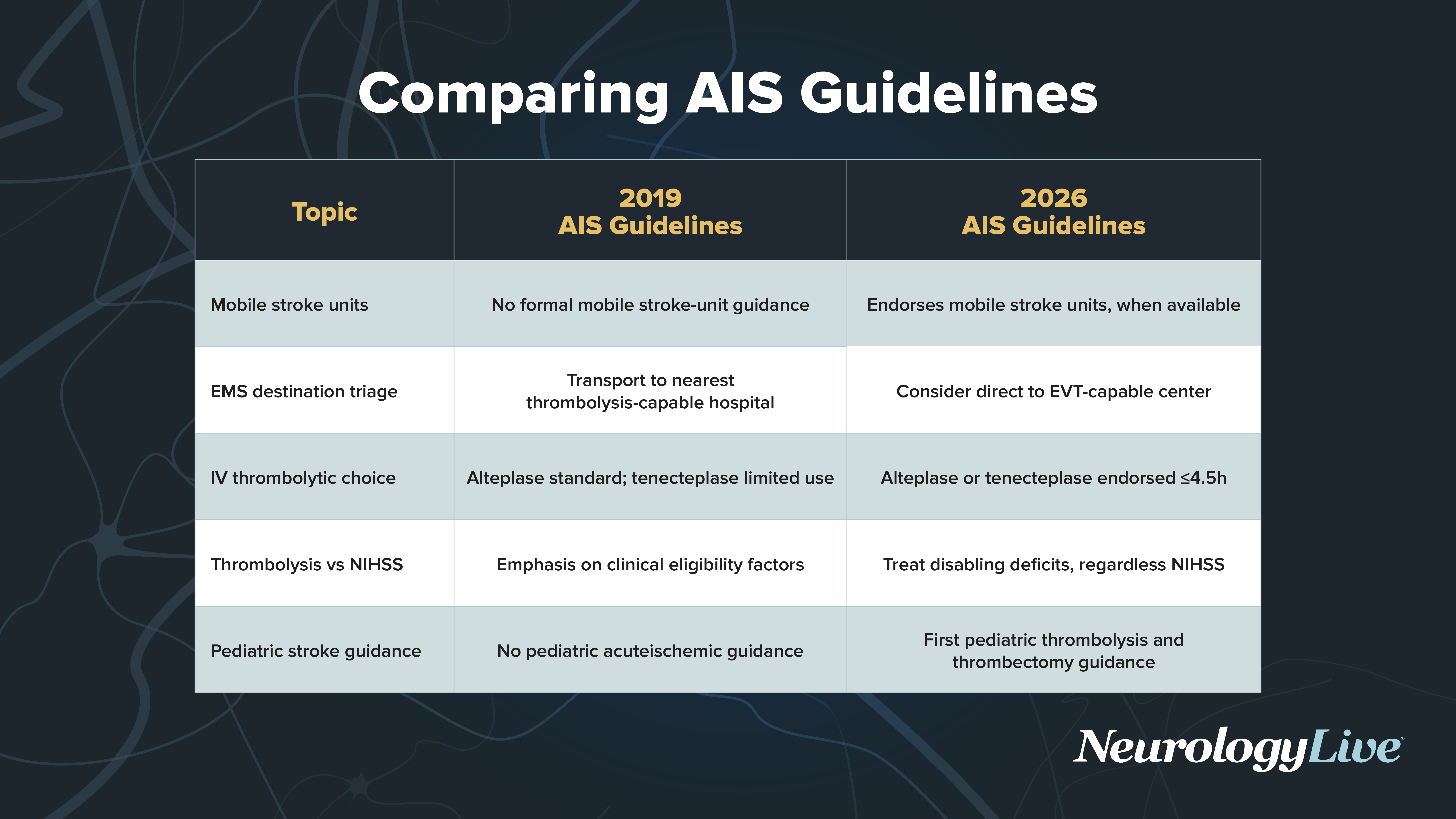
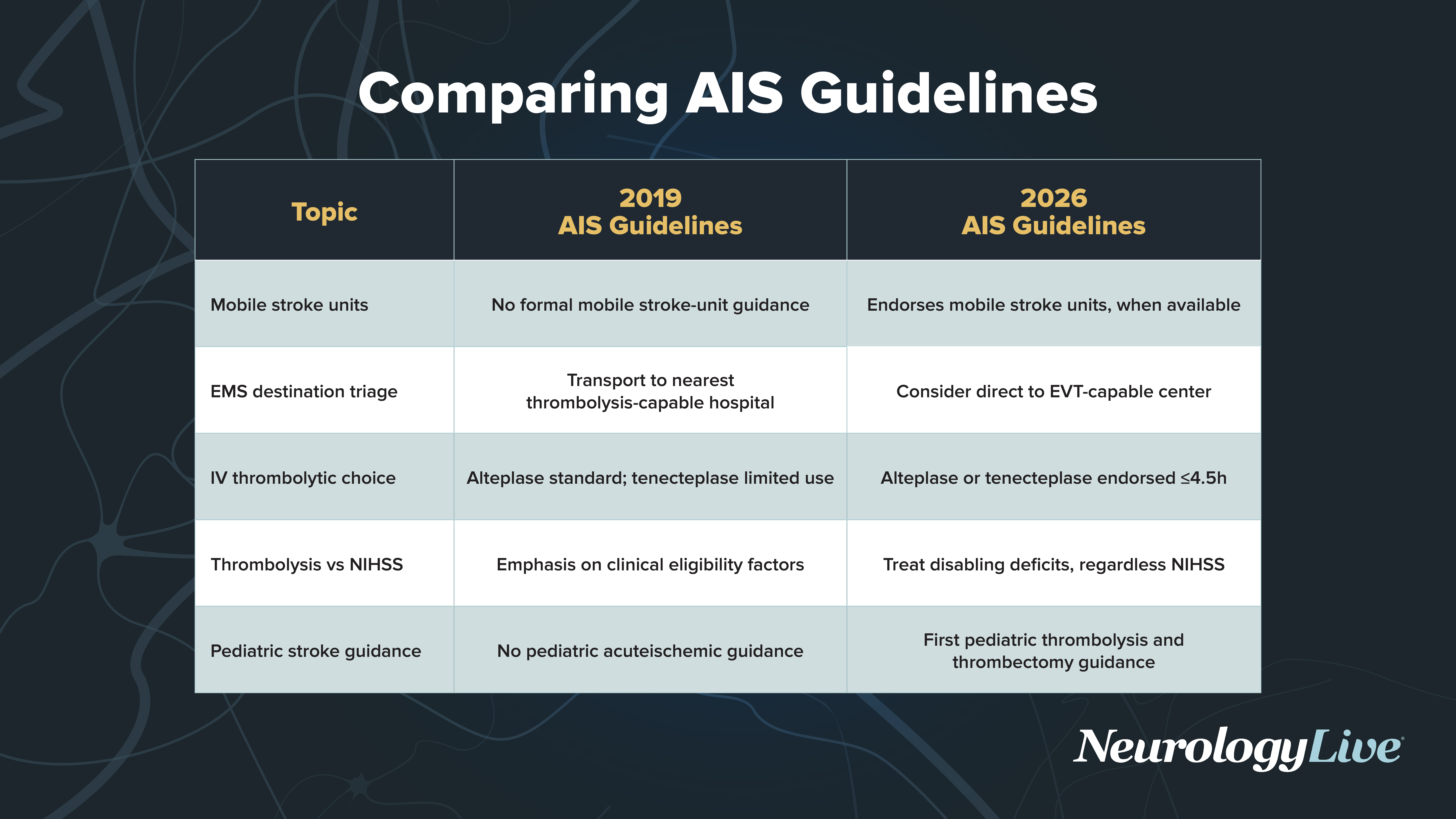
The updated stroke guidelines span the full continuum of acute ischemic stroke care, from prehospital triage and selection of intravenous thrombolytic agents to refined criteria for mechanical thrombectomy and post-procedural management. They clarify indications for tenecteplase and basilar artery thrombectomy, offer more cautious guidance for medium and distal vessel occlusions, and introduce structured recommendations for pediatric stroke and post-stroke dysphagia treatment. In addition to informing real-world clinical decision-making, the guidelines identify ongoing gaps in areas such as blood pressure management after reperfusion and device optimization, helping to shape future clinical trials and innovation in stroke systems of care.
As part of ongoing coverage, NeurologyLive® spoke with Andrei Alexandrov, MD, an award-winning leader in stroke research and clinical care, for an in-depth discussion of the updated guidelines. In this interview, Alexandrov shared key takeaways from the recommendations, examined their implications for everyday clinical practice, and highlighted remaining challenges in post-stroke blood pressure management. He also offered insight into how the revised criteria may shape future research priorities and therapeutic development in the field.
Top Takeaways From the 2026 Stoke Guidelines
Alexandrov explained that the updated 2026 stroke guidelines align formal recommendations with evolving real-world practice. Most notably, tenecteplase (TNK) is now recommended alongside alteplase as an acceptable agent for intravenous thrombolysis, reflecting widespread adoption at advanced stroke centers. The guidelines also formally endorse mobile stroke units for rapid thrombolysis delivery and triage where available, and, for the first time, incorporate structured recommendations for pediatric stroke, including imaging, registry development, and treatment considerations.
Major Takeaways
- Tenecteplase is now recommended alongside alteplase as an acceptable intravenous thrombolytic agent.
- Mobile stroke units are endorsed for rapid thrombolysis delivery and triage where available.
- Pediatric stroke is formally included, with guidance on imaging, registries, and treatment considerations.
- The guidelines are among the most comprehensive and detailed stroke updates published to date.
Unanswered Questions: Blood Pressure management and Reperfusion injury
Alexandrov noted that optimal blood pressure management after successful reperfusion remains unsettled. Although cerebral hyperperfusion is recognized after thrombectomy, trials of intensive blood pressure lowering have not improved outcomes and may cause harm. The field now faces the challenge of determining whether more individualized and standardized approaches are needed.
Major Takeaways
- Cerebral hyperperfusion occurs in a substantial subset of patients after successful reperfusion.
- Intensive blood pressure lowering has not consistently improved outcomes in trials.(Why should it? You're reducing the blood flow and oxygen delivery to the brain when it needs it most to prevent penumbra death! Can't you think at all?)
- Individualized blood pressure strategies may be preferable to one-size-fits-all approaches.
- More rigorous and standardized trials are needed to guide post-thrombectomy management.
Expanding the Scope of Stroke Care: Dysphagia and Rehabilitation
('care' NOT RECOVERY! For that alone, you're fired!)
Alexandrov spotlighted guidelines expansion beyond acute reperfusion, highlighting pharyngeal electrical stimulation (PES) as a recommended option for post-stroke dysphagia. With FDA approval supported by European data, this therapy represents a shift toward more active treatment of neurogenic dysphagia rather than relying solely on compensatory measures.
Major Takeaways
- Pharyngeal electrical stimulation is now recommended for selected patients with post-stroke dysphagia.
- FDA approval was supported by European data demonstrating safety and efficacy.
- The guidelines may accelerate adoption of more active dysphagia therapies in US practice.
- Stroke care continues to expand beyond acute reperfusion to include rehabilitation innovation.
Looking Ahead: A Tool for Practice Change and Future Research
Alexandrov concluded by mentioning that the 2026 update serves both as a consolidation of current evidence and a roadmap for future investigation. It equips clinicians to implement updated protocols while identifying research gaps in thrombectomy expansion, device development, and post-reperfusion management.
Major Takeaways
- The guidelines can help clinicians advocate for updated institutional protocols.
- Research gaps are clearly identified, guiding future clinical trials.
- Mechanical thrombectomy, thrombolysis, and rehabilitation strategies continue to evolve.
- The 2026 update represents both consolidation of progress and a roadmap for future innovation.
Transcript edited for clarity.
No comments:
Post a Comment