Having just had bronchitis and spells of coughing fits and sneezing. There is a major decision to make; do you bury you face in your good arm so as to not spread germs over a vast area? Or do you grab the affected arm to prevent elbowing your neighbor on the bus or plane? Both are not possible. Since your doctor and therapists COMPLETELY FUCKING FAILED AT CURING SPASTICITY! Ask them the proper response. The first time that occurred for me was at the kitchen table, buried the mouth in the arm, thus allowing the affected left arm to sweep my complete place setting to the floor, breaking most of it.
Thursday, April 30, 2026
Relationship between lower limb muscle coordination and knee flexion angle during the swing phase of gait in post-stroke individuals
THIS DOES NOTHING TO GET SURVIVORS RECOVERED! If you can't write EXACT protocols for guaranteed recovery, then get the hell out of stroke! Describing something does nothing for survivors! And you are too blitheringly stupid to see that; along with your mentors and seniors researchers! I'd have you all fired!
Relationship between lower limb muscle coordination and knee flexion angle during the swing phase of gait in post-stroke individuals
Abstract
Background
Stroke patients with hemiplegia often show inefficient gait patterns, including reduced knee flexion during the swing phase, which may increase fall risk. Post-stroke gait frequently involves merged muscle synergies that affect lower limb kinematics. However, it remains unclear how muscle synergy merging and fractionation relate to knee flexion during the swing phase. Therefore, this study aimed to examine the association between knee flexion during the swing phase and muscle synergy merging and fractionation patterns in patients with stroke.
Methods
The study comprised 21 stroke patients with hemiplegia. Surface electromyography was recorded from eight lower-limb muscles on the paretic side during comfortable gait. Maximum knee flexion angle (MKFA) during the swing phase was measured using a markerless motion capture system. Using non-negative matrix factorization, the number of muscle synergies, their spatiotemporal structure were calculated. Participants were classified into a low-synergy group (LS; n = 5; one or two synergies) or a high-synergy group (HS; n = 16; three synergies). Group comparisons of MKFA during the swing phase were performed. Furthermore, we investigated whether muscle synergies of the HS group could be fractionations of those of the LS group.
Results
The HS group showed significantly greater MKFA compared with the LS group (p = 0.032). In the HS group, the ankle plantar flexors constituted an independent muscle synergy, whereas in the LS group, these muscles had high weightings within a muscle synergy associated with load response. Furthermore, the independent muscle synergies observed in the HS group were shown to be fractionated from the merged muscle synergies present in the LS group.
Conclusion
Our results showed that merged muscle synergies were associated with reduced MKFA during the swing phase, whereas an independent synergy involving the plantar flexors was associated with greater knee flexion. These findings suggest that fractionation of the plantar flexor synergy may be important for improving knee kinematics after stroke and could inform targeted rehabilitation strategies. Given the relatively small and imbalanced sample size, cautious interpretation of the findings is warranted. Further studies with larger, balanced samples are needed to further strengthen the evidence for these findings.
Monday, April 27, 2026
Comparative efficacy of motor imagery augmented with central non-invasive brain stimulation versus peripheral electrical stimulation for upper extremity rehabilitation post-stroke: a systematic review and network meta-analysis
So, our fuckingly incompetent stroke medical 'professionals' STILL HAVEN'T WRITTEN ANY PROTOCOLS TO GET SURVIVORS RECOVERED! WOW! This was totally useless research then! Hope you blithering idiots like not recovering when you become the 1 in 4 per WHO that has a stroke!
And you've known of motor imagery for HOW LONG AND DONE NOTHING?
- motor imagery
(92 posts to January 2013)
Comparative efficacy of motor imagery augmented with central non-invasive brain stimulation versus peripheral electrical stimulation for upper extremity rehabilitation post-stroke: a systematic review and network meta-analysis
Abstract
Background
Upper limb dysfunction is a common and debilitating consequence of stroke, severely affecting patients’ activities of daily living and quality of life. Motor imagery (MI) has emerged as a promising rehabilitation technique, and its combination with various forms of non-invasive stimulation, both central (e.g., repetitive transcranial magnetic stimulation, rTMS; transcranial direct current stimulation, tDCS) and peripheral (e.g., functional electrical stimulation, FES), has been increasingly investigated. While previous meta-analyses have confirmed the general benefit of combined interventions, the relative efficacy of different MI-based combination strategies remains unclear. This systematic review and network meta-analysis aimed to directly and indirectly compare the effectiveness of MI augmented with different non-invasive central or peripheral stimulation modalities for upper extremity recovery post-stroke.
Methods
We registered the study on PROSPERO (CRD420251131264) and followed the PRISMA guidelines. Randomized controlled trials (RCTs) were searched in PubMed, Cochrane Library, EMBASE, Scopus, CNKI, and Wanfang databases from inception until August 4, 2025. The included RCTs involved adult stroke patients with upper limb dysfunction receiving MI combined with any non-invasive stimulation. The primary outcome was the change in upper limb motor function measured by the Fugl-Meyer Assessment (FMA or FMA-UE). A frequentist network meta-analysis was performed using random-effects models. Risk of bias was assessed using the Cochrane RoB 2 tool. Subgroup, sensitivity, and meta-regression analyses were conducted to explore heterogeneity.
Results
Seventeen RCTs involving 846 participants were included in the systematic review, with 13 studies forming the network for meta-analysis, comparing 9 intervention strategies. Network meta-analysis for the FMA outcome showed that MI combined with low-frequency rTMS (MI-LF-rTMS) showed a statistically significant difference compared to conventional rehabilitation alone (Standardized Mean Difference, SMD = 1.755, 95% CI 0.631 to 2.879, p = 0.002). No other intervention, including MI-tDCS, MI-FES, or any single therapy, showed a statistically significant difference compared to conventional rehabilitation. MI-LF-rTMS also showed a statistically significant difference in upper limb functional activity (Action Research Arm Test). Subgroup analyses indicated that the statistically significant difference for MI-LF-rTMS was also observed across intervention durations ≤ 4 weeks, disease stages ≤ 3 months post-stroke, and in protocols not using brain-computer interface technology. Meta-regression identified that the use of a brain-computer interface, publication year, and patient mean age were significant sources of heterogeneity.
Conclusion
Among the intervention strategies evaluated in this network meta-analysis, motor imagery combined with low-frequency repetitive transcranial magnetic stimulation (MI-LF-rTMS) showed a statistically significant difference compared to conventional rehabilitation. This regimen integrates central neuromodulation with cognitive training and may be a clinically feasible option, particularly for patients in the early phase after stroke. Future research should focus on parameter optimization, mechanistic exploration, and validation in larger, more diverse populations.
Friday, April 24, 2026
A just-released study finds that engaging in a brain game could lower your risk of dementia.
Ask your competent? doctor THE EXACT SPECIFIC GAME AND HOW LONG TO PLAY! Not knowing that is
COMPLETE FUCKING INCOMPETENCY! From your doctor, hospital and board of directors; all need to be fired!
A just-released study finds that engaging in a brain game could lower your risk of dementia
Study shows some people actually get stronger and sharper with age—here's what they all have in common
You'll just have to positively assume that this research on pessimism is COMPLETELY WRONG!
Your competent? doctor will then also confirm that this earlier research is totally wrong! Oh NO, your doctor doesn't know about it, does s/he?
My positive outlook is over the top; having fun the rest of my life! Currently in Rome, heading towards the Amalfi coast tomorrow.
Study shows some people actually get stronger and sharper with age—here's what they all have in common
Fact checked by Nick Blackmer
- A new study found that adults 65 and older can improve both their physical and cognitive function.
- People with a positive attitude toward aging were more likely to experience these health improvements.
- A rosier outlook on growing older makes you more likely to engage in habits that support health.
One of the most powerful influences on how well you age may be how you feel about it. A recent study that tracked thousands of older adults for over a decade suggests that physical and cognitive improvement is indeed possible with age—and one factor stood out in predicting who might boost functioning over time: mindset. Participants who held more positive views of aging were more likely to improve as they got older, researchers reported in the journal Geriatrics.
A Deeper Look at the Findings
Examples of people accomplishing remarkable feats later in life aren’t hard to find. The study points to Diana Nyad, who completed a 110-mile swim from Cuba to Florida at age 64, and Joseph Turner, who produced some of the most influential paintings later in his career.
The researchers wanted to know whether these kinds of stories are outliers—or part of a broader pattern, according to study author Martin Slade, MPH, PhD, a lecturer in occupational medicine at Yale School of Medicine. They also wondered whether attitude might help explain the difference.
To answer these questions, the team followed about 11,300 adults ages 65 and older from the Health and Retirement Study over 12 years. They assessed physical and cognitive health using measures like walking speed and cognitive tests, and asked participants about their beliefs around aging.
By the end of the study, 45.15% of participants showed improvement in cognitive function, physical function, or both. Notably, more positive beliefs around aging were associated with a higher likelihood of improvement. “There are two take-away messages from the study,” Slade said. “First, that the cognition and physical health of older people can improve and, in fact, a significant portion of older people do improve. Second, that positive age beliefs increase the likelihood that an older person’s cognition and physical health will improve over time.”
The findings come with some caveats, though. Slade noted that the researchers didn’t measure muscle and brain neuron plasticity, making it difficult to know exactly what caused the improvements. And the study didn’t examine which specific behaviors might have resulted from participants’ beliefs, which could help explain the link, pointed out Rosanne M. Leipzig, MD, PhD, a geriatrician and professor at the Icahn School of Medicine at Mount Sinai in New York.
Why Would a Positive Attitude Translate to Better Aging?
On a basic level, having a positive attitude means you’re more likely to try new things, experts said. “Aging beliefs are self-fulfilling prophecies,” Leipzig said. “What you do is related to what you expect.” In other words, if you don’t see age as a limitation, you’re probably more likely to sign up for a challenging dance class, make new friends, or travel—boosting your physical and mental fitness along the way. It’s that physical movement that’s key, noted Nir Barzilai, MD, a professor of genetics and medicine at Albert Einstein College of Medicine, director of the Institute for Aging Research, and co-founder and president of the Academy for Health and Lifespan Research. Having a positive attitude without positive habits may not make much of a difference, he added.
The same goes for a doom-and-gloom attitude about aging, which experts said often leads to fewer health-promoting activities. Leipzig has seen this pattern in his own patients. “In my practice, I have seen those with negative age beliefs withdraw, stop engaging, refuse to try adaptations like hearing aids or medical care that might help them have lives that are less isolated and more enjoyable,” he said.
Optimistic beliefs about aging may even change the brain’s structure, Slade added, increasing the rate at which neurons form new connections later in life. His previous research showed that negative aging beliefs can affect the brain, linking them to biomarkers associated with Alzheimer’s disease.
How to Have a Rosier Outlook on Aging
If you take anything away from this study, Barzilai said, it should be that the trajectory of aging is not set in stone. “There’s a flexibility [to it],” he added.
Having a positive outlook on your ability to get out into the world, challenge your brain, stay social, and move your body can influence how likely you are to keep doing these things—helping you adopt behaviors that may support a longer, healthier life, experts said.
So how do you flip a negative outlook into a more rosy one? What’s crucial, Leipzig said, is to try to view the last third of life as a time of possibility rather than inevitable decline. “It can be a time of continuing ability and even improvement for many people,” she noted. “Don’t sabotage yourself with your age beliefs.”
Barzilai, for his part, practices what he preaches. He recently moved with his wife from a suburban home to bustling Manhattan, where there’s more access to activity and culture. “I’m so busy, and Manhattan is so exciting,” he said.
Read the original article on Health
Objectively Measured Daytime Napping Patterns and All-Cause Mortality in Older Adults
It would seen to be better to address why the napping is occurring, NO sleep protocol so maybe not enough rest is achieved the night before. It would help if your doctor actually critically thinks about your napping. Maybe you need coffee napping.
- Coffee napping August 2014
Objectively Measured Daytime Napping Patterns and All-Cause Mortality in Older Adults
Key Points
Question Are objectively measured daytime nap characteristics, including duration, frequency, variability, and timing, associated with all-cause mortality among community-dwelling older adults? Findings In this prospective cohort study of 1338 adults aged 56 years or older, longer and more frequent daytime napping, as well as morning napping, were associated with higher all-cause mortality. Variability in nap duration was not associated with mortality.Meaning The findings suggest longer and more frequent, particularly morning, napping may be a behavioral marker of increased mortality risk in late life, underscoring the potential clinical value of incorporating wearable device–based nap assessments into routine health monitoring.
Abstract
Importance Daytime napping is common among older adults, but evidence linking objective daytime nap patterns to mortality is limited, as prior studies relied largely on self-report. Some daytime nap characteristics, such as timing and variability of nap duration across days, are also understudied.
Objective To test whether actigraphy-measured daytime nap duration, frequency, variability, and timing are associated with all-cause mortality.
Design, Setting, and Participants This prospective cohort study used data from the population-based Rush Memory and Aging Project, in which the analytic baseline was initiated in August 2005. Participants in this current study were community-dwelling adults aged 56 years or older in northern Illinois, with up to 19 years of follow-up. Data for this study were gathered until April 2025.
Main Outcome and Measures Daytime napping, defined as sleeping between 9 am and 7 pm and assessed by up to 14 days of actigraphy data. Cox proportional hazards regression models were used to estimate associations between baseline daytime nap characteristics (duration, frequency, variability in duration across days, and timing) and subsequent all-cause mortality.
Results Among 1338 participants over a mean (SD) follow-up of 8.30 (4.78) years (mean [SD] participant age, 81.40 [7.39] years; 1018 [76.0%] female), 926 (69.2%) died at a mean (SD) of 7.54 (4.52) years (range, 0.08-19.08 years) after analytic baseline. Participants wore the actigraphy device for a mean (SD) of 9.58 (1.22) days. After adjusting for all covariates, longer daytime nap duration (adjusted hazard ratio [AHR] per 1-hour increase, 1.13; 95% CI, 1.04-1.23; P = .005) and higher nap frequency (AHR per additional daily nap, 1.07; 95% CI, 1.02-1.13; P = .003) at baseline were associated with increased mortality. Morning nappers had higher mortality risk compared with early afternoon nappers (AHR, 1.30; 95% CI, 1.03-1.64; P = .03). Variability in daytime nap duration was not associated with mortality after covariate adjustment (AHR per 1-hour increase, 1.01; 95% CI, 0.89-1.14; P = .93).
Conclusions and Relevance In this prospective cohort study of community-dwelling older adults, longer and more frequent daytime napping, especially in the morning, were associated with higher all-cause mortality. The findings suggest incorporating wearable device–based daytime nap assessments into clinical and public health practices may provide novel opportunities for early risk identification of health conditions.
How the immune system may influence Alzheimer’s, Parkinson’s, and related diseases
Maybe this is why saunas are helpful in preventing dementia, boosting the immune system.
How the immune system may influence Alzheimer’s, Parkinson’s, and related diseases
A sweeping review shows how the brain’s immune defenses can both fight and fuel neurodegeneration, revealing why timing, cell type, and disease context may be crucial for future therapies.
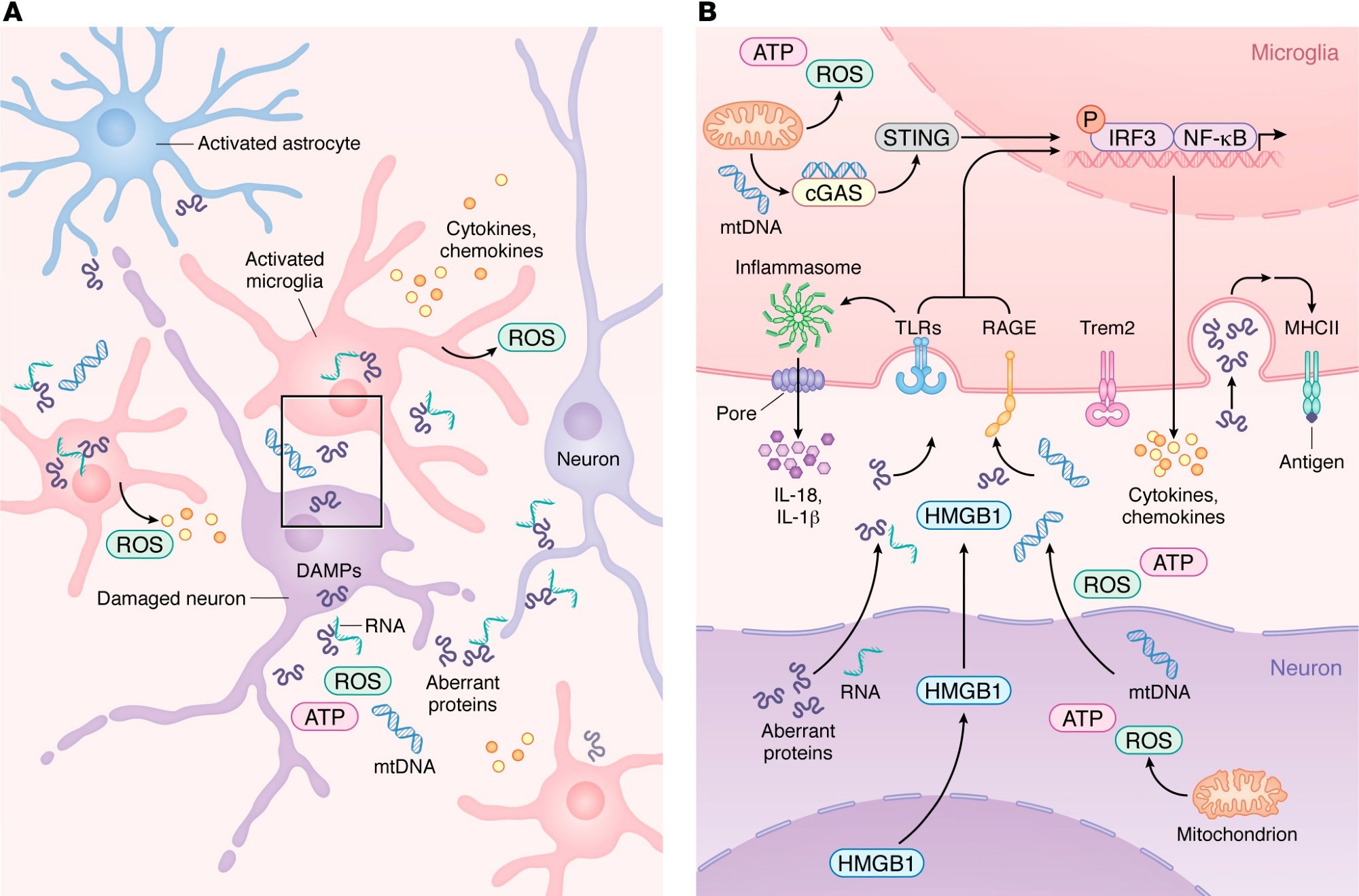
Innate immune activation and microglial transition during neurodegeneration. (A) During neurodegeneration, distressed neurons release DAMPs such as mtDNA, ROS, HMGB1, aberrant proteins, and pTau–bound RNA. These signals activate resident microglia and astrocytes, which then recruit peripheral immune cells. As shown in more detail in B, activated microglia upregulate PRRs, including TLRs, RAGE, and cGAS, enabling detection of neuron-derived DAMPs. Engagement of PRRs induces proinflammatory gene expression programs and activates inflammasome pathways that promote release of chemokines and cytokines into the CNS parenchyma. As microglia transition from homeostatic to reactive states in a TREM2-dependent manner, damage-associated microglia increase MHC-II expression to support antigen presentation and coordination of adaptive immune responses that attempt to limit neurodegeneration.
A recent review published in the Journal of Clinical Investigation synthesized current evidence on immune mechanisms in neurodegeneration. Accumulating evidence suggests that the immune system not only drives the progression of neurodegenerative diseases but also contributes to their onset through maladaptive cellular signaling and activation. The central nervous system (CNS) parenchyma depends on resident immune cells to maintain the blood-brain barrier (BBB) and respond to dysfunctional cells, pathogens, or cellular damage under steady-state conditions.
Neurons activate signaling pathways to respond to cellular dysfunction, while microglia and astrocytes alleviate danger signals and recruit peripheral immune cells. However, these responses can aggravate aberrant protein deposition during neurodegeneration, and the balance between detrimental and beneficial immune involvement is poorly defined. In the present review, researchers reviewed current knowledge of immune mechanisms in neurodegeneration.
Innate Immune Signaling in
Neurodegenerative Disease
Aberrant proteins, including phosphorylated tau, amyloid β (Aβ), and α-synuclein, have been identified as damage-associated molecular patterns (DAMPs) that activate pattern recognition receptors in the CNS. Toll-like receptor 2 (TLR2) and TLR4 are upregulated in mouse models of Alzheimer’s disease (AD) and in the brains of AD patients.
The binding of Aβ to TLR4 or TLR2 elevates the expression of cytokines, including tumor necrosis factor (TNF)-α, interleukin (IL)-6, IL-1β, IL-17, and IL-10, in microglia and astrocytes. Pharmacological inhibition or genetic ablation of these TLRs worsens cognitive decline and increases Aβ burden in the brain by decreasing microglial activation. The review also highlighted inflammasome and DNA-sensing pathways, including NLRP3 and cGAS-STING, as additional contributors to neuroinflammation across neurodegenerative diseases.
Studies have consistently reported increased expression of the receptor for advanced glycation end products (RAGE) on neurons, astrocytes, and microglia in AD, Parkinson’s disease (PD), and amyotrophic lateral sclerosis. RAGE overexpression in mouse AD models accelerated cognitive impairment, while its deficiency decreased memory deficits.
Genetic studies in AD patients identified two single-nucleotide polymorphisms (SNPs) in the triggering receptor expressed on myeloid cells 2 (TREM2), which is highly expressed by microglia, as risk factors of a magnitude comparable to carrying the apolipoprotein E (APOE) ε4 allele. These observations indicate that microglia are key players in neurodegenerative pathogenesis.
T Cell Responses Across
Neurodegenerative Disorders
A growing body of evidence indicates that cluster of differentiation 4 (CD4+) T cells have disease-specific functions across neurodegenerative diseases. Aβ-restricted CD4+ T cell transfusion into a transgenic AD mouse model was neuroprotective, preventing cognitive decline. In contrast, α-synuclein-specific CD4+ T cells were neurotoxic in PD models, promoting inflammation.

α-synuclein overexpression increased recruitment of CD4+ T cells producing interferon-γ, while depleting these cells decreased neuronal loss. These observations indicate that CD4+ T cells can be protective in some neurodegenerative diseases and pathogenic in others. In addition, CD8+ T cells have garnered increasing attention as contributors to CNS pathology. CD3+ and CD8+ T cells have been detected in the hippocampus in AD, with CD3+ T cell numbers correlating with tau pathology.
Similarly, increased CD8+ T cell numbers were observed in PD and correlated with neuronal death, although whether this relationship is causative or reactive remains uncertain. Further, the accumulation of neuroprotective CD8+ T cells in the brains of AD mice has been reported and shown to restrict amyloid plaque growth. Overall, studies reveal that CD8+ T cells have diverse roles in neurodegenerative diseases, shaped by antigen specificity, microglial interactions, and tissue residency. The review also noted growing interest in granzyme K-expressing CD8+ T cells as potentially specialized players in several neurodegenerative conditions.
Aging, Injury, and Viral Effects
on CNS Immunity
Aging is a major risk factor for neurodegenerative diseases. In youth, microglia survey the CNS, astrocytes maintain the BBB, and only a small number of T cells enter the parenchyma. However, in advanced ages, chronic low-grade inflammation occurs, during which many immune pathways become dysregulated.
Further, repetitive head injury can accelerate neurodegeneration. Traumatic brain injury is linked to the development of PD, AD, and chronic traumatic encephalopathy, even when it occurs in childhood. Following mild traumatic brain injury, the release of DAMPs by distressed cells triggers microglial activation, which clears debris and reinforces weakened BBB regions.
Repetitive injuries may increase reactivity and trigger microglial death, thereby allowing the entry of myelomonocytic cells. Like repetitive injuries, viral infections can alter CNS immunity and influence vulnerability to neurodegeneration. Recent studies have linked non-neurotropic and neurotropic viral infections to a higher risk of neurodegenerative diseases.
Immune Timing and
Neurodegeneration Implications
Taken together, neurodegenerative diseases stem from a complex interplay of environmental and biological factors that govern the magnitude and timing of immune activation and the programming of T cells, microglia, and other leukocytes. Viral infection, repetitive head injury, and aging restructure the CNS immune environment. Many immune pathways involved exhibit stage-dependent and context-specific functions.
Microglial activation may initially help clear aberrant proteins, but could become maladaptive with protracted stimulation. Similarly, CD8+ T cells can promote neuronal injury or support tissue repair based on antigen specificity, local signaling cues, and effector programming. As such, appreciating the cell-intrinsic states and temporal dynamics of immune cells is crucial for understanding immune signatures and determining when immunomodulatory interventions will be beneficial.
Journal reference:
- Latour YL, McGavern DB (2026). Immune signaling and function in neurodegeneration. Journal of Clinical Investigation, 136(8), e199850. DOI: 10.1172/JCI199850, https://www.jci.org/articles/view/199850
A single sauna session boosts immune cells within minutes
I'm getting a personal sauna from NuRecover but will use a cold shower instead of a chiller bucket for the cold shock proteins.
A single sauna session boosts immune cells within minutes
New research reveals how a brief Finnish sauna session mobilizes immune defenses within minutes, offering fresh clues into how heat exposure may influence human health.
 Study: Acute Finnish sauna heat exposure induces stronger immune cell than cytokine responses. Image credit: Mr. Tempter/Shutterstock.com
Study: Acute Finnish sauna heat exposure induces stronger immune cell than cytokine responses. Image credit: Mr. Tempter/Shutterstock.com
Heat exposure is harmful but can sometimes have beneficial effects. Finnish sauna bathing (FSB) is an example of controlled acute heat stress that may influence immune function by altering immune cells and cytokines. A 30-minute Finnish sauna session rapidly increases circulating immune cells while leaving most cytokine levels unchanged, according to a study published in the journal Temperature.
How Finnish sauna bathing
became a global health habit
FSB involves exposing people to relatively dry air at 70–100 °C for 10-30 minutes per session. It is part of Finnish culture and is shown to offer multiple health benefits. Existing literature reports lower risks of cardiovascular disease, dementia, psychosis, and some respiratory conditions. FSB is also associated with fewer adverse outcomes in disadvantaged socioeconomic settings and with better physical fitness.
Acute heat stress may reshape
immune and inflammatory responses
Prior research suggests that regular FSB is associated with lower levels of systemic inflammation. The current study examined how heat stress associated with FSB manifests as acute changes in white blood cells and cytokines up to 30 minutes after the sauna.
Single sauna session
triggers rapid immune cell mobilisation
Participants were free of known cardiovascular disease (CVD) but had one or more risk factors, such as smoking, hypertension, or obesity. The study included 51 middle-aged adults who were regular sauna users. During the 30-minute sauna session, body temperature, measured at the ear, increased steadily, reflecting the heat stress exposure, while plasma volume remained unchanged on average.
Among women, hemoglobin and hematocrit levels were lower, while platelet counts were higher than in men. In both sexes, all these factors increased with FSB. White cells also rose in women, and remained slightly higher at 30 minutes post-sauna.
Among white cells, neutrophils and lymphocytes returned to baseline at 30 minutes, unlike the persistent elevation seen with the combined MXD cell category (monocytes, eosinophils, and basophils). Overall, white cell proportions were preserved.
Only two cytokines changed significantly after FSB, and both decreased, while one additional marker showed a borderline increase. Immediately after FSB exposure, body temperature was correlated with circulating cytokine levels, though not with white cell counts. These included several interferons and interleukins, which were positively associated with raised ear temperature. Conversely, two cytokines were inversely correlated with ear temperature. These changes were independent of the frequency of sauna use across the week.
These findings suggest that white cells are mobilized in association with FSB exposure, but there was no direct correlation with increased temperature. Significant associations were observed for only a few cytokines, whereas a larger number showed correlations with temperature change in the immediate post-sauna period. The associations between temperature change and cytokines were largely unchanged after adjustment for sex or body mass index.
The authors propose that physiological challenge caused by FSB-induced heat stress may underlie these changes. The increase in hemoglobin concentration and hematocrit suggests a possible loss of plasma volume in the hot, dry FSB conditions, although average plasma volume did not change, and results were adjusted for individual variation.
The increase in neutrophil and lymphocyte counts could be due to immune cell mobilization in response to heat stress. The generalized nature of the response is suggested by the overall preservation of the differential count.
Apparently, a large temperature change is not required for such mobilization, as no correlation was found between temperature change and white cell count. Conversely, the former was associated with cytokine changes in the immediate post-sauna period, suggesting a heat-stress response.
The authors report that to the best of their knowledge, few prior studies have explored both immune cells and cytokines in relation to FSB-induced heat stress. The sauna use pattern in this study closely resembled that in real life and in some earlier research.
A few other studies have shown changes in some interleukins using different sauna protocols. This highlights the need for further research to distinguish sauna-induced responses in habitual sauna users (who are likely heat-adapted) from those in individuals who seldom or never use it.
Limited immune profiling
leaves key cell responses unclear
The authors measured three main white cell categories (neutrophils, lymphocytes, and the combined MXD group), but did not assess monocytes, eosinophils, and basophils separately. A more detailed lymphocyte assessment could have better assessed the heat-stress response to the FSB.
The physiological effects of cytokines correlated with temperature change following FSB remain unknown. The origin of the possibly mobilized white cells is unclear. The possibility of low plasma volume remains relevant, but was not factored into the analysis. Moreover, the study measured only the acute physiological response rather than chronic resting conditions.
Future directions should include research on the relevance of intermittent heat and cold stress exposure and whether these acute responses translate into long-term health effects.
Download your PDF copy by clicking here.
Journal reference:
Heinonen, I. H. A., Koivula, T., Hollmén, M., Immonen, J., Kunutsor, S. K., Jalkanen, S., & Laukkanen, J. A. (2026). Acute Finnish sauna heat exposure induces stronger immune cell than cytokine responses. Temperature. DOI: https://doi.org/10.1080/23328940.2026.2645467. https://www.tandfonline.com/doi/full/10.1080/23328940.2026.2645467#abstract
Multiple Pregnancies May Shield the Female Brain From Stroke
Strokes during pregnancy are a problem your competent? doctor needs to prevent!
- pregnancy
(14 posts to December 2011)
Multiple Pregnancies May Shield the Female Brain From Stroke
Summary: Conventional wisdom often jokes that having many children can “make you lose your mind,” but a new study suggests the opposite for brain health.
The research found that women who had three or more live births had a significantly lower risk of stroke and “covert” brain damage (vascular lesions). Given that women account for 57% of all strokes in the U.S., these findings offer a vital new tool for predicting and preventing neurological injury in females.
Key Findings
- The “Three-Birth” Threshold: After following 1,882 women over an 18-year period, researchers determined that three or more live births were consistently associated with a reduced risk of all-cause stroke.
- Reduced Vascular Injury: Women with three or more children also showed fewer signs of covert brain infarcts (brain lesions) and lower volumes of white matter hyperintensity.
- Unique Predictor: Interestingly, other factors like the use of hormone replacement therapy or specific estradiol levels did not show the same significant protective association in this cohort, making the number of live births a standout predictor.
- Statistical Rigor: The results remained significant even after researchers adjusted for major vascular risk factors like high blood pressure and cholesterol.
Source: UT San Antonio
While some say having lots of kids can make you lose your faculties, a new study suggests otherwise.
Research co-led by UT Health San Antonio, the academic health center of The University of Texas at San Antonio, associates a greater number of live births with a reduced risk of stroke or brain damage for mothers. As more women than men have strokes, the finding is seen as significant in helping determine risk.
The study, titled, “Number of Live Births as a Protective Factor Against Clinical and Covert Brain Infarcts: The Framingham Heart Study,” was published on April 7 in the Journal of the American Heart Association, and on behalf of the association.
“Our findings would suggest that reproductive factors – for example, number of live births – may be an additional factor to consider when assessing stroke risk in women,” said Sudha Seshadri, MD, a behavioral neurologist, professor and founding director of the Glenn Biggs Institute for Alzheimer’s and Neurodegenerative Diseases at UT Health San Antonio.
She is joint senior author of the study with Emer R. McGrath, PhD, with the School of Medicine at the University of Galway in Ireland. “Inclusion of this risk factor in female-specific clinical prediction rules for stroke may enhance risk prediction in women,” Seshadri said.
Reproductive factors in stroke
The study notes that stroke is a major cause of morbidity and death and disproportionately affects women, who account for 57% of all strokes in the United States.
Reproductive factors – for example, age at first menstrual period, age at menopause, circulating estrogen levels, number of pregnancies and use of hormone replacement therapy – affect overall lifetime exposure to estrogen, and therefore have been implicated as important predictors of future stroke risk in women.
Generally, greater exposure for a longer period or to higher levels of the body’s own estrogen has recently been associated with a lower burden of cerebral small-vessel disease in women. However, evidence for some factors, such as live births, has been conflicting.
For this study, researchers determined the association between number of live births and other female-specific reproductive factors and subsequent risk of stroke and magnetic resonance imaging markers of vascular brain injury in a community-based cohort. That cohort was the Framingham Heart Study, a long-term and ongoing community-based observational study of residents in Framingham, Massachusetts, dating to 1948. Seshadri serves as senior investigator.
Live births and decreased risk
The scientists followed 1,882 women over time, and who were stroke-free at a baseline examination during 1998 to 2001 and at a mean age of 61. They considered reproductive factors including the women’s number of live births given, age at menopause, postmenopausal hormone replacement therapy use, and serum estradiol and estrone levels.
During a median 18-year follow-up, they assessed the same participants for number of strokes from all causes, and secondarily for “covert brain infarcts” – like brain lesions representing vascular damage from restricted or reduced blood blow – and white matter hyperintensity volume, detected by MRI.
Over that period, 126 women had strokes. The researchers used statistical analyses known as multivariable Cox proportional hazards models adjusting for major vascular risk factors, and determined that three or more live births were associated with a reduced risk of stroke. Similarly, they found that three or more live births were associated with decreased risk of vascular brain injury.
“This may be an important factor to include in female-specific clinical prediction rules for stroke, but will require further study,” Seshadri said.
The researchers found no significant association between other reproductive factors and stroke or MRI markers of vascular brain injury.
Other authors of the study are with Boston University; Mass General Brigham, Boston; and University of California-Davis.
Key Questions Answered:
Q: Does this mean pregnancy is “medicine” for the brain?
A: It suggests that the biological state of pregnancy and the resulting hormonal shifts provide a protective effect on brain vasculature. However, it’s one factor among many; diet, exercise, and genetics still play massive roles in stroke prevention.
Q: If I had fewer than three children, am I at higher risk?
A: Not necessarily. The study found that three or more births provided a statistically significant reduction in risk, but it doesn’t mean women with fewer children are doomed to have strokes. It simply highlights a biological “bonus” for those who have had more births.
Q: Why does estrogen protect the brain?
A: Estrogen is known to be “neuroprotective.” It helps maintain the elasticity of blood vessels and reduces inflammation. Longer lifetime exposure to your body’s own estrogen seems to keep the brain’s “plumbing” in better shape for longer.
Editorial Notes:
- This article was edited by a Neuroscience News editor.
- Journal paper reviewed in full.
- Additional context added by our staff.
About this neurology research news
Author: Steven Lee
Source: UT San Antonio
Contact: Steven Lee – UT San Antonio
Image: The image is credited to Neuroscience News
Subscribe to:
Posts (Atom)