http://onlinelibrary.wiley.com/doi/10.1002/ana.22384/abstract
http://www.fabulousandfit.com/diets/study-says-cholesterol-doesnt-cause-stroke/
This second link is no longer functional which is where the following paragraphs came from.
There is a considerable amount of controversy surrounding the issue of saturated fat, cholesterol, and heart disease these days. Certainly, it seems that cholesterol on its own is a lousy predictor of heart disease.
And, just to add to this confusing mix, a new study published in the journal Annals of Neurology suggests that cholesterol has little or no causative role to play in the development of ischaemic stroke.
Conventional advice states that one of the risk factors for ischemic stroke (when blood supply to the brain is blocked by the build-up of fatty deposits in blood vessels), is high cholesterol levels.
14,000 men and women were followed for more than 30 years. Researchers looked at the relationship between cholesterol levels and risk of ischaemic stroke. They found no relationship at all in women, and no increased risk of stroke in men, unless cholesterol levels were raised 9.0 mmol/l (348 mg/dl), or more.
Triglycerides Levels and Stroke Risk
The researchers also examined the relationship between triglyceride levels and stroke risk, and they discovered that when triglyceride levels were higher the risk of stroke was higher, too.
So, it seems stroke is more closely associated with triglyceride than cholesterol, but whether higher levels actually cause stroke is unknown yet.
Interestingly, previous evidence has linked triglycerides with increased risk of heart disease and stroke. Researchers concluded that,
Lowering both lipids provides more benefit than reducing LDL-C alone. Source
So, how can you lower your triglyceride levels?
Maintain a healthy weight.
Be more active.
Avoid a high carbohydrate intake, especially simple sugars.
Limit your alcohol intake.
Quit smoking.
Government guidelines recommend a diet lower in fat and higher in carbohydrates, but if avoiding a high carbohydrate intake is beneficial for triglycerides levels, perhaps conventional nutrition advice needs a revamp — what do you think?
This one I know you would need to talk to your doctor on. I am currently taking a statin to reduce my cholesterol, wonder how long it is going to take to get a consensus on this new finding, I notice it didn't say anything about heart attacks.
Wednesday, March 9, 2011
TGF alpha and stroke rehab
Has your competent? doctor ensured human testing gets done? NO? So, you DON'T have a functioning stroke doctor, do you?
HAVE THEY BEEN FIRED YET?
TGF alpha and stroke rehab
I like the nasal spray. I wonder if this is just for acute rehab or could be used for chronic rehab?
New stroke therapy successful in rats
Date: 2010-01-12
Contact: Jennifer Fitzenberger
Phone: (949) 824-3969
Email: jfitzen@uci.edu
James Fallon
IRVINE — People with impaired mobility after a stroke soon may have a therapy that restores limb function long after the injury, if a supplemental protein works as well in humans as it does in paralyzed rats.
Two new studies by UC Irvine biologists have found that a protein naturally occurring in humans restores motor function in rats after a stroke. Administered directly to the brain, the protein restores 99 percent of lost movement; if it's given through the nose, 70 percent of lost movement is regained. Untreated rats improve by only 30 percent.
"No drugs exist that will help a stroke after a few days. If you have a stroke, you don't have many treatment options," said James Fallon, psychiatry & human behavior professor and senior co-author of the studies. "Now we have evidence there may be therapies that can repair damage to a significant degree long after the stroke. It's a completely unexpected and remarkable finding, and it's worth trying in humans."
The studies, carried out by UC Irvine postdoctoral researcher Magda Guerra-Crespo, chronicle the success of a small protein called transforming growth factor alpha, which plays critical tissue-forming and developmental roles in humans from just after conception through birth and into old age.
"TGF alpha has been studied for two decades in other organ systems but never before has been shown to reverse the symptoms of a stroke," Guerra-Crespo said. No lasting side effects were observed.
In the first study, published in the journal Neuroscience, scientists sought to learn whether TGF alpha administered directly to the brain could help rats with stroke-induced loss of limb function, typically on one side — as is seen in humans.
When put inside a cylinder, healthy rats will jump up with both front legs, but stroke-impaired rats will use just one leg, favoring the injured side. When given a choice of directions to walk, impaired rats will move toward their good side.
One month after the study rats suffered an induced stroke (equal to about a year for humans), some were injected with TGF alpha. Within a month, they had regained nearly all their motor function, hopping up with both legs in the cylinder exercise and not favoring a side in the directional test. Rats that did not receive treatment improved just 30 percent.
Scientists examined the rats' brains and found that TGF alpha was stimulating neuron growth. First, it prompted adult stem cells in the brain to divide, creating more cells. Those cells then turned into brain cells and moved to the injured part of the brain, replacing neurons lost to the stroke. These new neurons, the scientists believe, helped restore motor function.
"It's becoming more and more clear that the brain is like any other organ: It has a lot of potential to regenerate," said Darius Gleason, a developmental & cell biology graduate student who worked on the study. "We are just emulating nature by giving a little nudge to what the brain is trying to do itself."
In the second study, appearing online Jan. 11 in the Journal of Stroke & Cerebrovascular Diseases, scientists placed TGF alpha in the rats' noses, simulating a nasal spray. They used a slightly different chemical version of the protein to render it more stable on its journey to the brain. After a month, the injured rats had regained 70 percent of their function, indicating that the intranasal method also works well.
"We saw the same phenomena," Fallon said. "It wasn't as profound, but we still ended up with very significant behavioral improvements and the same regenerative anatomical process."
UC Irvine researchers Andres Sistos, Tina Toosky, Ihsan Solaroglu, John Zhang and Peter Bryant also worked on the intracranial study. Guerra-Crespo was supported by a UC MEXUS postdoctoral fellowship, Gleason was supported by a California Institute for Regenerative Medicine fellowship, and the research was funded by unrestricted gifts to Fallon.
Founded in 1965, the University of California, Irvine, is a top-ranked university dedicated to research, scholarship and community service. Led by Chancellor Michael Drake since 2005, UC Irvine is among the fastest-growing University of California campuses, with more than 27,000 undergraduate and graduate students, 1,100 faculty and 9,200 staff. The top employer in dynamic Orange County, UC Irvine contributes an annual economic impact of $4.2 billion. For more news, visit http://www.today.uci.edu/.
News Radio: UCI maintains on campus an ISDN line for conducting interviews with its faculty and experts. Use of this line is available for a fee to radio news programs/stations that wish to interview UCI faculty and experts. Use of the ISDN line is subject to availability and approval by the university.
UCI maintains an online directory of faculty available as experts to the media. To access, visit www.today.uci.edu/experts. For UCI breaking news, visit http://www.zotwire.uci.edu/.
A member of a stroke forum saw this and tried to mimic this on his own - It is not possible at this stage to try this at home so I decided to research which if any supplements were commercially available which contained this substance. I found two sources, namely, velvet deer antler and colostrum. This is a good question for your doctor to answer.
Monday, March 7, 2011
The Science of Stroke: Mechanisms in Search of Treatments Dr. Michael A. Moskowitz
When I first saw this referred to in ten steps forward in stroke research I knew I had to find it. I was unable to locate a free copy on the web so I contacted my local library and the librarian agreed to find me a copy from a partner library, but she ended up finding a free copy on the web here;
http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6WSS-515T9P7-K&_user=10&_coverDate=10%2F06%2F2010&_rdoc=17&_fmt=high&_orig=browse&_origin=browse&_zone=rslt_list_item&_srch=doc-info(%23toc%237054%232010%23999319998%232473768%23FLA%23display%23Volume)&_cdi=7054&_sort=d&_docanchor=&_ct=17&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=047db96ee281eb77b3593523a96758d8&searchtype=a
This is just the introduction, check out the URL if you want to read more;
Introduction
Selected section titles are here;
Calcium Dysregulation
Oxidative and Nitrosative Stress
Cortical Spreading Depolarizations
Inflammation
Necrosis, Necroptosis, and Autophagy: The Execution
What Causes the White Matter Damage Underlying VCI?
Why Does Stroke Increase the Risk of Dementia? This is worth reading although we need prevention
How Does the Brain Repair Itself after Stroke?
Repair and Remodeling Processes after Stroke
Someday I'll compare Dr. Moskowitz's theories with Dr. Clarkes Clarkes' stroke protocol
These two are the best I've seen and wonder why there aren't more references to them.We have to get away from the only acute stroke medication is tPA. Everyone of your doctors should know about this, my opinion only.
http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6WSS-515T9P7-K&_user=10&_coverDate=10%2F06%2F2010&_rdoc=17&_fmt=high&_orig=browse&_origin=browse&_zone=rslt_list_item&_srch=doc-info(%23toc%237054%232010%23999319998%232473768%23FLA%23display%23Volume)&_cdi=7054&_sort=d&_docanchor=&_ct=17&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=047db96ee281eb77b3593523a96758d8&searchtype=a
This is just the introduction, check out the URL if you want to read more;
Introduction
Few neurological conditions are as complex and devastating as
stroke, the second leading cause of death worldwide. Also
called a brain attack, victims may suddenly experience paralysis,
impaired speech, or loss of vision due to interruption of blood
flow (ischemia) caused by thrombosis or embolism. Less
frequently (<15%), strokes are caused by hemorrhage or cardiac
arrest. On average, strokes in the USA strike once every 40 s and
cause death every 4 min, with an estimated 41.6% death rate in
2007 (
absolute numbers are likely to rise. Among survivors, work
capacity is compromised in 70% of victims, and 30% need
assistance with self-care. Hence, the disease burden is great.
The estimated cost for stroke is 73.7 billion dollars in 2010
(USA) and projected to be 1.52 trillion dollars in 2050 (in 2005
dollars) (are spared, and the problem is global. For example, in the
Russian Federation and China, the estimated death rates per
100,000 population are five to ten times higher than in the USA
(mankind. For the above considerations and more, there is a compelling
need to accelerate efforts to interrogate the stroke process and
define the links that exist with other conditions such as vascular
and neurodegenerative dementia. It is also crucial to expand the
narrow repertoire of therapeutic opportunities for these devastating
conditions. To accomplish this, novel approaches are
required that expand upon our evolving mechanistic understanding
of the fundamentals of cell survival and death
processes as well as tissue repair. The future depends upon
how successful we are in deciphering these mechanisms and
bringing clarity to the complex interactions between the multiplicity
of cell and tissue types within brain (
with this knowledge and its successful therapeutic application,
the field of stroke could be transformed.
In this spirit then, this brief review addresses selected issues
fundamental to the science of ischemic stroke and vascular
dementia. It begins with posing questions about stroke risk
factors followed by a discussion of key cell and tissue mechanisms
that render brain susceptible as well as tolerant to
ischemic injury, including those promoting tissue protection
and repair. The review ends by highlighting promising treatment
strategies, inspired by these endogenous mechanisms, which
present the opportunity to open new avenues in stroke therapy.Selected section titles are here;
Parenchymal Failure: Why and How Does the Brain Die during Ischemia?
Salvageable versus Nonsalvageable Tissue: Salvageable Tissue Is the Target for Therapy
Salvageable versus Nonsalvageable Tissue: Salvageable Tissue Is the Target for Therapy
What Are the Prominent Mechanisms Leading to Cell and Tissue Demise?
ExcitotoxicityCalcium Dysregulation
Oxidative and Nitrosative Stress
Cortical Spreading Depolarizations
Inflammation
Necrosis, Necroptosis, and Autophagy: The Execution
What Causes the White Matter Damage Underlying VCI?
Why Does Stroke Increase the Risk of Dementia? This is worth reading although we need prevention
How Does the Brain Repair Itself after Stroke?
Repair and Remodeling Processes after Stroke
Moving Forward: Charting a Course toward New Stroke Therapies
Additional Strategies for Repair and Recovery: Trophic Factors and Cell-Based Therapies
Someday I'll compare Dr. Moskowitz's theories with Dr. Clarkes Clarkes' stroke protocol
These two are the best I've seen and wonder why there aren't more references to them.We have to get away from the only acute stroke medication is tPA. Everyone of your doctors should know about this, my opinion only.
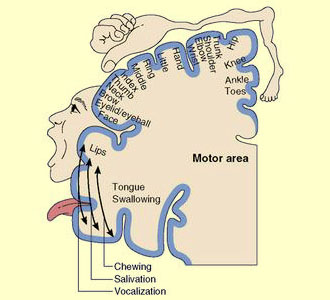
homunculus and stroke rehab
motor homunculus (Latin: little man).
After finally seeing my MRI and the damaged areas in my brain I started looking for a brain map to see what actually was destroyed and came across the motor and sensory homunculus maps.
Motor ones can be found here
http://www.brainconnection.com/med/medart/l/homunculus.jpg
or here
http://thebrain.mcgill.ca/flash/i/i_06/i_06_cr/i_06_cr_mou/i_06_cr_mou_1b.jpg
or here
http://www.vis.caltech.edu/~zoltan/szeged8/img8.htm
Sensory ones are here:
http://www.amareway.org/holisticliving/06/sensory-homunculus-cortical-homunculus-motor-homunculus/
According to the researcher who looked at my MRIs the infarct did not get into the sensory map. That may be true but my senses are still weaker than they should be so I think the connection out from the sensory map may have been damaged. By looking at the motor homunculus I can now see why I could wiggle my toes 2.5 years after my event. That area of the brain was spared and just needed to find a way thru or around all the dead space.I haven't quite figured out why my facial muscles still work, looking at my MRI it looks like that area is totally gone.
Nothing here is of immediate use to your rehab but if your doctors were writing up case studies they should be using these kinds of maps to explain what was damaged. And with these strokes could be compared to each other. What a novel idea! Standardized documentation and then we could easily start statistically mapping therapies to damage.
After finally seeing my MRI and the damaged areas in my brain I started looking for a brain map to see what actually was destroyed and came across the motor and sensory homunculus maps.
Motor ones can be found here
http://www.brainconnection.com/med/medart/l/homunculus.jpg
{kind=link}
or here
http://thebrain.mcgill.ca/flash/i/i_06/i_06_cr/i_06_cr_mou/i_06_cr_mou_1b.jpg
{kind=link}
or here
http://www.vis.caltech.edu/~zoltan/szeged8/img8.htm
Sensory ones are here:
http://www.amareway.org/holisticliving/06/sensory-homunculus-cortical-homunculus-motor-homunculus/
According to the researcher who looked at my MRIs the infarct did not get into the sensory map. That may be true but my senses are still weaker than they should be so I think the connection out from the sensory map may have been damaged. By looking at the motor homunculus I can now see why I could wiggle my toes 2.5 years after my event. That area of the brain was spared and just needed to find a way thru or around all the dead space.I haven't quite figured out why my facial muscles still work, looking at my MRI it looks like that area is totally gone.
Nothing here is of immediate use to your rehab but if your doctors were writing up case studies they should be using these kinds of maps to explain what was damaged. And with these strokes could be compared to each other. What a novel idea! Standardized documentation and then we could easily start statistically mapping therapies to damage.
magnesium and stroke rehab
This doesn't really tell you anything other than this is safe to administer and that further research needs to be done. Who is following up with additional research?
http://stroke.ahajournals.org/cgi/content/short/29/5/918
Dose Optimization of Intravenous Magnesium Sulfate After Acute Stroke
Keith W. Muir, MD, MRCP; ;Kennedy R. Lees, MD, FRCP
From the Acute Stroke Unit, University Department of Medicine and Therapeutics, Western Infirmary, Glasgow, Scotland.
Correspondence to Dr Keith W. Muir, Department of Neurology, Institute of Neurological Sciences, Southern General Hospital, Glasgow G51 4TF, Scotland. E-mail k.r.lees@clinmed.gla.ac.uk or k.muir@clinmed.gk.ac.uk
Background and Purpose—Parenterally administered MgSO4 is neuroprotective in standard animal models of focal cerebral ischemia and in many other paradigms of brain injury. Previous small clinical trials in stroke patients have explored the safety and tolerability of different infusion regimens. This study was undertaken to optimize the regimen for a multicenter trial.
Methods— Within 24 hours of the onset of clinically diagnosed stroke, patients were randomized to receive placebo or one of three intravenous MgSO4 infusions: a loading infusion of 8, 12, or 16 mmol, followed by 65 mmol over 24 hours. Cardiovascular parameters, serum magnesium concentrations, and blood glucose concentrations were determined. Outcome at 30 and 90 days was recorded.
Results—Twenty-five patients were recruited and treated at a mean time of 20 hours after stroke. No tolerability problems were identified. No effects of magnesium on heart rate, blood pressure, or blood glucose were evident. Serum magnesium concentrations rose to target levels most rapidly in the highest loading infusion group and were maintained in all groups for at least 24 hours.
Conclusions—MgSO4 infusions that rapidly elevate the serum magnesium concentration to potentially therapeutic levels are well tolerated and have no major hemodynamic effects in patients with acute stroke. The 16-mmol loading infusion achieved target serum concentrations most rapidly and has been chosen for further trials.
http://stroke.ahajournals.org/cgi/content/short/29/5/918
Dose Optimization of Intravenous Magnesium Sulfate After Acute Stroke
Keith W. Muir, MD, MRCP; ;Kennedy R. Lees, MD, FRCP
From the Acute Stroke Unit, University Department of Medicine and Therapeutics, Western Infirmary, Glasgow, Scotland.
Correspondence to Dr Keith W. Muir, Department of Neurology, Institute of Neurological Sciences, Southern General Hospital, Glasgow G51 4TF, Scotland. E-mail k.r.lees@clinmed.gla.ac.uk or k.muir@clinmed.gk.ac.uk
Background and Purpose—Parenterally administered MgSO4 is neuroprotective in standard animal models of focal cerebral ischemia and in many other paradigms of brain injury. Previous small clinical trials in stroke patients have explored the safety and tolerability of different infusion regimens. This study was undertaken to optimize the regimen for a multicenter trial.
Methods— Within 24 hours of the onset of clinically diagnosed stroke, patients were randomized to receive placebo or one of three intravenous MgSO4 infusions: a loading infusion of 8, 12, or 16 mmol, followed by 65 mmol over 24 hours. Cardiovascular parameters, serum magnesium concentrations, and blood glucose concentrations were determined. Outcome at 30 and 90 days was recorded.
Results—Twenty-five patients were recruited and treated at a mean time of 20 hours after stroke. No tolerability problems were identified. No effects of magnesium on heart rate, blood pressure, or blood glucose were evident. Serum magnesium concentrations rose to target levels most rapidly in the highest loading infusion group and were maintained in all groups for at least 24 hours.
Conclusions—MgSO4 infusions that rapidly elevate the serum magnesium concentration to potentially therapeutic levels are well tolerated and have no major hemodynamic effects in patients with acute stroke. The 16-mmol loading infusion achieved target serum concentrations most rapidly and has been chosen for further trials.
Sunday, March 6, 2011
finger intrinsics and stroke rehab
First some definitions. Intrinsic muscles are those completely contained within the hand/wrist unit. The extrinsic muscles are contained in the forearm and connected to the hand by tendons and provide
most of the power and range of motion of the joints of the hand.
Intrinsics stabilize the hand in fine motor tasks.
I have been working a lot on passively flexing and unflexing my fingers which are the extrinsic muscles, flexors and extensors but have not been working on the intrinsics mainly because I think I need to get the extrinsics working first.
On my 21 day canoe trip on the day I ripped the skin off my left palm we were paddling downstream with an upstream wind of 20-30 mph and I was paddling as best as I could on the right side with my left hand gripping the t-grip. My extension of my left arm was pretty poor, only able to get it out maybe 10-12 inches from my chest. We beat against the wind for maybe an hour until we were all forced ashore. After some consultations it was decided to set up camp, sleep and start paddling again in the evening when the wind usually dies down. So we slept from 5-10 pm and started again at midnight paddling until 3 am(24 hour daylight is wonderful at this latitude) I didn't sleep too well because the left hand was aching a lot. I think what occurred is that I totally overworked my finger flexors and the intrinsic muscles in the hand started firing to try to help hold the paddle. This was a wonderful occurence to find out about since it may lead me to a way to get the intrinsics firing again.
My other possibility is Theraband progressive hand trainer sheets. This is not clinically researched or tested so don't bother listening to my ramblings. Ask your therapist how to get intrinsics back and watch them blanch.
most of the power and range of motion of the joints of the hand.
Intrinsics stabilize the hand in fine motor tasks.
I have been working a lot on passively flexing and unflexing my fingers which are the extrinsic muscles, flexors and extensors but have not been working on the intrinsics mainly because I think I need to get the extrinsics working first.
On my 21 day canoe trip on the day I ripped the skin off my left palm we were paddling downstream with an upstream wind of 20-30 mph and I was paddling as best as I could on the right side with my left hand gripping the t-grip. My extension of my left arm was pretty poor, only able to get it out maybe 10-12 inches from my chest. We beat against the wind for maybe an hour until we were all forced ashore. After some consultations it was decided to set up camp, sleep and start paddling again in the evening when the wind usually dies down. So we slept from 5-10 pm and started again at midnight paddling until 3 am(24 hour daylight is wonderful at this latitude) I didn't sleep too well because the left hand was aching a lot. I think what occurred is that I totally overworked my finger flexors and the intrinsic muscles in the hand started firing to try to help hold the paddle. This was a wonderful occurence to find out about since it may lead me to a way to get the intrinsics firing again.
My other possibility is Theraband progressive hand trainer sheets. This is not clinically researched or tested so don't bother listening to my ramblings. Ask your therapist how to get intrinsics back and watch them blanch.
Transplants to restore memory for Alzheimer's sufferers after brain cells grown in lab
This mentions nothing about stroke but the general theory and work might be transferable if someone is willing to research the possibilities.
http://www.mirror.co.uk/news/top-stories/2011/03/05/transplants-to-restore-memory-for-alzheimer-s-sufferers-after-brain-cells-grown-in-lab-115875-22967051/
http://www.mirror.co.uk/news/top-stories/2011/03/05/transplants-to-restore-memory-for-alzheimer-s-sufferers-after-brain-cells-grown-in-lab-115875-22967051/
parasympathetic nervous system in the quest for stroke therapeutics
http://www.nature.com/jcbfm/journal/vaop/ncurrent/full/jcbfm201124a.html
I wish someone would correlate all these research findings and put together a comprehensive writeup of what should come next. I didn't get anything useful out of this and I'm not going to pay for the rest of the article. Isn't that what the medical profession is for?
I wish someone would correlate all these research findings and put together a comprehensive writeup of what should come next. I didn't get anything useful out of this and I'm not going to pay for the rest of the article. Isn't that what the medical profession is for?
Abstract
Stroke is a devastating neurovascular disease with limited therapeutic options. The pathogenesis of stroke involves complex interrelated molecular mechanisms including excitotoxicity, oxidative and nitrosative stress, cortical spreading depolarizations, inflammation, necrosis, and apoptosis. Successful development of stroke therapeutics depends on understanding these molecular mechanisms and how to counteract them to limit tissue damage during stroke. Activation of the parasympathetic nervous system (PNS) has been shown to antagonize a multiplicity of pathologic mechanisms. Elements of parasympathetic activation such as vagus nerve stimulation have already been used successfully in treating brain disorders such as epilepsy and depression. This review discusses the anatomical basis and molecular mechanisms involved in activation of the PNS, and assesses the strength of available evidence for the further development of this modality into a stroke therapy.
Friday, March 4, 2011
stem cell testing for stroke UK
http://www.drugs.com/clinical_trials/reneuron-gives-update-stroke-clinical-trial-11261.html
I know this is just safety testing but you have to start somewhere.
Guildford, UK, 3 March 2011: ReNeuron Group plc (LSE: RENE.L) today provides an update on progress with the PISCES clinical trial of its ReN001 stem cell therapy for disabled stroke patients. The PISCES study (Pilot Investigation of Stem Cells in Stroke) is the world’s first fully regulated clinical trial of a neural stem cell therapy for disabled stroke patients. Stroke is the third largest cause of death and the single largest cause of adult disability in the developed world.
The Company is pleased to report that the first two patients treated in the clinical trial are both well. Both patients were successfully treated with ReN001 with no acute safety issues arising. Both patients were discharged two days after their respective treatments and are back in their local communities in the Greater Glasgow area. The first patient treated has now been assessed at three months post-treatment and has experienced no adverse reactions or effects relating to the therapy.
The final patient in the first dose cohort has consented to treatment and, assuming a successful pre-treatment evaluation period, is expected to be dosed in May. On this basis, the Data Safety Monitoring Board would be expected to review data from the first dose cohort in August and, all being well, give approval for the trial to move on to a higher dose cohort at that time. The Company therefore expects that this higher dose cohort of three further patients would have been treated by the end of this year assuming no significant recruitment delays.
As the PISCES clinical trial continues into longer term follow-up of the patients treated, and into treatment of the higher dose cohorts, a number of treatment efficacy measures will be evaluated over time, including structural and functional MRI imaging measures as well as a number of tests of sensory, motor and cognitive functions. Although the primary endpoints of the clinical trial relate to the safety and tolerability of the ReN001 treatment, the Company hopes to use these potential efficacy measures in the design of subsequent clinical studies where efficacy of the treatment would be the primary endpoint.
The remaining dose cohorts in the PISCES trial are expected to be treated in 2012, at which point the Company intends to have discussed and agreed its subsequent clinical development strategy for ReN001 with the relevant regulatory authorities both in the UK and beyond. The Company is also exploring the clinical potential of its lead CTX stem cell line in other categories of the stroke patient population and in other neurological conditions where the mechanisms of action of the cells may be relevant. This is with a view to commencing further clinical trials in these indications as quickly as possible, based on the very significant pre-clinical safety and efficacy data already in existence with the CTX cells, as well as the emerging early clinical data from the PISCES trial. The Company will provide further updates on these activities, as well as progress with its other therapeutic programmes in peripheral arterial disease and retinitis pigmentosa, in due course.
The PISCES clinical trial is being conducted in Scotland at the Institute of Neurological Sciences, Southern General Hospital, Greater Glasgow and Clyde NHS Board. In this Phase I single administration dose escalation safety study, ReNeuron’s ReN001 stem cell therapy is being administered to a total of 12 stroke patients who have been left disabled by an ischaemic stroke, the most common form of the condition. The Principal Investigator for the trial is Professor Keith Muir, SINAPSE Professor of Clinical Imaging, Division of Clinical Neurosciences at the University of Glasgow. Patients in the clinical trial will be monitored for two years, with longer term follow-up procedures in place thereafter.
Michael Hunt, Chief Executive Officer of ReNeuron, said:
“Both ReNeuron and the clinical team in Glasgow are very encouraged by the progress of the PISCES clinical trial thus far. We are delighted that the two patients treated so far are doing as well as they are and we could not have hoped for a smoother start in terms of the clinical procedure itself and the lack of any apparent short term safety effects from the ReN001 therapy thereafter. We look forward to providing further updates on the clinical trial in due course.”
Enquiries:
Michael Hunt, Chief Executive Officer - ReNeuron +44 (0) 1483 302560 Dr John Sinden, Chief Scientific Officer - ReNeuron
Lisa Baderoon, Mark Court, Isabel Podda +44 (0) 20 7466 5000 Buchanan Communications
Antony Legge, Oliver Rigby +44 (0) 20 7776 6550 Daniel Stewart & Company plc
James Gallagher, Tim Graham +44 (0) 20 3206 7000 Matrix Corporate Capital LLP
Eleanor Cowie, Media Relations Officer +44 (0) 141 330 3683 University of Glasgow
About stroke
Approximately 150,000 people suffer a stroke in the UK each year. The vast majority of these strokes are ischaemic in nature, caused by a blockage of blood flow in the brain (as opposed to a haemorrhagic or bleeding stroke).
Approximately one half of all stroke survivors are left with permanent disabilities as a result of the damage caused to brain tissue arising from the stroke. The annual health and social costs of caring for these patients is estimated to be in excess of ? billion in the UK, with stroke patients estimated to be occupying at least 25 per cent of long term hospital beds.
The only current treatment for ischaemic stroke patients occurs in the acute phase of the condition (within several hours of the stroke), when anti-clotting agents are administered to dissolve the clot causing the blockage in blood flow to the brain. Only a small proportion of patients get to the hospital in time to be treated in this way.
Beyond the acute phase, there are no existing treatments, other than preventative or rehabilitation measures, to alleviate the disabilities suffered by stroke patients who have survived their stroke.
Source: UK Stroke Association
About ReNeuron’s ReN001 stem cell therapy for stroke
ReNeuron’s ReN001 cell therapy for stroke consists of a neural stem cell line, designated CTX, which has been generated using the Company’s proprietary cell expansion and cell selection technologies and then taken through a full manufacturing scale-up and quality-testing process. As such, ReN001 is a standardised, clinical and commercial-grade cell therapy product capable of treating all eligible patients presenting.
ReN001 has been shown to reverse the functional deficits associated with stroke disability when administered several weeks after the stroke event in relevant pre-clinical models of the condition. Extensive pre-clinical testing also indicates that the therapy is safe, with the ReN001 cells eventually cleared from the body with no adverse safety effects arising.
If ultimately shown to be safe and effective clinically, ReN001 would therefore offer a significant new treatment option for stroke survivors. The therapy offers the potential for a degree of recovery of function in disabled stroke patients, resulting in greater independence and quality of life for these patients and reduced reliance on health and social care systems.
The ReN001 cells that are being used in the initial clinical trial are taken from the existing manufactured cell banks that will form the basis of the eventual marketed product. There will therefore be no need to re-derive and test new ReN001 cell lines for subsequent clinical trials or for the market – all such cells can simply be expanded from the existing banked and tested product.
About the Institute of Neurological Sciences at Glasgow University
The clinical Stroke Research Group of the Division of Clinical Neurosciences is based at the Institute of Neurological Sciences at Glasgow University, and has major collaborations, internally with the Glasgow Experimental MRI Centre, with SINAPSE (Scottish Imaging Network: A Platform for Scientific Excellence), and with the Translational Medicine Research Initiative (TMRI). Around 900 patients per year are admitted through the Acute Stroke Unit, which provides stroke services to the population of south Glasgow and specialist stroke treatments for the West of Scotland.
The unit is the highest user of acute clot-busting (thrombolytic) treatment in the UK at present, and has been extensively involved in clinical trials in stroke. Major research interests include evaluation of advanced brain imaging techniques in acute stroke, development of novel brain imaging techniques, improving the use of clot-busting drug treatments in stroke, and developing trial methodology for evaluation of regenerative treatments. The group has support from the Stroke Association, the Medical Research Council, and the TMRI. Further work with regenerative strategies include collaborations with groups developing both drug-based and stem cell therapies across Europe. About ReNeuron ReNeuron is a leading, clinical-stage stem cell business. Its primary objective is the development of novel stem cell therapies targeting areas of significant unmet or poorly met medical need.
ReNeuron has used its unique stem cell technologies to develop cell-based therapies for significant disease conditions where the cells can be readily administered “off-the-shelf” to any eligible patient without the need for additional immunosuppressive drug treatments. ReNeuron’s lead candidate is its ReN001 stem cell therapy for the treatment of patients left disabled by the effects of a stroke. This therapy is currently in early clinical development. ReNeuron’s ReN009 stem cell therapy is being developed as a treatment for peripheral arterial disease, a serious and common side-effect of diabetes. The Company is also developing stem cell therapies for other conditions such as blindness-causing diseases of the retina.
ReNeuron has also developed a range of stem cell lines for non-therapeutic applications – its ReNcell® products for use in academic and commercial research. The Company’s ReNcell®CX and ReNcell®VM neural cell lines are marketed worldwide under license by USA-based Millipore Corporation.
ReNeuron’s shares are traded on the London AIM market under the symbol RENE.L. Further information on ReNeuron and its products can be found at http://www.reneuron.com/.
This announcement contains forward-looking statements with respect to the financial condition, results of operations and business achievements/performance of ReNeuron and certain of the plans and objectives of management of ReNeuron with respect thereto. These statements may generally, but not always, be identified by the use of words such as "should", "expects", "estimates", "believes" or similar expressions. This announcement also contains forward-looking statements attributed to certain third parties relating to their estimates regarding the growth of markets and demand for products. By their nature, forward-looking statements involve risk and uncertainty because they reflect ReNeuron's current expectations and assumptions as to future events and circumstances that may not prove accurate. A number of factors could cause ReNeuron's actual financial condition, results of operations and business achievements/performance to differ materially from the estimates made or implied in such forward-looking statements and, accordingly, reliance should not be placed on such statements.
I know this is just safety testing but you have to start somewhere.
Guildford, UK, 3 March 2011: ReNeuron Group plc (LSE: RENE.L) today provides an update on progress with the PISCES clinical trial of its ReN001 stem cell therapy for disabled stroke patients. The PISCES study (Pilot Investigation of Stem Cells in Stroke) is the world’s first fully regulated clinical trial of a neural stem cell therapy for disabled stroke patients. Stroke is the third largest cause of death and the single largest cause of adult disability in the developed world.
The Company is pleased to report that the first two patients treated in the clinical trial are both well. Both patients were successfully treated with ReN001 with no acute safety issues arising. Both patients were discharged two days after their respective treatments and are back in their local communities in the Greater Glasgow area. The first patient treated has now been assessed at three months post-treatment and has experienced no adverse reactions or effects relating to the therapy.
The final patient in the first dose cohort has consented to treatment and, assuming a successful pre-treatment evaluation period, is expected to be dosed in May. On this basis, the Data Safety Monitoring Board would be expected to review data from the first dose cohort in August and, all being well, give approval for the trial to move on to a higher dose cohort at that time. The Company therefore expects that this higher dose cohort of three further patients would have been treated by the end of this year assuming no significant recruitment delays.
As the PISCES clinical trial continues into longer term follow-up of the patients treated, and into treatment of the higher dose cohorts, a number of treatment efficacy measures will be evaluated over time, including structural and functional MRI imaging measures as well as a number of tests of sensory, motor and cognitive functions. Although the primary endpoints of the clinical trial relate to the safety and tolerability of the ReN001 treatment, the Company hopes to use these potential efficacy measures in the design of subsequent clinical studies where efficacy of the treatment would be the primary endpoint.
The remaining dose cohorts in the PISCES trial are expected to be treated in 2012, at which point the Company intends to have discussed and agreed its subsequent clinical development strategy for ReN001 with the relevant regulatory authorities both in the UK and beyond. The Company is also exploring the clinical potential of its lead CTX stem cell line in other categories of the stroke patient population and in other neurological conditions where the mechanisms of action of the cells may be relevant. This is with a view to commencing further clinical trials in these indications as quickly as possible, based on the very significant pre-clinical safety and efficacy data already in existence with the CTX cells, as well as the emerging early clinical data from the PISCES trial. The Company will provide further updates on these activities, as well as progress with its other therapeutic programmes in peripheral arterial disease and retinitis pigmentosa, in due course.
The PISCES clinical trial is being conducted in Scotland at the Institute of Neurological Sciences, Southern General Hospital, Greater Glasgow and Clyde NHS Board. In this Phase I single administration dose escalation safety study, ReNeuron’s ReN001 stem cell therapy is being administered to a total of 12 stroke patients who have been left disabled by an ischaemic stroke, the most common form of the condition. The Principal Investigator for the trial is Professor Keith Muir, SINAPSE Professor of Clinical Imaging, Division of Clinical Neurosciences at the University of Glasgow. Patients in the clinical trial will be monitored for two years, with longer term follow-up procedures in place thereafter.
Michael Hunt, Chief Executive Officer of ReNeuron, said:
“Both ReNeuron and the clinical team in Glasgow are very encouraged by the progress of the PISCES clinical trial thus far. We are delighted that the two patients treated so far are doing as well as they are and we could not have hoped for a smoother start in terms of the clinical procedure itself and the lack of any apparent short term safety effects from the ReN001 therapy thereafter. We look forward to providing further updates on the clinical trial in due course.”
Enquiries:
Michael Hunt, Chief Executive Officer - ReNeuron +44 (0) 1483 302560 Dr John Sinden, Chief Scientific Officer - ReNeuron
Lisa Baderoon, Mark Court, Isabel Podda +44 (0) 20 7466 5000 Buchanan Communications
Antony Legge, Oliver Rigby +44 (0) 20 7776 6550 Daniel Stewart & Company plc
James Gallagher, Tim Graham +44 (0) 20 3206 7000 Matrix Corporate Capital LLP
Eleanor Cowie, Media Relations Officer +44 (0) 141 330 3683 University of Glasgow
About stroke
Approximately 150,000 people suffer a stroke in the UK each year. The vast majority of these strokes are ischaemic in nature, caused by a blockage of blood flow in the brain (as opposed to a haemorrhagic or bleeding stroke).
Approximately one half of all stroke survivors are left with permanent disabilities as a result of the damage caused to brain tissue arising from the stroke. The annual health and social costs of caring for these patients is estimated to be in excess of ? billion in the UK, with stroke patients estimated to be occupying at least 25 per cent of long term hospital beds.
The only current treatment for ischaemic stroke patients occurs in the acute phase of the condition (within several hours of the stroke), when anti-clotting agents are administered to dissolve the clot causing the blockage in blood flow to the brain. Only a small proportion of patients get to the hospital in time to be treated in this way.
Beyond the acute phase, there are no existing treatments, other than preventative or rehabilitation measures, to alleviate the disabilities suffered by stroke patients who have survived their stroke.
Source: UK Stroke Association
About ReNeuron’s ReN001 stem cell therapy for stroke
ReNeuron’s ReN001 cell therapy for stroke consists of a neural stem cell line, designated CTX, which has been generated using the Company’s proprietary cell expansion and cell selection technologies and then taken through a full manufacturing scale-up and quality-testing process. As such, ReN001 is a standardised, clinical and commercial-grade cell therapy product capable of treating all eligible patients presenting.
ReN001 has been shown to reverse the functional deficits associated with stroke disability when administered several weeks after the stroke event in relevant pre-clinical models of the condition. Extensive pre-clinical testing also indicates that the therapy is safe, with the ReN001 cells eventually cleared from the body with no adverse safety effects arising.
If ultimately shown to be safe and effective clinically, ReN001 would therefore offer a significant new treatment option for stroke survivors. The therapy offers the potential for a degree of recovery of function in disabled stroke patients, resulting in greater independence and quality of life for these patients and reduced reliance on health and social care systems.
The ReN001 cells that are being used in the initial clinical trial are taken from the existing manufactured cell banks that will form the basis of the eventual marketed product. There will therefore be no need to re-derive and test new ReN001 cell lines for subsequent clinical trials or for the market – all such cells can simply be expanded from the existing banked and tested product.
About the Institute of Neurological Sciences at Glasgow University
The clinical Stroke Research Group of the Division of Clinical Neurosciences is based at the Institute of Neurological Sciences at Glasgow University, and has major collaborations, internally with the Glasgow Experimental MRI Centre, with SINAPSE (Scottish Imaging Network: A Platform for Scientific Excellence), and with the Translational Medicine Research Initiative (TMRI). Around 900 patients per year are admitted through the Acute Stroke Unit, which provides stroke services to the population of south Glasgow and specialist stroke treatments for the West of Scotland.
The unit is the highest user of acute clot-busting (thrombolytic) treatment in the UK at present, and has been extensively involved in clinical trials in stroke. Major research interests include evaluation of advanced brain imaging techniques in acute stroke, development of novel brain imaging techniques, improving the use of clot-busting drug treatments in stroke, and developing trial methodology for evaluation of regenerative treatments. The group has support from the Stroke Association, the Medical Research Council, and the TMRI. Further work with regenerative strategies include collaborations with groups developing both drug-based and stem cell therapies across Europe. About ReNeuron ReNeuron is a leading, clinical-stage stem cell business. Its primary objective is the development of novel stem cell therapies targeting areas of significant unmet or poorly met medical need.
ReNeuron has used its unique stem cell technologies to develop cell-based therapies for significant disease conditions where the cells can be readily administered “off-the-shelf” to any eligible patient without the need for additional immunosuppressive drug treatments. ReNeuron’s lead candidate is its ReN001 stem cell therapy for the treatment of patients left disabled by the effects of a stroke. This therapy is currently in early clinical development. ReNeuron’s ReN009 stem cell therapy is being developed as a treatment for peripheral arterial disease, a serious and common side-effect of diabetes. The Company is also developing stem cell therapies for other conditions such as blindness-causing diseases of the retina.
ReNeuron has also developed a range of stem cell lines for non-therapeutic applications – its ReNcell® products for use in academic and commercial research. The Company’s ReNcell®CX and ReNcell®VM neural cell lines are marketed worldwide under license by USA-based Millipore Corporation.
ReNeuron’s shares are traded on the London AIM market under the symbol RENE.L. Further information on ReNeuron and its products can be found at http://www.reneuron.com/.
This announcement contains forward-looking statements with respect to the financial condition, results of operations and business achievements/performance of ReNeuron and certain of the plans and objectives of management of ReNeuron with respect thereto. These statements may generally, but not always, be identified by the use of words such as "should", "expects", "estimates", "believes" or similar expressions. This announcement also contains forward-looking statements attributed to certain third parties relating to their estimates regarding the growth of markets and demand for products. By their nature, forward-looking statements involve risk and uncertainty because they reflect ReNeuron's current expectations and assumptions as to future events and circumstances that may not prove accurate. A number of factors could cause ReNeuron's actual financial condition, results of operations and business achievements/performance to differ materially from the estimates made or implied in such forward-looking statements and, accordingly, reliance should not be placed on such statements.
canadian best practices for stroke care
http://www.strokebestpractices.ca/index.php/overview/
What Canada lists as best practices. It probably won't help any of us chronic survivors but at least you'll know more than your medical staff.
What Canada lists as best practices. It probably won't help any of us chronic survivors but at least you'll know more than your medical staff.
New Zealand stroke research
http://www.nzherald.co.nz/health/news/article.cfm?c_id=204&objectid=10685204
http://tvnz.co.nz/health-news/high-hopes-stroke-research-breakthrough-3877861
http://www.nzdoctor.co.nz/un-doctored/2010/november-2010/04/otago-research-uncovers-potential-for-stroke-victims-to-dramatically-regain-mobility-.aspx
None of the links I tried specified what drug was being tested. I will be going to the library to see if the Nature article mentions it. I like the possible 3 week window.
University of Otago and American researchers have discovered a drug therapy which could dramatically help stroke victims by unlocking paralysed arms and legs and restoring much of their lost mobility.
Results of the 2 year study were published today in the online edition of the international scientific journal Nature.
"This also provides hope for those with traumatic head injuries - the brain mechanisms of repair are similar so there is potential for this to work for them too," study co-author Dr Andrew Clarkson said.
Dr Clarkson, 31, a research fellow at the Otago University departments of psychology and anatomy and structural biology, said human trials using the drug compounds could begin within two years.
One compound, known to enhance cognition and initially developed to treat Alzheimer's disease, is already being tested in people with learning difficulties.
In the first study of its kind, Dr Clarkson and colleagues at the University of California, including neurologist co-author Dr Thomas Carmichael, found the compound, given to mice in slow-release doses, re-activated brain neurons responsible for limb function.
Dr Clarkson said the finding was "tremendous" and could be "the biggest therapeutic breakthrough in many years".
The treatment worked on gross motor skills, but it would take further research to clarify whether the drug could also help with the fine motor skills associated with speech.
The research suggests some brain cells affected by strokes or other head injuries have not been killed, as often previously thought, but are effectively "sleeping" and can be reactivated.
Ok, a couple of lines from the article:
This increased tonic inhibition is mediated by extrasynaptic GABAA receptors and is caused by an impairment in GABA (γ-aminobutyric acid) transporter (GAT-3/GAT-4) function. To counteract the heightened inhibition, we administered in vivo a benzodiazepine inverse agonist specific for α5-subunit-containing extrasynaptic GABAA receptors at a delay after stroke. This treatment produced an early and sustained recovery of motor function.
What!!
http://tvnz.co.nz/health-news/high-hopes-stroke-research-breakthrough-3877861
http://www.nzdoctor.co.nz/un-doctored/2010/november-2010/04/otago-research-uncovers-potential-for-stroke-victims-to-dramatically-regain-mobility-.aspx
None of the links I tried specified what drug was being tested. I will be going to the library to see if the Nature article mentions it. I like the possible 3 week window.
University of Otago and American researchers have discovered a drug therapy which could dramatically help stroke victims by unlocking paralysed arms and legs and restoring much of their lost mobility.
Results of the 2 year study were published today in the online edition of the international scientific journal Nature.
"This also provides hope for those with traumatic head injuries - the brain mechanisms of repair are similar so there is potential for this to work for them too," study co-author Dr Andrew Clarkson said.
Dr Clarkson, 31, a research fellow at the Otago University departments of psychology and anatomy and structural biology, said human trials using the drug compounds could begin within two years.
One compound, known to enhance cognition and initially developed to treat Alzheimer's disease, is already being tested in people with learning difficulties.
In the first study of its kind, Dr Clarkson and colleagues at the University of California, including neurologist co-author Dr Thomas Carmichael, found the compound, given to mice in slow-release doses, re-activated brain neurons responsible for limb function.
These neurons had initially appeared to be dead or dormant after a stroke.
Six weeks of treatment produced dramatic results, with an extra 50 per cent of gross motor limb mobility consistently gained. Treatment of the mice began three days after the stroke - the equivalent of about three weeks in humans.Dr Clarkson said the finding was "tremendous" and could be "the biggest therapeutic breakthrough in many years".
The treatment worked on gross motor skills, but it would take further research to clarify whether the drug could also help with the fine motor skills associated with speech.
The research suggests some brain cells affected by strokes or other head injuries have not been killed, as often previously thought, but are effectively "sleeping" and can be reactivated.
Ok, a couple of lines from the article:
This increased tonic inhibition is mediated by extrasynaptic GABAA receptors and is caused by an impairment in GABA (γ-aminobutyric acid) transporter (GAT-3/GAT-4) function. To counteract the heightened inhibition, we administered in vivo a benzodiazepine inverse agonist specific for α5-subunit-containing extrasynaptic GABAA receptors at a delay after stroke. This treatment produced an early and sustained recovery of motor function.
What!!
Thursday, March 3, 2011
Lobster shells may offer paralysis cure, study finds
This one is taking a leap to possibly transfer this into acute stroke rehab, but if someone doesn't think outside the bun we'll never get anywhere.
http://www.themedguru.com/20100419/newsfeature/lobsters-may-offer-paralysis-cure-study-finds-86134225.html
http://www.themedguru.com/20100419/newsfeature/lobsters-may-offer-paralysis-cure-study-finds-86134225.html
In what could lead to a new discovery of nerve cell regeneration for people paralyzed by spinal cord injuries, researchers claim the shells of sea creatures may repair damaged nerve membranes and restore the spinal cord's ability to transmit signals to the brain.
After spinal cord injuries, many people become paralyzed because their brains are cut off from central pattern generators, which are networks of neurons in the spinal cord that are thought to produce an automatic walking motion.
Richard Borgens and his team comprising of physiologist Riyi Shi and chemist Youngnam Cho from the Center for Paralysis Research at the Purdue School of Veterinary Medicine have discovered that the simple sugar found in the crustacean shells of lobsters is capable of targeting damaged membranes.
Professor Richard Borgens stated, “This is the most exciting development for spinal cord and brain injury since Second World War.
“I am very excited. Using chemicals to repair the damaged nervous system is a completely new way to treat people with these terrible injuries. It’s amazing one of these special chemicals would turn out to be a sugar.”
Experiment on guinea pigs
Researchers started experimenting on guinea pigs. They first isolated and compressed a segment of the rodent’s spinal cord. Subsequently, they applied the chemical and a fluorescent dye that could only enter the cells through damaged membranes.
Scrutinizing the tissues under the microscope, the investigators noted that all the neurons in the spinal cord tissue remained unstained by the dye. Moreover, while measuring the guinea pigs’ brain response, they observed that the signals failed to reach the brain because of the damaged spinal cord.
Thirty minutes after injecting the sugar mixed with sterile water into the bloodstream of the animals the researchers found that the damaged cells had been repaired.
The experts stated, “However, 30•min after injecting chitosan into the rodents, the signals miraculously returned to the animals’ brains.”
Researchers theorize that the injected sugar migrates to the spinal cord injury where it plugs holes in the coating of the nerve cells.
Borgens added, “Science has moved in a new direction. Previously we have been looking at drugs which would potentially reduce damage. Now we are looking at complete repair.”
Implications of the study
The researchers are optimistic that the treatment, which showed promise in guinea pigs, will also work equally well in human trials.
Borgens stated, “The spinal cord of a guinea pig is very similar to that of a human – it is just smaller.
“This is not like a drug which may work in some species and not in others. This is a mechanical effect. The sugar molecules migrate to the nerve injury target and repair the injured area, not the undamaged area.”
The discovery has been published in The Journal of Experimental Biology.
Richard Borgens and his team comprising of physiologist Riyi Shi and chemist Youngnam Cho from the Center for Paralysis Research at the Purdue School of Veterinary Medicine have discovered that the simple sugar found in the crustacean shells of lobsters is capable of targeting damaged membranes.
Professor Richard Borgens stated, “This is the most exciting development for spinal cord and brain injury since Second World War.
“I am very excited. Using chemicals to repair the damaged nervous system is a completely new way to treat people with these terrible injuries. It’s amazing one of these special chemicals would turn out to be a sugar.”
Experiment on guinea pigs
Researchers started experimenting on guinea pigs. They first isolated and compressed a segment of the rodent’s spinal cord. Subsequently, they applied the chemical and a fluorescent dye that could only enter the cells through damaged membranes.
Scrutinizing the tissues under the microscope, the investigators noted that all the neurons in the spinal cord tissue remained unstained by the dye. Moreover, while measuring the guinea pigs’ brain response, they observed that the signals failed to reach the brain because of the damaged spinal cord.
Thirty minutes after injecting the sugar mixed with sterile water into the bloodstream of the animals the researchers found that the damaged cells had been repaired.
The experts stated, “However, 30•min after injecting chitosan into the rodents, the signals miraculously returned to the animals’ brains.”
Researchers theorize that the injected sugar migrates to the spinal cord injury where it plugs holes in the coating of the nerve cells.
Borgens added, “Science has moved in a new direction. Previously we have been looking at drugs which would potentially reduce damage. Now we are looking at complete repair.”
Implications of the study
The researchers are optimistic that the treatment, which showed promise in guinea pigs, will also work equally well in human trials.
Borgens stated, “The spinal cord of a guinea pig is very similar to that of a human – it is just smaller.
“This is not like a drug which may work in some species and not in others. This is a mechanical effect. The sugar molecules migrate to the nerve injury target and repair the injured area, not the undamaged area.”
The discovery has been published in The Journal of Experimental Biology.
A Nasal Spray against Alzheimer's Disease and Stroke
This one is pretty unknown yet, especially since it hasn't been tried in humans yet and doesn't yet seem to have a good understanding of why it works.
A Nasal Spray against Alzheimer's Disease and Stroke
Researchers have claimed to develop a nasal spray against Alzheimer's disease and stroke. The spray is expected to repair the vascular damage in the brain by provoking the body's immune system.
Researchers of the Tel Aviv University have claimed to develop this spray. Dr. Dan Frenkel, of the Tel Aviv University's Department of Neurobiology, says that they have done the clinical trials of the medication which have shown that it prevents brain tissue damage and restore cognitive impairment.
Dr. Frenkel believes that this new medication is a milestone which may help in developing vaccination and long-sought cure for Alzheimer's disease. He added that this spray might open new pathways for the treatments related to the immune system and could also reduce the cases of stroke and Alzheimer's disease. It may also prevent the progression of disease.
Researchers have conducted the tests of the spray on mice but it has not been tested on humans yet. The test conducted on mice has shown that vascular damage was prevented after the injection of vaccination and no side effects have been reported.
Dr. Frenkel told that this drug has already been tested safely by GlaxoSmithKline as an influenza treatment but it is unknown that when it will be available.
Ok, what are the active ingredients in the spray?
xenon gas and stroke rehab
I know this was not directly tested in stroke rehab but it sounds like something fascinating to followup on.
xenon gas and stroke rehab
Scientists have successfully conducted the first clinical trial giving xenon gas to patients undergoing coronary artery bypass grafting in order to safeguard against postoperative brain damage that can occur following this procedure.
Research published in Anesthesiology shows how the team safely gave xenon to 12 patients undergoing coronary artery bypass grafting while on cardiopulmonary artery bypass, a step which could eventually lead to new treatments for people suffering from illnesses that damage nerve cells, such as strokes, and brain and spinal cord injuries.
Earlier preclinical work by the team showed that xenon was effective as a neuroprotectant, stopping processes present during strokes or brain and spinal cord injuries that would damage nerve cells. They found that xenon was capable of blocking the effects of a particular type of glutamate receptor, the same receptor implicated in the pathway that leads to nerve cell death.
The discovery that xenon acted as a neuroprotectant came about when Professor Nick Franks ![]() , a biophysicist from Imperial College London was investigating possible molecular targets which could be responsible for the action of different anaesthetics.
, a biophysicist from Imperial College London was investigating possible molecular targets which could be responsible for the action of different anaesthetics.
Professor Mervyn Maze ![]() , an anaesthetist from Imperial College London who has collaborated with Professor Franks in the xenon research programme, said: "We knew from our earlier studies that xenon was effective in stopping damaged nerve cells from dying, but this study is of tremendous importance as it shows that it is feasible to administer xenon safely to a population of patients at risk for developing brain damage. What we need now is a clinical trial to test the efficacy of xenon in large numbers of patients.
, an anaesthetist from Imperial College London who has collaborated with Professor Franks in the xenon research programme, said: "We knew from our earlier studies that xenon was effective in stopping damaged nerve cells from dying, but this study is of tremendous importance as it shows that it is feasible to administer xenon safely to a population of patients at risk for developing brain damage. What we need now is a clinical trial to test the efficacy of xenon in large numbers of patients.
"Xenon could provide a whole new way of treating nerve damaging illnesses. Although we can stop people dying from these illnesses, there is not much we can do to stop the nerve damage that ultimately leads to devastating long-term disability."
Professor Franks added: "We hope xenon could be developed as a novel treatment. It is naturally occurring, and more importantly, its known lack of toxicity makes it an attractive candidate as a neuroprotectant in humans.
"Ultimately, we hope xenon could become part of standard medical treatment, with paramedics being able to administer it to stroke and brain-injured victims to stop ongoing nerve cell death."
And this makes me wonder if my earlier post on bubbles and ultrasound had come to an incorrect conclusion that the vibrating bubbles were the reason for the benefit rather than the xenon gas they used in the bubbles.
http://oc1dean.blogspot.com/2011/03/bubbles-with-ultrasound-stroke-drugs.html
Something for researchers to followup on.
I wonder if xenon gas causes the same voice response as helium?
Post-Stroke Spasticity Ask the Experts
I know this is subversive but what the hell. The National Stroke Association is having a webinar for stroke professionals. And since I am now a professional in stroke rehabilitation I qualify.
http://www.stroke.org/site/MessageViewer?em_id=9701.0&JServSessionIdr004=a7n04orm63.app202b
You can register here. It doesn't ask for a membership number and you can submit questions ahead of time.
The question box has a limited number of spaces so be succint with your questions. Mine were on how to get from stage to stage in Brunnstroms' stages of recovery, and what protocol is to be followed to cure it. I put down survivor as my professional title.
Lets crash the party, there seems to be no other way to get the attention of the NSA. In fact I think I'll register several times with different email addresses so I can ask more questions.
Ignore the email us link to advocacy@stroke.org It didn't work two months ago.
It would be great if we could get more survivors there than medical staff, I'm sure we'd have better questions.
http://www.stroke.org/site/MessageViewer?em_id=9701.0&JServSessionIdr004=a7n04orm63.app202b
You can register here. It doesn't ask for a membership number and you can submit questions ahead of time.
The question box has a limited number of spaces so be succint with your questions. Mine were on how to get from stage to stage in Brunnstroms' stages of recovery, and what protocol is to be followed to cure it. I put down survivor as my professional title.
Lets crash the party, there seems to be no other way to get the attention of the NSA. In fact I think I'll register several times with different email addresses so I can ask more questions.
Ignore the email us link to advocacy@stroke.org It didn't work two months ago.
It would be great if we could get more survivors there than medical staff, I'm sure we'd have better questions.
Wednesday, March 2, 2011
bubbles with ultrasound - stroke drugs directly into the brain
So I wonder which would be better, nanoparticles or bubbles? Or is it the xenon gas?
bubbles with ultrasound - stroke drugs directly into the brain
Now, stroke drugs directly into the brain (Thinkstock photos/Getty Images)
Scientists believe that bubbles could deliver a devastating blow to disease.
Injected into the blood, tiny bubbles of gas can ease the passage of vital stroke drugs into the brain, helping prevent damage to the grey matter.
Now, a group of researchers calling themselves ''the bubble community'' are studying how they could help fight disease.
They have shown that blasting bubbles with ultrasound makes them move back and forth, and, bizarrely, makes it easier for nearby cells to take up medicines.
"The theory is that the bubbles are stimulating the natural uptake mechanisms," the Daily Mail quoted Eleanor Stride, of University College London, as saying.
"Exactly which mechanisms, we're not sure."
Bubbles can even open up the blood-brain barrier, the protective blockade that regularly stops drugs from getting into the brain from the bloodstream.
Stride told New Scientist : "If you expose the blood-brain barrier to bubbles and ultrasound, you can temporarily and reversibly enhance its permeability, which is potentially interesting for a lot of brain treatments."
Examples include the treatment of stroke, in which an interruption of the blood supply to the brain causes cells to become damaged or die.
Researchers from the University of Cinncinnati in Ohio filled microbubbles with xenon - a gas known to protect brain cells from dying an improve blood flow, but difficult to administer.
Rats treated with the xenon-filled bubbles had smaller areas of brain damage than untreated animals.
In another piece of research, bubbles filled with a drug used to break down clots, were used to treat people who had strokes.
The technique eased the passage of the drug to the brain, speeding up the restoration of the blood flow to the brain.
But not without a cost - two of the patients given the highest dosage of the ''bubble drug'' in combination with ultrasound started haemorrhaging and died.
Gene variant affects stroke prognosis in humans
Interesting that this comes from Armenia
http://www.health.am/ab/more/gene-variant-affects-stroke-prognosis-in-humans/
A small difference in DNA sequence predicts the degree of disability after a stroke, according to a paper published online on February 28 in the Journal of Experimental Medicine. Stroke, the consequence of disturbed blood flow to the brain, can impair speech, movement and vision, but it is currently difficult for clinicians to predict the severity of these side effects or the long-term prognosis.
Strokes result in the death of brain cells called neurons. Angeles Almeida and co-workers found that variations in a gene known to control cell death - Tp53 - influence stroke outcome.
Tp53 comes in two flavors in humans: R and P. The R variant triggers cell death more efficiently. In two distinct groups of stroke patients, those exclusively expressing the R variant suffered more severe disability several months after the stroke. Neurons expressing the R variant were more vulnerable to death caused by oxygen deprivation, a condition that mimics the brain environment during stroke.
Future work is needed to determine if this Tp53 variation can also predict prognosis of patients with other disorders characterized by neuronal death, such as Alzheimer’s or Parkinson’s disease.
About The Journal of Experimental Medicine
The Journal of Experimental Medicine (JEM) is published by The Rockefeller University Press. All editorial decisions on manuscripts submitted are made by active scientists in conjunction with our in-house scientific editors. JEM content is posted to PubMed Central, where it is available to the public for free six months after publication. Authors retain copyright of their published works and third parties may reuse the content for non-commercial purposes under a creative commons license. For more information, please visit www. jem.org.
Gomez-Sanchez, J.C., et al. 2011. J. Exp. Med. doi:10.1084/jem.20101523
So who is following up on these gene variants to see how to stop the cell death from occuring? I can't quite see this becoming common unless there is an easy way to find that gene variant.
http://www.health.am/ab/more/gene-variant-affects-stroke-prognosis-in-humans/
A small difference in DNA sequence predicts the degree of disability after a stroke, according to a paper published online on February 28 in the Journal of Experimental Medicine. Stroke, the consequence of disturbed blood flow to the brain, can impair speech, movement and vision, but it is currently difficult for clinicians to predict the severity of these side effects or the long-term prognosis.
Strokes result in the death of brain cells called neurons. Angeles Almeida and co-workers found that variations in a gene known to control cell death - Tp53 - influence stroke outcome.
Tp53 comes in two flavors in humans: R and P. The R variant triggers cell death more efficiently. In two distinct groups of stroke patients, those exclusively expressing the R variant suffered more severe disability several months after the stroke. Neurons expressing the R variant were more vulnerable to death caused by oxygen deprivation, a condition that mimics the brain environment during stroke.
Future work is needed to determine if this Tp53 variation can also predict prognosis of patients with other disorders characterized by neuronal death, such as Alzheimer’s or Parkinson’s disease.
About The Journal of Experimental Medicine
The Journal of Experimental Medicine (JEM) is published by The Rockefeller University Press. All editorial decisions on manuscripts submitted are made by active scientists in conjunction with our in-house scientific editors. JEM content is posted to PubMed Central, where it is available to the public for free six months after publication. Authors retain copyright of their published works and third parties may reuse the content for non-commercial purposes under a creative commons license. For more information, please visit www. jem.org.
Gomez-Sanchez, J.C., et al. 2011. J. Exp. Med. doi:10.1084/jem.20101523
So who is following up on these gene variants to see how to stop the cell death from occuring? I can't quite see this becoming common unless there is an easy way to find that gene variant.
Tuesday, March 1, 2011
Boost potassium intake to cut stroke by 20 percent
http://www.theheart.org/article/1190147.do
Naples, Italy - The largest meta-analysis so far conducted examining the impact of potassium intake on cardiovascular outcomes has found that higher dietary consumption of this mineral is associated with lower rates of stroke and could also reduce the risk of coronary heart disease (CHD) and total CVD [1].
The results apply to all sectors of society and not just to specific "at-risk" subgroups, say Dr Lanfranc D'Elia (University of Naples Medical School, Italy) and colleagues in the study, published in the March 8, 2011 issue of the Journal of the American College of Cardiology. "Potassium intake may be increased by well-described dietary changes, mainly an increase in fruit and vegetable consumption, as recommended by all guidelines to prevent vascular diseases," they state.
Most doctors are not aware of what huge benefits one might derive from this measure. The researchers are not the first to urge people to eat more potassium-containing foods, and recent updated USDA dietary guidelines recommend increasing intake of foods rich in potassium. Senior author of this new research, Dr Pasquale Strazzullo (University of Naples Medical School, Italy), told heartwire that it is important to convey this to clinicians: "Most doctors are not aware of what huge benefits one might derive from this measure," he observes.
But doctors must also be careful not to confuse patients with too much detail on different nutrients, he says. Simple advice to eat more fruits and vegetables, in particular those that are very rich in potassium—including bananas, tomatoes, oranges, apricots, and most legumes—is probably best, he says. "The most practical advice we can give is that people should have five or six servings of fruit and vegetables a day," he says.
Potassium intake far lower than recommended in all participants
The researchers identified 11 studies on the association between habitual dietary potassium intake and incidence of vascular events over the past 30 years, including 247 510 participants with follow-up of five to 19 years, for their meta-analysis. There were 7066 strokes, 3058 CHD events, and 2497 total CVD events. Potassium intake was assessed by 24-hour dietary recall in two studies, by food frequency questionnaire (FFQ) in six, and by 24-hour urinary excretion in three.
In the pooled analysis, a 1.64-g (42 mmol)/day higher potassium intake—which Strazzullo says is equivalent to around three pieces of fruit high in potassium—was associated with a 21% lower risk of stroke (risk ratio 0.79; p=0.0007), with a trend toward lower risk of CHD and total CVD that attained statistical significance after the exclusion of a single cohort (RR 0.93; p=0.03 and RR 0.74; p=0.0037).
In all of the populations studied in the present meta-analysis, potassium intake was far lower than the recommended intake of 100 mmol or more per day, they note.
The Italian doctors say the protective effect of potassium against stroke is in part due to its BP-lowering effects, particularly in hypertensive individuals and in those with elevated sodium intake, but also likely due to other properties of the mineral, such as the inhibition of free radical formation, as demonstrated in experimental studies.
Increasing potassium=reducing salt: Prevent one million strokes/year
They add that the magnitude of risk reduction with increasing potassium intake by 1.64 g per day is similar to that which would result from lowering dietary sodium consumption by 5 g (85 mmol) per day and would translate "into a reduction of 1 155 000 stroke deaths per year on a worldwide scale."
Not sure what I'll do about this except add this to my questions to my cardiologist.
Naples, Italy - The largest meta-analysis so far conducted examining the impact of potassium intake on cardiovascular outcomes has found that higher dietary consumption of this mineral is associated with lower rates of stroke and could also reduce the risk of coronary heart disease (CHD) and total CVD [1].
The results apply to all sectors of society and not just to specific "at-risk" subgroups, say Dr Lanfranc D'Elia (University of Naples Medical School, Italy) and colleagues in the study, published in the March 8, 2011 issue of the Journal of the American College of Cardiology. "Potassium intake may be increased by well-described dietary changes, mainly an increase in fruit and vegetable consumption, as recommended by all guidelines to prevent vascular diseases," they state.
Most doctors are not aware of what huge benefits one might derive from this measure. The researchers are not the first to urge people to eat more potassium-containing foods, and recent updated USDA dietary guidelines recommend increasing intake of foods rich in potassium. Senior author of this new research, Dr Pasquale Strazzullo (University of Naples Medical School, Italy), told heartwire that it is important to convey this to clinicians: "Most doctors are not aware of what huge benefits one might derive from this measure," he observes.
But doctors must also be careful not to confuse patients with too much detail on different nutrients, he says. Simple advice to eat more fruits and vegetables, in particular those that are very rich in potassium—including bananas, tomatoes, oranges, apricots, and most legumes—is probably best, he says. "The most practical advice we can give is that people should have five or six servings of fruit and vegetables a day," he says.
Potassium intake far lower than recommended in all participants
The researchers identified 11 studies on the association between habitual dietary potassium intake and incidence of vascular events over the past 30 years, including 247 510 participants with follow-up of five to 19 years, for their meta-analysis. There were 7066 strokes, 3058 CHD events, and 2497 total CVD events. Potassium intake was assessed by 24-hour dietary recall in two studies, by food frequency questionnaire (FFQ) in six, and by 24-hour urinary excretion in three.
In the pooled analysis, a 1.64-g (42 mmol)/day higher potassium intake—which Strazzullo says is equivalent to around three pieces of fruit high in potassium—was associated with a 21% lower risk of stroke (risk ratio 0.79; p=0.0007), with a trend toward lower risk of CHD and total CVD that attained statistical significance after the exclusion of a single cohort (RR 0.93; p=0.03 and RR 0.74; p=0.0037).
In all of the populations studied in the present meta-analysis, potassium intake was far lower than the recommended intake of 100 mmol or more per day, they note.
The Italian doctors say the protective effect of potassium against stroke is in part due to its BP-lowering effects, particularly in hypertensive individuals and in those with elevated sodium intake, but also likely due to other properties of the mineral, such as the inhibition of free radical formation, as demonstrated in experimental studies.
Increasing potassium=reducing salt: Prevent one million strokes/year
They add that the magnitude of risk reduction with increasing potassium intake by 1.64 g per day is similar to that which would result from lowering dietary sodium consumption by 5 g (85 mmol) per day and would translate "into a reduction of 1 155 000 stroke deaths per year on a worldwide scale."
Not sure what I'll do about this except add this to my questions to my cardiologist.
tumeric and stroke rehab
http://www.sify.com/news/compound-derived-from-turmeric-has-neuroprotective-effects-news-scitech-kmqk4dagfjh.html
Two new studies suggest that a compound derived from curry spice turmeric may have clinical promise for ischemic stroke and traumatic brain injury (TBI), which currently lack good therapies.
A synthetic derivative of turmeric, made by scientists at the Salk Institute for Biological Studies, dramatically improved the behavioral and molecular deficits seen in animal models of these conditions.
In previous studies, David R. Schubert, and Pamela Maher in the Salk Cellular Neurobiology Laboratory had developed a series of new compounds using a novel drug discovery paradigm that starts with natural products derived from plants; it then calls for selecting synthetic derivatives that show efficacy in multiple assays testing protection against various aspects of the nerve cell damage and death that occur in brain injuries and in age-associated neurodegenerative diseases.
One compound, called CNB-001, which was derived from curcumin, the active ingredient in the spice turmeric, proved highly neuroprotective in all of the assays; it also enhanced memory in normal animals.
While the Salk group has a great deal of expertise in age-associated neurological diseases such as Alzheimer's, they do not run animal models of TBI and stroke.
"To test the prediction that drugs from our new drug discovery scheme will work in multiple models of CNS disease and trauma," Schubert explains, "we undertook a series of experiments to assay the drugs in collaboration with researchers at Cedars-Sinai and UCLA, who are leaders in the fields of stroke and TBI, respectively, and appreciate the potential for therapeutics based on natural products and their derivatives."
Employing the same animal model of stroke that was used to develop TPA, Paul Lapchak, of the Department of Neurology at the Burns and Allen Research Institute at Cedars-Sinai Medical Center in Los Angeles, collaborated with Schubert's team in a study that showed that CNB-001 was at least as effective as TPA in preventing the behavioral deficits caused by stroke.
The study, published in the Dec. 2, 2010 edition of the Journal of Neurochemistry, also demonstrated that unlike TPA, which reduces clotting in the blood vessels of the brain, the Salk compound has a direct protective effect on nerve cells within the brain. Maher has found that it maintains specific cell signaling pathways required for nerve cell survival.
Similarly, in a study to be published in early 2011 in Neurorehabilitation and Neural Repair, Fernando Gomez-Pinilla, and his colleagues in the Department of Physiological Science and Division of Neurosurgery at the University of California, Los Angeles used a rodent model of TBI to demonstrate that CNB-001 dramatically reversed the behavioral deficits in both locomotion and memory that accompany the brain injury.
As with stroke, CNB-001 was again found to maintain the critical signaling pathways required for nerve cell survival, as well as the connections between nerve cells that are lost with the injury.
The results of these two studies, which used two distinct models of brain injury, indicate that the Salk compound has clinical potential in conditions where there is currently no effective treatment. (ANI)
via sify.com
You know the drill, don't even think of self-treatment.
Two new studies suggest that a compound derived from curry spice turmeric may have clinical promise for ischemic stroke and traumatic brain injury (TBI), which currently lack good therapies.
A synthetic derivative of turmeric, made by scientists at the Salk Institute for Biological Studies, dramatically improved the behavioral and molecular deficits seen in animal models of these conditions.
In previous studies, David R. Schubert, and Pamela Maher in the Salk Cellular Neurobiology Laboratory had developed a series of new compounds using a novel drug discovery paradigm that starts with natural products derived from plants; it then calls for selecting synthetic derivatives that show efficacy in multiple assays testing protection against various aspects of the nerve cell damage and death that occur in brain injuries and in age-associated neurodegenerative diseases.
One compound, called CNB-001, which was derived from curcumin, the active ingredient in the spice turmeric, proved highly neuroprotective in all of the assays; it also enhanced memory in normal animals.
While the Salk group has a great deal of expertise in age-associated neurological diseases such as Alzheimer's, they do not run animal models of TBI and stroke.
"To test the prediction that drugs from our new drug discovery scheme will work in multiple models of CNS disease and trauma," Schubert explains, "we undertook a series of experiments to assay the drugs in collaboration with researchers at Cedars-Sinai and UCLA, who are leaders in the fields of stroke and TBI, respectively, and appreciate the potential for therapeutics based on natural products and their derivatives."
Employing the same animal model of stroke that was used to develop TPA, Paul Lapchak, of the Department of Neurology at the Burns and Allen Research Institute at Cedars-Sinai Medical Center in Los Angeles, collaborated with Schubert's team in a study that showed that CNB-001 was at least as effective as TPA in preventing the behavioral deficits caused by stroke.
The study, published in the Dec. 2, 2010 edition of the Journal of Neurochemistry, also demonstrated that unlike TPA, which reduces clotting in the blood vessels of the brain, the Salk compound has a direct protective effect on nerve cells within the brain. Maher has found that it maintains specific cell signaling pathways required for nerve cell survival.
Similarly, in a study to be published in early 2011 in Neurorehabilitation and Neural Repair, Fernando Gomez-Pinilla, and his colleagues in the Department of Physiological Science and Division of Neurosurgery at the University of California, Los Angeles used a rodent model of TBI to demonstrate that CNB-001 dramatically reversed the behavioral deficits in both locomotion and memory that accompany the brain injury.
As with stroke, CNB-001 was again found to maintain the critical signaling pathways required for nerve cell survival, as well as the connections between nerve cells that are lost with the injury.
The results of these two studies, which used two distinct models of brain injury, indicate that the Salk compound has clinical potential in conditions where there is currently no effective treatment. (ANI)
via sify.com
You know the drill, don't even think of self-treatment.
Niacin aids stroke recovery
I'm not sure how much I trust this since the last line in the URL refers to Neuroaid(I deleted that line from the post) Read up what I think about Neuroaid here
http://www.massagebyben.com/articles/articledetail.php?artid=22396&catid=272
Studies show that Vitamin B3 aids stroke recovery, this was revealed by Henry Ford Neuroscience Institute's director Dr. Michael Chopp last February during the International Stroke Conference held in Texas.
Commonly known as Niacin, Vitamin B3 releases energy from carbohydrates, proteins, and fats so that these can be used by the body. This way, it helps control blood sugar levels, keeps skin healthy, and maintains proper functioning of the digestive and nervous systems. It is useful in the treatment of osteoarthritis and prevent diabetes or delay the need for insulin.
Niacin's role in stroke prevention is one of the new discoveries in terms of benefits. It prevents stroke, particularly ischemic stroke due to atherosclerosis, because regular intake of Vitamin B3, which is commonly found in most of the food we consume daily, actually helps increase good cholesterol in the blood and reduces arterial plaque. A fact most beneficial if combined with Vitamin A and E than Niacin alone, according to research.
Now, Niacin's role in stroke care is increasing as the study of Dr. Chopp seem to indicate. The study involved rats induced with ischemic stroke and given niacin, which in turn revealed an increase in nerve cells and blood vessels. The study indicates that Niacin helps restore neurological functions after stroke.
Dr. Chopp's team observed that the brains of the ischemic stroke-induced rats showed growth of new blood cells, sprouting of nerve cells, and improved neurological outcomes after these were given Niacin. Thus, they found that Niacin helps restore neurological function in the brain of animals following a stroke by rewiring the brain.
However, since testing of its benefits on stroke treatment is still in animal level, human testing is still needed before Niacin can be proven effective in treating stroke. They are now in the process of conducting human trials through an extended-release form of Niacin in stroke patients.
Their study also confirmed the effectivity of Niacin to increase High-Density Lipoprotein-Cholesterol (HDL-C) in the blood, also known as the good cholesterol, which helps get rid of fatty deposits in arterial walls that lead to atherosclerosis. Niacin's increasing of HDL-C in the blood also increased blood vessels in the brain and axonal and dendritic growth leading to a substantial improvement of neurological function.
Niacin is a water-soluble vitamin that can be found in red meat, poultry, potatoes, yoghurt, pasta, fish, nuts, milk, eggs, and foods fortified with it such as breads and breakfast cereals.
Studies show that Vitamin B3 or Niacin aids stroke recovery by rewiring the brain and recreating aspects of it. While studies such as these are still underway for human trial, the fact remains that, as of this time, Vitamin B3 or Niacin is still best for stroke prevention.
I am taking Niacin now for some part of my cholesterol. Some day a researcher will evaluate all the various acute therapies and come up with a standard protocol for each hour since the event.
http://www.massagebyben.com/articles/articledetail.php?artid=22396&catid=272
Studies show that Vitamin B3 aids stroke recovery, this was revealed by Henry Ford Neuroscience Institute's director Dr. Michael Chopp last February during the International Stroke Conference held in Texas.
Commonly known as Niacin, Vitamin B3 releases energy from carbohydrates, proteins, and fats so that these can be used by the body. This way, it helps control blood sugar levels, keeps skin healthy, and maintains proper functioning of the digestive and nervous systems. It is useful in the treatment of osteoarthritis and prevent diabetes or delay the need for insulin.
Niacin's role in stroke prevention is one of the new discoveries in terms of benefits. It prevents stroke, particularly ischemic stroke due to atherosclerosis, because regular intake of Vitamin B3, which is commonly found in most of the food we consume daily, actually helps increase good cholesterol in the blood and reduces arterial plaque. A fact most beneficial if combined with Vitamin A and E than Niacin alone, according to research.
Now, Niacin's role in stroke care is increasing as the study of Dr. Chopp seem to indicate. The study involved rats induced with ischemic stroke and given niacin, which in turn revealed an increase in nerve cells and blood vessels. The study indicates that Niacin helps restore neurological functions after stroke.
Dr. Chopp's team observed that the brains of the ischemic stroke-induced rats showed growth of new blood cells, sprouting of nerve cells, and improved neurological outcomes after these were given Niacin. Thus, they found that Niacin helps restore neurological function in the brain of animals following a stroke by rewiring the brain.
However, since testing of its benefits on stroke treatment is still in animal level, human testing is still needed before Niacin can be proven effective in treating stroke. They are now in the process of conducting human trials through an extended-release form of Niacin in stroke patients.
Their study also confirmed the effectivity of Niacin to increase High-Density Lipoprotein-Cholesterol (HDL-C) in the blood, also known as the good cholesterol, which helps get rid of fatty deposits in arterial walls that lead to atherosclerosis. Niacin's increasing of HDL-C in the blood also increased blood vessels in the brain and axonal and dendritic growth leading to a substantial improvement of neurological function.
Niacin is a water-soluble vitamin that can be found in red meat, poultry, potatoes, yoghurt, pasta, fish, nuts, milk, eggs, and foods fortified with it such as breads and breakfast cereals.
Studies show that Vitamin B3 or Niacin aids stroke recovery by rewiring the brain and recreating aspects of it. While studies such as these are still underway for human trial, the fact remains that, as of this time, Vitamin B3 or Niacin is still best for stroke prevention.
I am taking Niacin now for some part of my cholesterol. Some day a researcher will evaluate all the various acute therapies and come up with a standard protocol for each hour since the event.
Subscribe to:
Posts (Atom)